-
M-1 - PHI Pharmacist : BASICS OF TB AND NTEP
Fullscreen-
PHI-Pharmacist: TB and TB Epidemiology
FullscreenTuberculosis
Content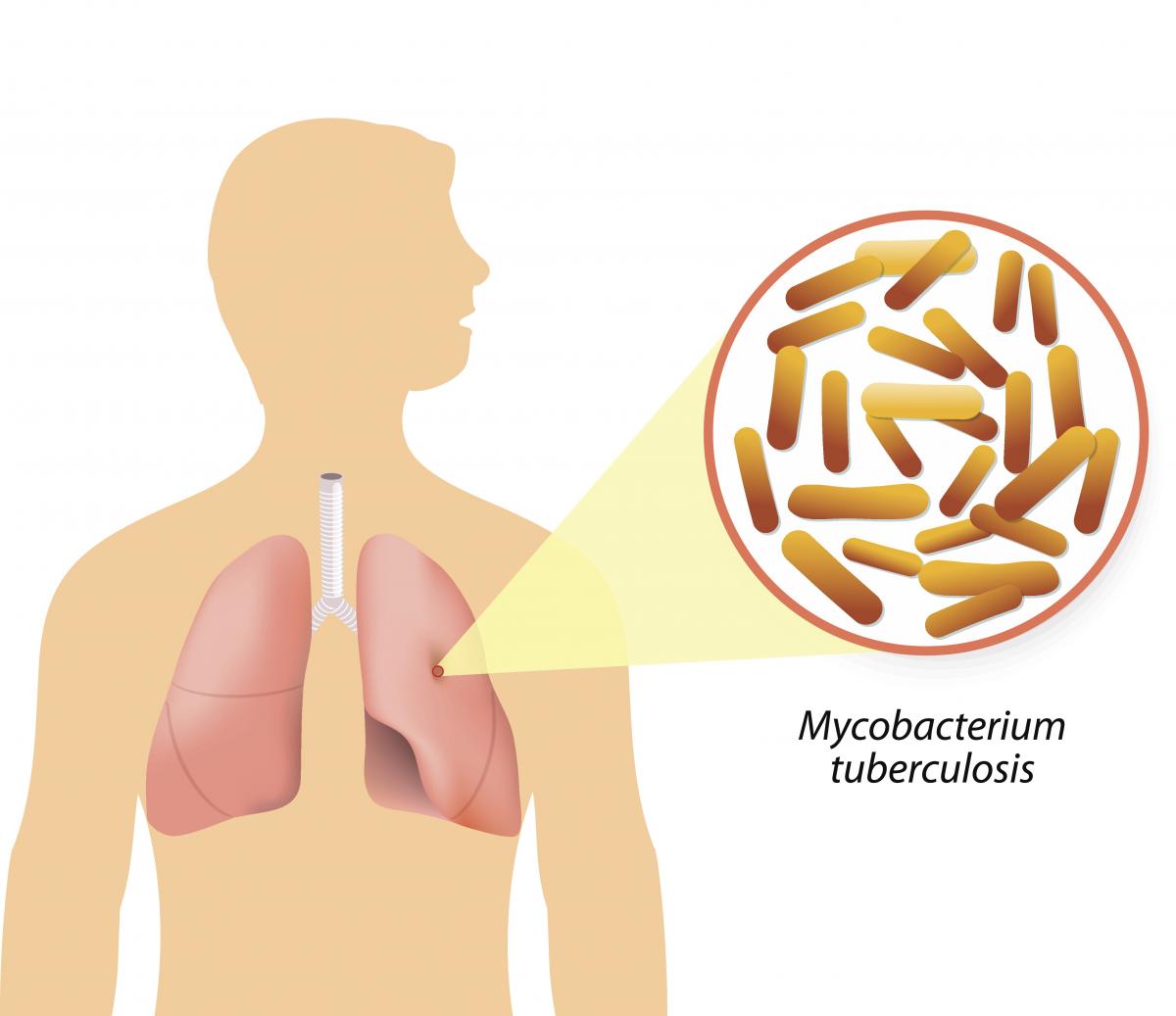
Figure: Causative agent for Tuberculosis is Bacillus: Mycobacterium tuberculosis (M.tb)
-
Tuberculosis (TB) is a communicable disease that is a major cause of ill health.
-
TB is caused by the bacillus Mycobacterium tuberculosis (M.tb)
-
TB disease typically affects the lungs (pulmonary TB) (80%) but can also affect other parts of the body (extra pulmonary TB) (20%)
-
It spreads when people who are sick with TB expel bacteria into the air (for example by coughing, sneezing, shouting or singing)
-
It is one of the top 10 causes of death worldwide and the leading cause of death from a single infectious agent
Resources
- Global Tuberculosis Report, 2020; Geneva: World Health Organization, 2020
- Training Modules (1-4) for Programme Managers and Medical Officers India: Central TB Division, MoHFW, Government of India,July 2020
-
Global Burden of TB
Content- Globally, an estimated 11 million people fell ill with TB (incidence) in 2021.
- Historically, it has been the top infectious disease killer. In 2021, there were an estimated 1.4 million TB deaths and an additional 187 000 deaths among HIV-positive people.
- Three countries accounted for 42% of global cases in 2021: India (26%), the Russian Federation (8.5%) and Pakistan (7.9%).
Image
Figure: Estimated TB incidence in 2021, for countries with at least 100 000 incident cases; Source: Global TB Report, 2022.
Resources
Burden of TB in India
ContentTB is one of the top burdensome infectious diseases in India. It is estimated that, around 1/4th (26%) of the world's TB cases are in India, translating to about 30 Lakhs new TB cases emerging each year (TB incidence). Against this estimated incidence the National TB Elimination program reported around 19 lakh new and relapse cases in the year 2021.
An estimated 5 Lakhs deaths occur due to TB each year in the country, translating to about 1 case of TB death every one-two minutes. Compared to this, there are only about 60 thousand deaths due to HIV and about 77 deaths due to Malaria each year.
TB diagnosis and treatment services although provided free of cost in the public sector, the cost of accessing these services and related loss of wages drive the affected people with poverty (catastrophic costs). TB also has a huge impact on the world's and the country's economy because of loss of workdays (100 million workdays per year).
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test What is the estimated number of incident TB cases that emerge each year in India? 35 Lakh cases 26 Lakh Cases 26% of the Global Burden 19 Lakh Cases 2 The estimated number of new and relapse (incident) cases in India that emerge each year is about 26 Lakh Yes Yes How many cases of deaths are estimated to be caused by TB in India Approximately One death every 2-3 minutes Approximately 5 Lakh deaths 60 Thousand deaths each year 1 and 2 4 In India it is estimated that there is around one death caused due to TB every one to two minutes, translating to about 5Lakh deaths each year in India Yes Yes Resources:
TB Causative organism
Content
Figure Mycobacterium tuberculosis
TB is caused due to the infection by a bacterium called Mycobacterium tuberculosis.

Figure: Extra-Pulmonary Tuberculosis
It often affects the lungs, and in such cases it is called Pulmonary Tuberculosis. But, it can affect almost any part of the body (except the hair and the nails), in which it is known as Extra-Pulmonary Tuberculosis.
Resources:
Mode of TB Transmission
ContentTuberculosis is transmitted mainly through the air via droplet nuclei generated when a TB patient coughs or sneezes.
It is estimated that every sputum smear-positive patient spreads the infection to 10 – 15 persons annually, if untreated..

Figure: Transmission of TB bacteria through air via droplet
Resources:
- Technical and Operational Guidelines for TB Control in India 2016
- WHO - Fact sheet details on Tuberculosis
Kindly provide your valuable feedback on the page to the link provided HERE
Determinants of TB Disease
ContentDeterminants are any characteristics that affect the health of a patient.
Biological Determinants Behavioral Determinants Socio Economic Determinants Occupational Determinants - People living with HIV(PL HIV)
- History of contact with a case of TB
- People with underlying medical conditions like Diabetes, Kidney disease, Cancer etc.
- Existing lung disease
- Old age
- Use of tobacco and alcohol
- Malnutrition
- Person in contact with TB infected patient
- Person living in areas with poor ventilation & over crowding
- Poverty and Malnutrition
- Homeless
- Mining work
- Quarry work(Silicosis)
- Construction work
- Migrant worker
- Daily wagers
Vulnerable Population for Tuberculosis
ContentTB can affect anyone but it is more prevalent in some communities which are vulnerable to TB disease due to various factors which are mentioned below:
Increased exposure of TB due to where they live or work
- prisoners
- slum dwellers
- miners
- hospital visitors
- healthcare workers
Limited access to Quality TB services
- Migrant workers
- Women in settings with gender disparity,
- Children
- Physically challenged
- Transgender population
- Tribal and population living in hard to reach areas
- Refugees or internally displaced people
- Illegal miners and undocumented migrants
Increased risk because of biological or behavioural factors that compromise immune functions in people who:
- People who live with HIV
- have diabetes or silicosis
- undergo immunosuppressive therapy
- are undernourished
- use tobacco
- suffer from alcohol use disorders.
- inject drugs
TB Infection
Content-
TB Infection (or previously known as Latent TB infection) is a stage in between uninfected and having active TB. In this stage the person has no symptoms and can only be identified using laboratory tests.
-
The vast majority of infected people may never develop TB disease. However, to achieve TB elimination, it is important to treat TB infection in people at risk of developing active TB disease.
-
It is a state of persistent immune response to stimulation by Mycobacterium tuberculosis antigens with no evidence of clinically manifested active TB.
-
There is no single acceptable/reliable test for direct identification of Mycobacterium tuberculosis infection in humans. Tuberculin Skin Test (TST) and Interferon-gamma release assay (IGRA) are commonly used tests for identifying TB infection.
Resources:
-
Progression to TB Disease
ContentAfter exposure to infective droplets containing M.TB, only a small proportion gets infected and further progresses to active TB disease.
- Majority of those that get infected persist in a stage of clinical latency known as TB infection (previously known as Latent TB infection). They do not have TB disease and do not show any symptoms of TB and no evidence of any TB related changes on chest X-ray.
- A small proportion of those with prior infection may progress to active TB disease due to various environmental/ agent/ host factors.

Figure: Flow chart for TB disease progression
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
TB Infection Vs Active TB Disease
ContentTB Infection Active TB Disease May not have any signs & symptoms Has sign and symptoms such as cough for more than two weeks, fever, weight loss and blood in sputum Has dormant, contained bacteria is the body Has active, multiplying bacteria in the body Doesn't spread TB bacteria to others May spread TB bacteria to others Chest X-ray usually normal Lesion in Chest X- ray (usually) May advance to active TB. It is estimated that the lifetime risk of an individual with TB infection for progression to active TB is 5–10%. Needs treatment for TB disease Resources:
Chemotherapy and its implication in TB control
ContentChemotherapy for TB is the use of an anti-TB drugs to kill, or prevent the replication of, TB mycobacteria in the patient’s body. Effective anti-TB chemotherapy renders the patient non-contagious and cures the patient, thereby interrupting the chain of transmission. Mortality rates of TB range from 50-80% in untreated smear-positive individuals and drop to lower than 5% under chemotherapy.
Most of the bacteria are killed during the first 8 weeks of treatment; however, there are persistent organisms that require longer treatment. TB disease must be treated for at least 6 months and in some cases even longer. The use of multi-drug therapy reduces the incidence of drug-resistant cases and increases the overall effectiveness of treatment.
If treatment is interrupted, any surviving bacteria may cause the patient to later become ill and infectious again, potentially with drug-resistant disease.
How infectious are tuberculosis patients under chemotherapy?
Under effective chemotherapy, there is a substantial decline in infectiousness in two weeks time, and may not be a major source of risk to any contacts. This decline is indicated by the rapid fall in the number of viable organisms in the sputum, and reduced frequency of coughing.
Types of Chemotherapy in TB
- Preventive Chemotherapy: Regimen for healthy but TB infected persons with a high risk of developing TB, in order to prevent them from developing TB.
- Standard Chemotherapy: Two-phased chemotherapy for an average of 6-8 months based on the combination of at least four major drugs (HRZE) given for 2 months during the initial intensive phase of treatment and followed by a combination of at least 2 drugs given for at least 4 months during the continuation phase of treatment.
- Chemotherapy for Drug-resistant TB: Two-phased chemotherapy varying from 9 - 24 months in patients having demonstrated resistance to drugs used in standard chemotherapy. The regimen varies with the drug to which the resistance is present, however, each regimen contains a mix of second-line anti-TB drugs including injectables.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Tuberculosis Infectiousness and Host Susceptibility, The Journal of Infectious Diseases, Vol. 216, suppl_6, 2017.
- Tuberculosis chemotherapy: Current Drug Delivery Approaches, Respiratory Research 7, Article no. 118, 2006.
- Tuberculosis Case-finding and Chemotherapy: Questions and Answers, K. Toman.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which type of chemotherapy regimen of anti-TB drugs is used for infected persons with a high risk of developing TB who have no signs or symptoms of active disease, in order to prevent them from developing TB? First-line anti-TB drugs Preventive Chemotherapy Standard Chemotherapy Chemotherapy for Drug Resistant-TB 2 Preventive chemotherapy regimen of anti-TB drugs is used for infected persons with a high risk of developing TB who have no signs or symptoms of active disease, in order to prevent them from developing TB. Yes Yes Prevention of TB
ContentAs TB is an airborne infection, TB bacteria are released into the air when someone with infectious TB coughs or sneezes. The risk of infection can be reduced by taking simple precautions:
Figure: Measures for control and prevention of tuberculosis
TB Preventive Treatment(TPT) also has a very important role in prevention of TB. Presently, household contacts of sputum-positive TB patients are given TPT upon confirmation of TB infection and ruling our active Tuberculosis.
Resources:
-
Ph-Ch2: NTEP
FullscreenEvolution of TB Elimination Programme in India
ContentThe National Tuberculosis Control Program (NTP) of India was launched in 1962. It relied on BCG, X-ray based diagnosis and Streptomycin and INH based treatment centralized at district level.
Based on a review of the NTP, and WHO recommendations of the DOTS Strategy, Government of India then revised the NTP and launched new program with the title Revised National Tuberculosis Control Program (RNTCP) in 1997. It used Sputum microscopy at DMC(Designated Microscopy Centres) for diagnosis, and multi-drug Short Course Anti-TB Therapy, decentralized to the TU (TB Unit) level.
In recognition of the rising drug resistance problem the DOTS Plus/ PMDT (Programmatic Management of Drug Resistant TB) was launched in 2006 and scaled up to the entire country by 2012.
Further to strengthen the monitoring and supervision system - a case based notification system - Nikshay was introduced in 2012. The same year Tuberculosis was added as a notifiable disease at the point of diagnosis by all health care providers.
Other key milestones from 2012 to 2020 were the availability of the Standards of TB Care in India (STCI) in 2014, introduction of the Daily weight band wise Fixed Dose combination (FDC) in 2016 and new drugs like Bedaquilline and Delaminid were started in 2017 and 2018 respectively.
To emphasise the commitment of the Government of India and to accelerate the efforts towards TB elimination, RNTCP was renamed as "National Tuberculosis Elimination Programme (NTEP)" in 2020.

Figure: Key milestones under NTEP
Resources:
India's commitment to End TB
ContentThe Government of India has committed to achieving the Sustainable Development Goals(SDG) targets related to ending TB by 2025 (5 years ahead of the global target). This would mean that in 2025, the 2030 target of achieving 80% reduction in incidence, 90% reduction in deaths due to TB compared to that of 2015, is to be achieved.
Parameter 2015 Value SDG 2030 Target Commitment for 2025 Estimated annual Incidence 217 cases/Lakh 80% reduction 44 cases/lakh Estimated annual Mortality 4.5 lakh 90% reduction 45,000 Table: India's commitment to End TB by 2025.
Resources:
NTEP Objectives- in relation to NSP 2017-2025
ContentNSP 2012 - 2017 had the aim of achieving universal access to quality diagnosis and treatment. The NSP 2017-2025 which builds on the success and learnings of the last NSP, and articulates the bold and innovative steps required to move towards TB elimination. In 2020, RNTCP was renamed to "National Tuberculosis Elimination Programme" with the following objectives:

Figure: Objectives of NTEP
Resources:
Organizational Structure of NTEP
ContentNational Tuberculosis Elimination Programme (NTEP) is a centrally sponsored programme being implemented under the aegis of National Health Mission.
National Level: Managed by Central TB Division (CTD), the technical arm of the Ministry of Health and Family Welfare (MOHFW)
State Level: State TB Cell coordinates the overall TB elimination programme in state under the guidance of State Health Society. The training ,supervision, monitoring and evaluation NTEP at state level are looked after by STDC (State TB Training and Demonstration Centre).
District TB Centre (DTC) is the nodal point for all TB elimination activities in the district under the guidance of the District Health Society.
Tuberculosis Unit (TU) Level: NTEP activities at block/sub-district level are implemented through TU which comprises Designated Medical Officer (MO) supported by two full-time NTEP staff - STS (Senior Treatment Supervisor) & STLS (Senior TB Lab Supervisor).
PHI (Peripheral Health Institute): PHI is a health facility manned by a Medical Officer (MO). Some of the PHIs are also the Tuberculosis Diagnostic Centres, which are the most peripheral level laboratories in the NTEP structure. All the Private Health Facilities like Private Practitioners / Private Hospitals / Clinics / Nursing Homes are also PHI.

Figure: Organisational structure of NTEP
Resources:
The State TB Cell
ContentThe State TB Cell or STC is the state-level implementing structure of the National TB Elimination Program (NTEP). It is the leading institution for management of NTEP activities at the state level.
The STC is a State Government entity that acts as the bridge between the Central and State Governments for implementing the NTEP. It works under the guidance of the Central TB Division (CTD), and it oversees the program implementation at the districts.
- The State TB Cell is supported by the State TB Training and Demonstration Centre (STDC) for its technical functionalities. STDC mainly supports training, supervision and monitoring.
- The nodal laboratory for the State is the Intermediate Reference Laboratory (IRL). This supports quality assurance of the smear microscopy network and laboratory services in the state.
- The STC has a fully operational State Drug Store (SDS) which is responsible for the effective management and uninterrupted supply of good-quality of medicines and other logistics.
Human Resources at the State TB Cell are:
- State Tuberculosis Officer (STO). A dedicated official from the state health system, at the rank of a Joint Director is designated as the STO and heads the implementation of the NTEP at state level.
- Medical Officer STC (MO-STC): A medical officer from the state health system assists the STO in overseeing various activities.
- State DRTB Coordinator: Assist the STO in DRTB activities monitoring across the districts
- TB - HIV Coordinator: Assist the STO in overseeing TB comorbidities across the district.
- State PPM Coordinator: Looks at the private sector engagement
- State IEC Officer/ACSM Officer: Oversees the implementation of advocacy, communication and social mobilisation activities across different districts.
- STC - Epidemiologist: Assist the STO and STDC Directors by analyzing state-level data and preparing review materials
- Other support staff at the STC include
- Accounts Officer
- Technical Officer-PSM
- Secretarial Assistant
- Data entry operators/Nikshay operator
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Training Modules (5-9) for Programme Managers and Medical Officers, 2020.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following statements are true about the State TB Cell (STC)? STC is a state government entity. It is the leading institution for the management of NTEP activities at the state level. It is supported by the STDC. All of the above 4 The STC is a state government entity that is the leading institution for the management of NTEP activities at the state level and is supported by the STDC. Yes Yes State TB Training and Demonstration Centre [STDC]
ContentThe State Tuberculosis (TB) Cell (STC) is supported by the State TB Training and Demonstration Centre (STDC) in many states through its three units – Training Unit, Supervision and Monitoring Unit and an Intermediate Reference Laboratory (IRL). This relationship is shown in the figure below.
- Training Unit: It is involved in estimating the training load, organizing state level training (Induction and Refresher) and evaluating the performance of those who undergo training.
- Supervision and Monitoring Unit: It consists of a team which is dedicated to the supervision of TB elimination activities through supervisory visits, periodic desk review of Nikshay and Nikshay Aushadhi data, and plans state internal evaluations apart from assisting in other supervision and monitoring activities of National Reference Laboratories, Central TB Division and other national/international monitoring missions.
- Intermediate Reference Laboratory: This supports an effective quality assurance system of the sputum smear microscopy network and laboratory services for the programmatic management of drug-resistant TB (molecular drug resistance and culture and drug susceptibility testing) in the state.
The STDC is also involved in operational research.
Human Resources in the STDC
- The STDC functions under the leadership of STDC Director.
Training and Supervision & Monitoring Units:
- 1 Epidemiologist
- 1/more Medical Officer
- 1 Nikshay Operator
- 1 Secretarial Assistant
Intermediate Reference Laboratory (IRL):
- 1 Microbiologist
- 1 Microbiologist- External Quality Assistance (EQA)
- 1 Senior Laboratory Technician- EQA
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Training Modules (5-9) for Programme Managers and Medical Officers, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
District TB Centre [DTC]
ContentThe key level for the management of public health services is the district level. The District Tuberculosis Centre (DTC) is the nodal point for tuberculosis (TB) control activities in the district.
Functions of the DTC
The primary role of the DTC is a managerial one. The DTC is the central program management unit of the district responsible for all activities related to National TB Elimination Programme (NTEP) implementation such as:
- Advocacy
- Active case finding
- Diagnosis, treatment (both for drug-susceptible and drug-resistant TB cases) and follow up
- Managing comorbidities
- Service delivery
- Maintaining diagnostic and treatment infrastructure
- Setting up Drug-resistant TB (DR-TB) centres
- Ensuring community engagement and TB forums
- Multi-sectorial involvement for drug management, and supervision and monitoring
- Financial management
- Drugs, logistics and supply chain management.
Components of the DTC
- District Drug Store (DDS)
- Nucleic Acid Amplification Test machine (Cartridge Based NAAT or TrueNAT)
- Designated Microscopic Center (DMC)
- Treatment Support Center
- Drug Resistant TB (DR-TB) Center
- X-Ray Unit
With expansion of TB services and ongoing collaboration with various national programs, the structure of DTC is highly integrated as part of general health system and some components may cater to non-TB patients as well e.g., the DMC may be a part of general laboratory, and X-ray unit can be functional for all departments and not just chest/TB section.
Human Resources Deployed at the DTC
The Chief District Health Officer (CDHO) / Chief District Medical Officer (CDMO) / Civil Surgeon or an equivalent functionary in the district is responsible for all medical and public health activities including control of TB.
A full-time District TB Officer (DTO), trained at the national level and based at the DTC, is responsible for planning, training, supervising and monitoring the programme in the district. The DTO is assisted by other technical and secretarial staff:
- Medical Officer- District TB Center
- District DR-TB-HIV Coordinator
- District Public Private Mix Coordinator
- District Program Coordinator
- District Drug Store Pharmacist
- District Data Entry Operator-Nikshay
- District Accountant
- Senior TB laboratory Supervisor
- Senior Treatment Supervisor
- Laboratory Technicians for DMC and NAAT site
- Counsellor for District DR-TB center
- TB Health Visitors
While the National TB Elimination Program (NTEP) approves the above positions through National Health Mission NTEP Project Implementation Plan, the district always has the flexibility for additional resource deployment based on the need and existing epidemic. The DTO and his/her team are supported by various other program officers/staff and non-governmental organizations working in the field for Tuberculosis and Health.
Resources
- NTEP Training Modules 1-4 for Programme Managers & Medical Officers, 2020.
- NTEP Training Modules 5-9 for Programme Managers & Medical Officers, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Tuberculosis Unit [TU]
ContentTuberculosis (TB) unit (TU) is the sub-district level supervisory unit of National TB Elimination Program with the following organogram:
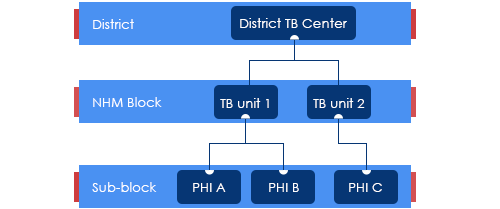
Figure: Organogram of a TB Unit
(PHI: Peripheral Health Institution)
TUs are based mainly on National Health Mission (NHM) health blocks with the aim of aligning with the NHM Block Programme Management Unit (BPMU) for optimum resource utilization and appropriate monitoring.
The TUs have been created based on a population of 1 per 2,00,000 (range 1.5 – 2.5 lakh) for rural and urban populations and 1 per 1,00,000 (0.75 – 1.25 lakh) population in hilly/tribal/difficult areas.
The TU consists of a designated Medical Officer-Tuberculosis Control (MO-TC), as well as one full-time supervisory staff - Senior Treatment Supervisor (STS). However, one Senior TB Laboratory Supervisor (STLS) will be there in every 5 lakh population (one per 2.5 lakh population for tribal/hilly/difficult areas), mostly covering 2-3 TUs.
TB Unit manages the provision of TB services (Diagnosis, Treatment, Prevention, etc.) and programme management in the assigned geographical area.
Resources
Peripheral Health Institutions [PHI] and Health Facilities
ContentUnder the National Tuberculosis Elimination Programme (NTEP), a Peripheral Health Institute (PHI) is a health facility that is manned by at least a Medical Officer (MO), where diagnosis and management of Tuberculosis (TB) are done.
At this level, there are dispensaries, Primary Health Centres (PHCs), Community Health Centres (CHCs), referral hospitals, major hospitals, speciality clinics or hospitals (including other health facilities), TB hospitals, Anti-retroviral Treatment (ART) centres and medical colleges within the respective district.
All health facilities in the private and Non-government Organisation (NGO) sectors participating in NTEP are also considered PHIs. Some of these PHIs also function as Designated Microscopy Centres (DMCs).
Role of PHIs in Program Management for TB Elimination
- PHIs undertake tuberculosis case-finding and treatment activities as a part of the general health services.
- In situations where more than one MO is posted in any of the PHC, one of them may be identified and entrusted with the responsibilities of the NTEP.
- Additionally, NTEP provides 1 TB Health Visitor (TBHV) per one lakh urban population to support the urban TB control activities in urban settings/ medical colleges.
Resources
Drugs Stores in NTEP
ContentImage
DRUG STORE
Central TB Division, MoHFW, has
Under NTEP, there is a large network of drug stores across the country to ensure a regular and uninterrupted supply of drugs and consumables. The Drugs and consumables are procured at the Central level and supplied at Central warehouses (GMSDs & CMSS); further drugs and consumables are supplied to the State Drug Stores and further dissemination to district and sub-district levels following the stocking norms to ensure uninterrupted supply of drugs and consumables to the patient.
To provide overall policy guidance and coordination, the Procurement and Supply Chain Management (PSM) Unit has been established at Central TB Division (CTD), MoHFW, for procurement and Supply Chain Management of all types of anti-TB drugs, diagnostics and consumables.
Standards of TB Care in India
ContentThe Standards for TB Care in India (STCI), which is a locally customized version of the International Standards of Tuberculosis Care, mentions 26 standards that every citizen of India should receive irrespective of the sector of treatment.
STCI were developed based on a series of discussions involving various stakeholders including clinicians, public health specialists, community workers and patient advocates.
STCI represent what is expected for quality TB care from the Indian healthcare system including both public and private systems.
It was first published in 2014 and outlines standards across the four themes of TB diagnosis, TB treatment, public health action and social inclusion.
Following are the list of the 26 Standards:

Table 1: Categorisation of the Standards for TB Care in India, Source: Standards for TB Care in India, World Health Organisation, pp. 13-23
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test How many standards in TB care are described in the Standards of TB Care in India (STCI) 2014? 4 15 26 32 3 There are 26 standards for TB care under four major categories: diagnosis, treatment, public health actions and social inclusion. Yes Yes Stages in TB Patient's Lifecycle
ContentThose who are suspected of having TB disease are first screened for symptoms like cough and fever for more than 2 weeks, blood stained sputum and weight-loss. If found positive on screening, then TB patients are referred for testing to the nearest health facility. If diagnosed with TB, then they are subsequently initiated on treatment. The TB patients initiated on treatment are regularly monitored with the help of field staff or digital interventions like 99DOTS and MERM (Medication Event Reminder Monitor) technology. NTEP staff also ensures that the TB patients are regularly followed up on monthly basis till their treatment completion.

Figure: Patient Flow
Kindly provide your valuable feedback on the page to the link provided HERE
-
Ph-Ch3: Diagnostic Technologies
FullscreenTesting for TB diagnosis
ContentNational Tuberculosis Elimination Programme (NTEP) strives for all presumptive TB patients to be microbiologically confirmed. Under NTEP, the acceptable methods for microbiological diagnosis of TB are:
Sputum Smear Microscopy (for Acid Fast Bacilli - AFB): Sputum Smear microscopy is the primary tool which is reliable, inexpensive, easily accessible and rapid method of diagnosing PTB, where in the bacilli are demonstrated in the sputum. Two types:
-
Ziehl-Neelsen Staining
-
Fluorescence staining
Rapid diagnostic molecular test: Rapid molecular tests that use techniques like NAAT are very specific. They amplify the genomic material in the patient sample and hence enhances detection
-
Nucleic Acid Amplification Test (NAAT) e.g., GeneXpert, TrueNat
Figure: Genxpert Machine for CBNAAT
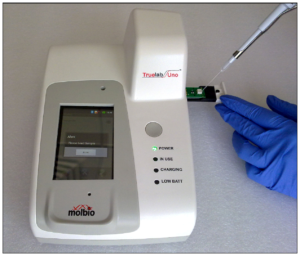
Figure: Truenat Machine
- Line Probe Assay
Culture and DST: A culture test involves studying bacteria by growing the bacteria on different substances. This is to find out if particular bacteria are present. In the case of the TB culture test, the test is to see if the TB bacteria Mycobacterium tuberculosis, are present.
Two types:
-
Solid (Lowenstein Jensen) media
-
Liquid media (Middlebrook) e.g., Bactec MGIT etc.
-
Microscopy
ContentMicroscopy is a TB diagnostic technology that utilizes the acid-fastness property of Mycobacterium tuberculosis to visualize it under a microscope. Results of sputum smear microscopy can either be smear-negative, or smear-positive (with various grades).
Advantages:
- It is currently the most accessible and cheapest TB diagnostic test available under National TB Elimination Programme (NTEP) in India.
- It has the shortest turnaround time for diagnosis.
- It has high specificity.
Limitations:
- Low sensitivity. It becomes positive only when more than 5000 bacilli/ml of sample are present. Hence, cases would be missed in early disease, or when an inappropriate biological specimen is provided, where bacterial load in sputum is less.
- It is unable to differentiate between M. tuberculosis and Non-tuberculous Mycobacteria (NTM). This is predominantly an issue in geographies with lower burden.
There are two types of microscopies used in NTEP: Ziehl-Neelsen (ZN) Microscopy and Fluorescence Microscopy (FM). These vary in the type of stain and microscope used. FM is newer of the two types and is currently recommended for use over ZN.
Resources
Cartridge Based Nucleic Acid Amplification Test [CBNAAT]
ContentCartridge Based Nucleic Acid Amplification Test (CBNAAT) is a rapid molecular diagnostic test. It is used for diagnosis of Tuberculosis (TB) and Rif-resistant Tuberculosis (RR-TB) in NTEP. Results are obtained from unprocessed sputum samples in about 2hours which helps in early detection and treatment of TB patients.
India has vast number of CBNAAT laboratories which are utilized for TB/RR-TB detection and Universal Drug Susceptibility Testing (UDST) under the National TB Elimination Program (NTEP).

Figure: CBNAAT Cartridge and Machine in Use (Image courtesy: USAID supported Challenge TB Project)
The CB-NAAT system detects DNA sequences specific for Mycobacterium tuberculosis complex and rifampicin resistance by Polymerase Chain Reaction (PCR). It concentrates Mycobacterium tuberculosis bacilli from sputum samples, isolates genomic material from the captured bacteria by sonication and subsequently amplifies the genomic DNA by PCR. The process identifies clinically relevant rifampicin resistance-inducing mutations in the RNA polymerase beta (rpoB) gene in the Mycobacterium tuberculosis genome in a real-time format using fluorescent probes called molecular beacons.
Video fileVideo: Cartridge-Based Nucleic Acid Amplification Test [CBNAAT] - GeneXpert Technology
Resources
- Training Module (1-4) for Program Managers and Medical Officers, NTEP, MoHFW, 2020.
- India TB Report 2021, National TB Elimination Program (NTEP), MoHFW, 2021.
Assessment Questions
Question
Answer 1
Answer 2
Answer3
Answer 4
Correct Answer
Correct explanation
Part of pre-test
Part of post-test
Under NTEP, CBNAAT is offered upfront for which of these categories?
PLHIV
Paediatric presumptive TB
Presumptive DR-TB
All of the above
4
Under NTEP, CBNAAT is recommended upfront for People living with HIV, Paediatric Presumptive TB patients, Presumptive DR-TB patients and patients notified from the Private sector.
Yes
Yes
CBNAAT requires the processing of sputum samples before testing
True
False
2
Results are obtained from unprocessed sputum samples in about 2hours from a CBNAAT machine
Yes
Yes
Intended Use of TrueNAT MTB and TrueNAT MTB Rif Dx Assay
ContentTrueNAT MTB and TrueNAT MTB Rif Dx Assay are intended to be used for detection of Mycobacterium tuberculosis bacteria (for TB diagnosis) and to detect resistance to rifampicin (Rif), respectively.
Positioning of TrueNAT MTB and TrueNAT MTB Rif Dx Assay
TrueNAT MTB and TrueNAT MTB Rif Dx Assay are suitable as point-of-care tests for use in peripheral laboratories and microscopy centres due to the following operational features:
- Biosafety requirements similar to smear microscopy
- Sample pre-treatment and preparation kits stable at 2-40°C, while TrueNAT chips stable between 2-30°C
- Test reagents with shelf life of 2 years
- Operates up to 8 hours on fully-charged batteries
- Temperature controlled operation, like air-conditioning, not required (operates up to ≤ 40°C)
- Operates under a wide relative humidity range (10-80%) & dusty conditions
- Portable and comes with a carrying case.
Target population
National TB Elimination Programme (NTEP) has defined the use of Nucleic Acid Amplification Test (NAAT) like Cartridge Based Nucleic Acid Amplification Test (CBNAAT) and TrueNAT as upfront tests for diagnosis of TB in presumptive paediatric TB, presumptive extra-pulmonary cases, People Living with HIV (PLHIV), smear negative X-ray suggestive of TB, contacts of Drug Resistant TB (DR-TB), treatment non-responders, TB affected patients retrieved after loss to follow-up and other vulnerable groups.
Resources
- Guidelines for Programmatic Management of Drug resistant Tuberculosis (PMDT) in India, 2021.
- Practical Guide to Implementation of TrueNAT Tests for the Detection of TB and Rifampicin Resistance.
Kindly provide your valuable feedback on the page to the link provided HERE
Line Probe Assay [LPA]
ContentLine Probe Assay (LPA) is a rapid molecular test available at centralised laboratories.
The assay is based on Polymerase Chain Reaction (PCR) that can simultaneously detect Mycobacterium tuberculosis complex as well as drug sensitivity to anti-TB drugs.

Figure 1: The GenoType MTBDRplus Molecular LPA Procedure; Source: Molecular Detection of Drug-resistant Tuberculosis by Line Probe Assay.
Advantages of LPA
- Rapid molecular test. (Turnaround time: 3-5 days)
- Highly sensitive and specific.
- Performed directly from sputum smear-positive specimens and on isolates of M. tuberculosis complex grown from smear-negative and smear-positive specimens.
- Detects multiple gene mutations in anti-TB drugs.
- First-line LPA detects mutations to rifampicin and isoniazid
- Second-line LPA detects mutations to fluoroquinolones and aminoglycosides.
- Suitable for low and high-throughput labs.
Disadvantages of LPA
- Cannot be used as a point-of-care test.
- Requires appropriate laboratory infrastructure, equipment and biosafety precautions.
- Different rooms (DNA extraction, pre-amplification, amplification, post-amplification/ hybridization) are required to perform different steps (Figure 2).
- Requires trained manpower to perform tests and interpret test results.
- Stringent internal quality control is required to prevent contamination.

Figure 2: Amplification (A) and Post-amplification Laboratory (B) for LPA; Source: Molecular Detection of Drug-resistant Tuberculosis by Line Probe Assay.
Resources
- Guidelines for PMDT in India, 2021.
- Molecular Detection of Drug-resistant Tuberculosis by Line Probe Assay.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test LPA can be used as a point-of-care test. True False 2 LPA cannot be used as a point-of-care test. Yes Yes Solid and Liquid Culture in TB
ContentCulturing TB Bacilli is well known and historic method for detection/ confirmation of Tuberculosis. It is a highly sensitive and specific phenotypic test; it can detect even a few viable bacilli in the sample (Upto 10 Colony Forming Units- CFUs). TB bacilli multiply in the culture and form colonies of TB bacilli which can are easily be identified.
Based on the growth media used Culture is divided in to two types, Solid and Liquid Culture methods. Types Culture:
- Solid Culture on Lowenstein Jensen media : Historic gold standard culture test. Results take usually upto 2 months (60 days).
- Modern Liquid culture systems: (e.g. BACTEC MGIT 960, BacT Alert or Versatrek etc.) Results take usually up to 42 days.
Uses
- Solid culture is the gold standard diagnostic test for TB. But it is not used for the purpose of TB diagnosis due to the long turn around time of 2 months. It is largely used for research purposes where it is used as the baseline test on which the sensitivity and specificity of other tests are calculated.
- Liquid Culture is being used for follow-up monitoring of patients on drug resistant TB treatment to detect treatment failure. Liquid culture is also used for long term follow up patients who have successfully completed treatment to detect recurrence.
- Liquid culture is used as a previous step to grow bacilli and obtain isolates prior to Drug Susceptibility Testing.
- Liquid cultures are also used in TB prevalence surveys for its high sensitivity and specificity
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Culture Drug Susceptibility Testing [CDST]
ContentCulture Drug Susceptibility Testing (CDST) is a growth-based phenotypic method used to check the susceptibility of Mycobacterium tuberculosis strains to various first and second line anti-TB drugs. Mycobacterial resistance to a particular drug is identified if there is growth observed in culture in presence of that drug.

In NTEP CDST is the standard method to detect resistance in samples of patients who have tested positive on followup. While CDST is possible on both Solid and Liquid culture, currently, the NTEP utilizes only liquid culture as a method for DST, due to faster Turn around times.
CDST testing services are available under NTEP in designated, specialized laboratories called CDST Labs both in public and private sector. Currently there are 80 such laboratories (60 certified for First Line and 49 for Second line drugs). Such designated laboratories are subject to regular external quality assessment, often by the National Reference Laboratory at that region.
Quality assured DST to R, H, Z, Mfx, Lfx, Lzd, Am, Km and Cm are available across the country.
Resources
-
Ph-Ch4: Approaches to TB Case Finding
FullscreenScreening For Tuberculosis Disease
ContentScreening for active tuberculosis (TB) a process to filter out people who are less likely to have TB, from a group. Screened positive people are likely to have TB and are confirmed subsequently using a TB diagnostic test. This will allow finite diagnostic testing resources to be used on the remaining.
Screening in TB may be performed using simple field tools (4 Symptom complex) and tests such as Chest X-ray, or a combination of both. Combination of both is the most effective, but is often not applied due to the practical difficulties in making a chest X-ray conveniently available.
Screening is an integral part of any general case finding effort. It is also applied systematically in specific situations.
- At health care facilities (intensified case finding): Here those visiting are screened using the 4 symptom complex, often at the point of entry to the facility. Those screened positive may be fast-tracked to TB Diagnostic testing.
- In vulnerable populations in active case finding efforts: Here the entire population identified for active case finding are screened using the pre-decided protocols by going door to door.
Resources
Active Case Finding
ContentSystematic screening of all individuals of a defined population is known as active case finding. It is applied outside of health facilities at the community level by the health system.
Objective of ACF is to:
- identify cases early, initiate prompt treatment, reduce risk of poor treatment outcomes and reduce risk of further transmission of TB
- to provide access to diagnosis services to populations that would have been otherwise unreached
It is effort intensive and is recommended only in population groups where there is estimated high case load. In NTEP, ACF is recommended only to be performed in Key / vulnerable population.
ACF can also be clubbed with suitable ACSM campaigns to create awareness about the signs and symptoms and about TB in the target population/ community. It can also be combined with other health activities/ campaigns (such as Pulse Polio/ Leprosy screening/ population based screening for NCDs) for increased efficiency.
Resources
- Training Modules for Programme Managers and Medical Officers.
- Active TB Case Finding, Guidance Document.
- WHO recommendations for Systematic Screening for Active Tuberculosis
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following is not a primary objective of ACF? Increase TB notification Early identification of cases. Reduce the risk of transmission of TB. Reduce the risk of poor treatment outcomes. 1 Notification is not a primary objective of ACF. Yes Yes
-
-
M-2: PHI Pharmacist: TB Treatment
Fullscreen-
Ph-Ch6: General concepts in TB Treatment
FullscreenGoals of treatment
ContentThe goals of tuberculosis treatment are:
-
Rendering the patient non-infectious, breaking the chain of transmission and decreasing the infection pool
-
Decreasing case fatality and morbidity by ensuring relapse-free cure
-
Minimising and preventing the development of drug resistance.
To meet the goals of treatment, the regimens should be:
- Safe, easy to administer and aid treatment adherence
- Long enough to achieve the long-term cure of the disease, and short enough to increase patient compliance.
Any treatment regimen which reduces the pill count but increases the overall treatment success is an ideal regimen to meet the goals of tuberculosis treatment.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
In what scenarios is a TB treatment regimen considered efficient?
High sputum conversion
High treatment success
Low emergence of drug resistance
All of the above
4
The goal of TB treatment ties in with how we consider a regimen efficient, and this occurs when the regimen results in high sputum conversion and treatment success, and low relapse rates and emergence of drug resistance.
-
Strategies for TB Treatment
ContentUnder the National TB Elimination Programme (NTEP), strategies adopted in the treatment of TB are based on the available scientific and operational researches. These strategies are combined to ensure better treatment outcomes for the TB patients. The main strategies include:
Domiciliary Treatment
- This is a strategy that allows for the treatment of TB in a patient’s home.
- Domiciliary chemotherapy proved to be as effective as sanatoria treatment (which was the historical way of treating TB) and achieved higher cure rates.
- The patients having the social benefits of being at home.
Short Course Chemotherapy (SCC)
- Chemotherapy of TB underwent revolutionary changes in the 70s owing to the availability of two well-tolerated and highly effective drugs – rifampicin and pyrazinamide.
- These drugs allowed for SCC and made it possible to simplify treatment and reduce its duration without reducing the therapeutic effect.
- Now with SCC regimens, it is possible to treat and cure TB patients in 6 months.
- When given daily, these regimens are effective, achieve high cure rates, prevent the emergence of drug resistance and minimize relapses.
- The shorter duration also contributes to improvement in treatment adherence.
Directly Observed Treatment (DOT)
DOT is a method whereby a trained healthcare worker or another trained designated person (treatment supporter) watches a patient swallow each dose of anti-TB drugs and document it.
- DOT can reduce the development of drug resistance, treatment failure, or relapse after the end of treatment.
- Many patients who do not receive directly observed treatment stop taking drugs once they feel better.
- Hence, by providing DOT, the NTEP ensures that patients receive the right drugs, in the right doses, at the right intervals and for the right duration.
The modern treatment strategy is based on standardized short-course chemotherapy regimens largely administered on a domiciliary basis, utilising the DOTS strategy and proper case management to ensure completion of treatment and cure.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Treatment of Tuberculosis Disease, CDC, 2006.
- Guide on Tuberculosis Control for Primary Health Care Providers, WHO, 2015.
- Treatment of Tuberculosis: Guidelines for National Programmes, WHO, 2003.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of these treatment strategies are adopted by NTEP?
Domiciliary treatment
Use of short-course chemotherapy
Directly observed treatment
All of the above
4
Strategies utilized by NTEP in TB treatment are domiciliary, short-course chemotherapeutic short-course regimens that are directly observed.
Pharmacological Basis of treatment
ContentTuberculosis treatment and its different regimens have scientific backgrounds for their formulations. To understand this, we need to know about the mode of action of each anti-TB drug first.
Mode of Action of Anti-TB Drugs
Anti-TB drugs have the following three actions:
- Early bactericidal activity: Killing of actively growing bacilli (in the phase of rapid multiplication and uninhibited metabolic activity).
- Sterilizing activity of persisting bacilli, i.e., metabolically inhibited organisms in a quasi-dormant state.
- Ability to prevent the emergence of drug resistance.
The ranking of first-line drugs with respect to their type of activity is indicated in Table 1 below.
Table 1: Ranking of first-line anti-TB drugs used in the treatment of drug-sensitive TB, based on the mode of action and activity
First-line Drugs Early Bactericidal Sterilizing Prevention of emergence of drug resistance Isoniazid (H) ++++ ++ ++++ Rifampicin (R) +++ ++++ +++ Pyrazinamide (Z) ++ +++ + Ethambutol (E) + Nil ++ Thus, each drug has unique characteristics and drug combinations will make the regimen more effective.
Need for Long Duration of Treatment of TB
- Anti-TB drugs mostly kill actively multiplying tubercle bacilli.
- When bacilli have low metabolic activity, i.e., when bacterial growth has almost come to a standstill and the organisms are “dormant”, they are not killed by otherwise bactericidal drugs. Such organisms are referred to as persisters*.
- Though they may survive in the presence of drugs, behaving as if they were drug-resistant, they are in fact susceptible to the drugs.
- Thus, if for some reason these organisms regain their ability to multiply freely, they would be killed by the very drugs that had not harmed them before.
- When dormant bacilli again become metabolically active and start multiplying during effective chemotherapy, they are soon killed.
- Once chemotherapy has been completed, the revived bacilli may continue to multiply and thus cause relapse.
- This explains why conventional chemotherapy needs to be of long duration.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Tuberculosis Case-finding and Chemotherapy: Questions and Answers, K. Toman.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test What is the role of the intensive phase of anti-TB treatment? To reduce adverse drug reactions in patients To achieve rapid killing of actively multiplying bacillary population
To prevent the emergence of drug-resistance Options 2 and 3 4 The role of IP is to achieve rapid killing of actively multiplying bacillary population and eliminate naturally occurring drug-resistant mutants and prevent the further emergence of drug resistance. Yes Yes Which of the following drugs is bacteriostatic? Isoniazid Ethambutol Pyrazinamide Rifampicin 2 Ethambutol is an effective bacteriostatic drug, helpful in preventing the emergence of resistance to other companion drugs. Yes Yes Treatment Phases
ContentStandard TB Treatment is divided into two phases
- Intensive Phase(IP): In this phase,
- Kills most of the TB bacteria during the first 8 weeks of treatment, but some bacteria can survive longer
- Therefore, more drugs are administered to kill the bacteria and reduce the severity of disease.
- Treatment in this phase usually is of short duration(2 to 6 Months or more) in comparison to Continuation Phase(CP)
- Continuation Phase(CP): In this phase,
- All the remaining TB bacteria are in the dormant stage i.e., stage when growth and development of bacteria are temporarily stopped.
- Therefore, fewer but powerful antibiotics are administered to kill those bacteria.
- Treatment in this phase usually lasts longer than Intensive Phase(IP)(4 to 18 Months or more)
Kindly provide your valuable feedback on the page to the link provided HERE
- Intensive Phase(IP): In this phase,
Fixed Dose Combinations [FDC]s
ContentFixed-dose combinations (FDCs) are drug formulations where two or more drugs are combined physically into one formulation such as a tablet or pill.
This is more convenient to the patients taking medicines and it also simplifies the supply chain.

Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Advantages of FDCs
ContentFixed-Dose Combination(FDC) provides a simple approach to deliver the correct number of drugs at the right dosage as all the necessary drugs are combined in a single tablet. By altering the number of pills according to the patient’s body weight, complete treatment is delivered without the need for calculation of dose
Figure: Advantages of Fixed Dose Combination(FDC)
FDCs used in NTEP
ContentImage
TB Drug Regimen
ContentA regimen means a prescribed systematic form of treatment for a course of drug(s). For TB treatment, Multi drug combination of regimen is followed.
All TB drug regimens have an initial intensive phase(IP) followed by a continuation phase(CP).
Following are some of the main TB drug regimens used based on the drug resistance pattern detected for TB patients.
- First-Line Anti TB Drugs(Prescribed for Drug Sensitive TB DS-TB)
- Daily weight band wise FDC
- Second-Line Anti TB Drugs (Prescribed for Drug Resistance TB - DR-TB)
- H Mono Poly Regimen
- Shorter oral Bedaquiline containing MDR-TB regimen
- Longer oral Bedaquiline containing regimen
- Shorter injectable containing MDR-TB regimen
- First-Line Anti TB Drugs(Prescribed for Drug Sensitive TB DS-TB)
Follow-up of TB patient
ContentTo know the TB treatment response and to determine that if patient is cured, TB patients are clinically evaluated at the end of every four weeks of treatment, and they are also followed up by performing sputum test at end of each treatment phase (i.e. Intensive phase and Continuation phase)
TB patients during clinical evaluations are assessed to
- Identify possible adverse reactions to medications;
- Check for any comorbid conditions;
- Weight change;
- monitor adherence; and determine treatment efficacy by observing their symptoms
Although each patient responds to treatment at a different pace, all TB symptoms should gradually improve and eventually go away.
Patients whose symptoms do not improve during the first 2 months of treatment, or whose symptoms worsen after improving initially, should be re-evaluated for adherence issues and development of drug resistance.
Long Term Post-treatment follow up of TB patients
ContentAfter completion of TB treatment, all patients should be followed up at the end of
- 6 months,
- 12 months,
- 18 months &
- 24 months
TB patients at the follow up should be screened for any clinical symptoms and/or cough. If found positive on screening, then sputum microscopy and/or culture should be considered. This is important in detecting the recurrence of TB at the earliest.
After completion of TB treatment, if the patient has not developed any clinical symptoms and/or cough and also if the microscopy remains negative during their follow up, then the patient is considered as “Relapse Free Cure from TB.”
TB Treatment Outcome
ContentWhen a TB patient consumes all the doses under the prescribed regimen, then Treatment Outcome is declared for a Patient.
Treatment Outcome
Description
Cured
A TB patient who was microbiologically confirmed for TB at the beginning of treatment but who is smear or culture negative at the end of complete treatment
Treatment Complete
A TB patient who completed treatment without evidence of failure or clinical deterioration BUT with no record to show that the smear or culture results of biological specimen in the last month of treatment was negative, either because the test was not done or because the result is unavailable
Treatment Failure
A TB patient whose biological specimen is positive by smear or culture at the end of treatment
A case of paediatric TB who fails to have microbiological conversion to negative status or fails to respond clinically/or deteriorates after 4 weeks of compliant intensive phase shall be deemed to have failed response provided alternative diagnoses/reasons for non-response have been ruled out.
Loss to Follow up
A TB patient whose treatment was interrupted continuously for one month or more
Not Evaluated
A TB patient for whom no treatment outcome is assigned
Treatment Regimen Changed
A TB patient who is on first line regimen and has been diagnosed as having TB(DR-TB) and switched to DR-TB regimen prior to being declared as failed
Died
A patient who has died during anti-TB treatment(due to any reason)
Treatment success is considered when a TB patient either Cured or Treatment completed is accounted in treatment success
Adverse Drug Reactions
ContentAdverse Drug Reactions(ADR) are unwanted or harmful reactions experienced following the use of a drug or combination of drugs and are suspected to be related to a drug. Severity of adverse effects varies from tolerable and mild ADRs to serious and life threatening ADRs.
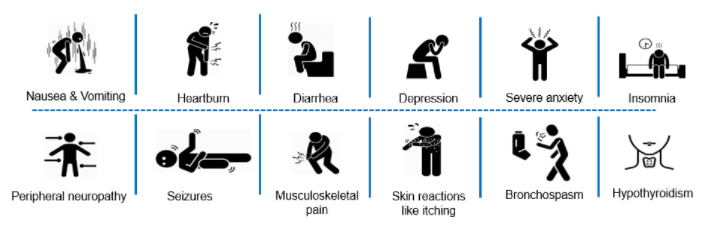
Figure: Various Adverse Drug Reactions
Common ADR Symptoms:
- Pain in upper abdominal area, with loss of appetite
- Nausea – Uneasy feeling with inclination to vomit, after having the drugs
- Gastritis – Burning sensation in lower chest region, bloating sensation, sourness in mouth
- Diarrhoea - Loose stool(2-3 in a day)
Types of ADR of TB Treatment
ContentAdverse Drug Reactions(ADR) are classified into serious and non-serious ADR depending upon the intensity of symptoms experienced by the patient. Below is the brief overview
Common ADRs
Non-serious ADR
Serious ADR
(Refer to the nearest health facility)
Nausea and Vomiting
Symptoms of dehydration like thirst, dizziness, tiredness, dry mouth and eyes
- Extreme vomiting,
- Signs and symptoms of severe dehydration
- Blood in vomit
- Electrolyte imbalance and
- Altered level of consciousness
Gastritis and Pain in abdomen
- Occasional Discomfort
- Sour taste in mouth with acid reflux
- Burning sensation in upper abdominal region
- Severe pain in abdomen
- Acidity, Burping, Flatulence, Vomiting
- Blood in vomit
- Electrolyte imbalance and
- Altered level of consciousness.
Diarrhoea
2-3 /3-10 loose liquid stools with signs and symptoms of dehydration.
- More than 10 watery stools
- Signs and symptoms of dehydration
- Blood in stool
- Fever
- Intense abdominal pain
- Electrolyte imbalance and
- Altered level of consciousness
Tingling, Burning, Numbness in hands and feet
- Mild numbness and weakness in hands and feet.
- Prickling, stabbing, burning or tingling along with gradual increase in severity of numbness and weakness.
- Signs and symptoms of moderate neuropathy
- Extreme sensitivity to touch,
- Lack of coordination and balance
- Muscle Weakness
- Poor control of bowel and bladder
Pain in Joints
- Pain on touching joints
- Pain on walking, swelling and redness
- Warmth in and around joints
- Stiffness and signs of increased tenderness
- Severe weakness and restricted joint movement
Skin rashes, itchiness, and allergic reactions
•Itching and skin rashes with tingling and burning sensations
- Itching with increased size and raised wheels
- Swelling of lips and tongue
- Severe allergic reactions /Serious disorder of the skin with painful rashes /Shredding of skin.
Management of Adverse Drug Reactions(ADRs) of TB Treatment
Content- Counsel and reassure the patient as the common occurring adverse effects usually resolve with time.
- Advise the patient to take all the drugs together.
- Advise patient to take light meal (biscuits, bread, rice etc.) before taking drugs.
- Inform patients that they may take drugs embedded in banana or at the bedtime to reduce their associated side effects.
- Encourage patients to keep themselves hydrated by increasing fluid intake.
- Provide ORS (Oral Rehydration Solution) to counter dehydration due to loose motion and vomiting.
Figure: Referral to PHI for ADR
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
TB Treatment Card
ContentThe Tuberculosis Treatment Card is a paper-based recording form that is kept in the institution treating the TB patient under the National TB Elimination Programme (NTEP). It is a pre-requisite documentation related to treatment services offered to TB patients under NTEP.
Uses of the TB Treatment Card
The TB treatment card is primarily used for:
- Documenting administered drugs with their dosages
- Documenting follow-up investigation results
- Monitoring adherence to treatment
- Recording adverse events
- Recording treatment outcomes
There are two pages in the TB treatment card and details in each page is delineated in the table below.
Table: Parts of the Treatment Card; Source: NTEP Training Module 2 for Programme Managers & Medical Officers, p. 105
PAGE
DETAILS CONTAINED IN PAGE
The First Page
Patient details such as name, age, sex and address of the patient
Type of disease History of anti-TB treatment Regimen prescribed and duration of treatment Results of investigation before and during treatment Comorbidity-related information Contact tracing and chemoprophylaxis details Social habits such as tobacco and alcohol use The Back Page
Details of intensive and continuation phases of treatment including drug details and adherence monitoring
Retrieval actions for missing doses Adverse events Post treatment follow-up, nutritional support details and remarks Treatment outcome Important Points to Note
- The TB treatment card is filled at the Peripheral Health Institution (PHI) when a patient is initiated on treatment.
- The original TB treatment card is kept at the PHI and updated fortnightly.
- A duplicate treatment card is to be given to the treatment supporter for documentation of daily events.
- The treatment supporter should be trained on how to record the treatment card.
- Details on the patient’s HIV status are not included in the treatment supporter’s copy to maintain confidentiality.
The figure below shows the 1st page of the TB treatment card. Click here to access the full form in the NTEP Training Modules 1-4 for Programme Managers & Medical Officers, p. 223.
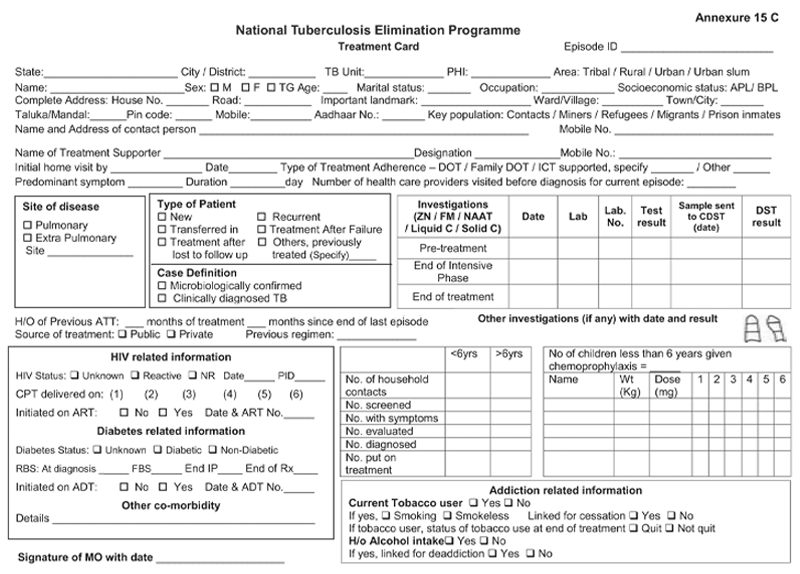
Figure: First Page of the TB Treatment Card; Source: NTEP Training Modules 1-4 for Programme Managers & Medical Officers, p. 223
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
NTEP TB ID Card
ContentIn the National TB Elimination Programme (NTEP), the ‘NTEP TB identity card’ is provided for their identification and record of clinical follow-ups.
The identity card is completed for each patient who has a Tuberculosis (TB) Treatment Card, and it is kept with the patient. Information from the TB Treatment Card is used to complete the identity card.
There are 3 parts in the NTEP TB identity card and details in each part is delineated in Table 1.
Table 1: Parts of the NTEP TB identity card; Source: NTEP Training Module 2 for Programme Managers & Medical Officers, p. 105
PART
DETAILS CONTAINED IN THE SECTION
The First and Second Part
Patient information
Name and address of the TB unit/ district
Treatment details of the patient including:
- Disease classification
- Type of patient
- Treatment provider
- Case definition
- Weight bands
- Dosage
- Sputum results
- Culture results
- Results of follow-up smear examinations
- Results of follow-up cultures
- Information on the date of treatment initiation
- Treatment outcome
The Back Part
Appointment dates for visits to NTEP facilities
Contact details of NTEP staff in case of side events/queries
The information contained in this card will help to continue treatment in case the patient is transferred or admitted to any other health facility any time during the treatment period. The TB identity card is shown in Figure 1.
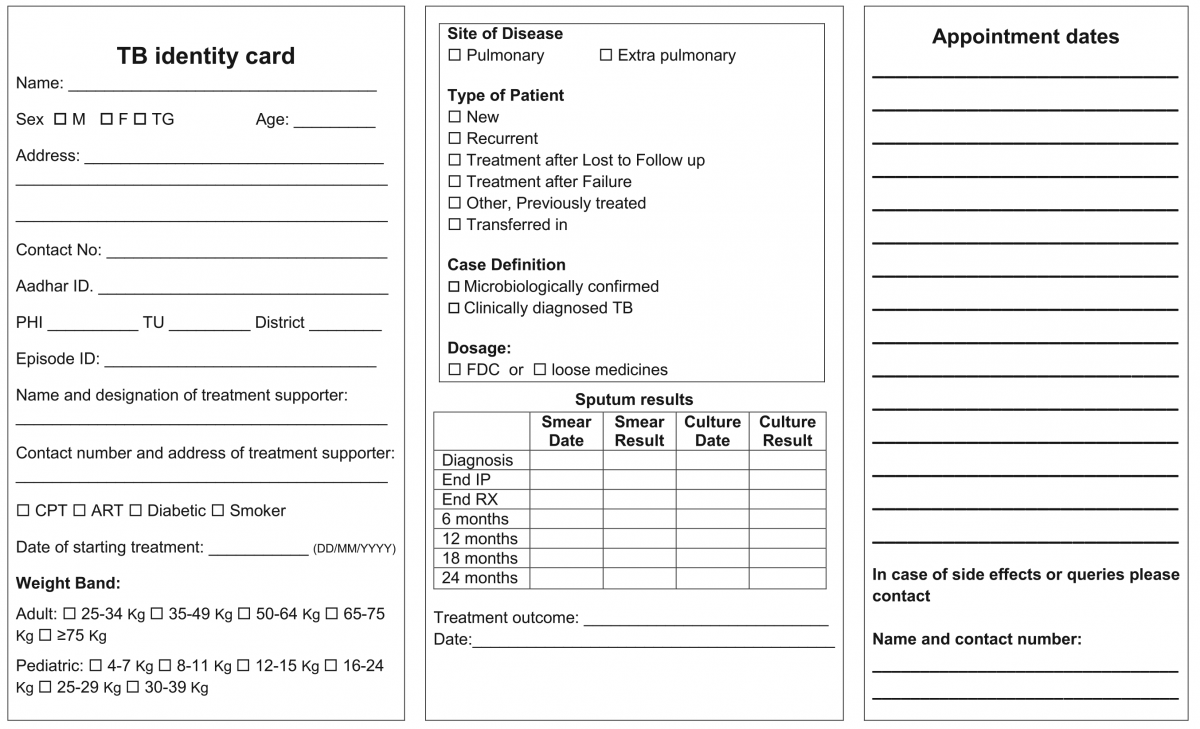
Figure 1: NTEP TB Identity Card; Source: NTEP Training Modules 1-4 for Programme Managers & Medical Officers, 2020

Figure 2: Sample of a patient’s TB identity card


Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Transfer of TB Patient
ContentTB patients may not stay in one place throughout the treatment duration. When they move from one place to other, there should be a mechanism to hand over the responsibility of continuing the patient's treatment in a facility near the new place of the patient. This is the concept of patient transfer and can be easily managed in Nikshay portal.
- The transfer module in Nikshay enables transfer requests of patients between Health Facilities (HFs) across the country.
- Provision of shifting of patient from one HF to another is possible if the patient changes his/her residence for the purpose of treatment.
- The requests are of two types: “Transfer In” and “Transfer Out”.
- All transfer requests needs to be accepted by the “District/ TB Unit (TU)/ Peripheral Health Institute (PHI)” where the transfer request is made in order for it to take effect.
- Transfer requests can be made to even the District/ TU level. However, it can be completed only once the “Transferred to PHI” has been assigned.

Figure: Transfer Management in Nikshay; Source: Nikshay Zendesk, Nikshay Knowledge Base, Advanced Transfer in Web.
Steps in Transfer of TB Patient
1. In Nikshay, the referring HF updates details from the current HF of patient to the HF where patient is being transferred.
2. The receiving HF gets the intimation about the transfer.
The patient transfer module also provides the provision to pull the patient belonging to another HF to the recipient HF. The accountability of the transferred patients is now with the receiving HF and the treatment initiating facility.
A separate transfer register is also available to get details about various transfers from and to a given district, which can be downloaded from Nikshay reports.
Resources
- Nikshay Zendesk, Nikshay Knowledge Base, Advanced Transfer in Web.
- Guidelines for PMDT in India, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Transfer requests include "Transfer In" and "Transfer Out".
True
False
1
Transfer requests include "Transfer In" and "Transfer Out".
Yes
Yes
Management of EPTB
ContentThe management principles of Extrapulmonary Tuberculosis (EPTB) are shown in the figure below.

Figure: Ten principles about what every EPTB patient in India needs as a basic standard of care
Abbr: CBNAAT:Cartridge-based Nucleic Acid AMplification Test; PTB: Pulmonary TB; NTEP: National TB Elimination Programme
Diagnosis of EP-TB
- All efforts need to be made to get a microbiological confirmation whenever a sample is available.
- Clinical diagnosis can be made by treating physician based on the clinical features, lab investigations, imaging studies and by ruling out other causes
Treatment Regimen and Duration for EPTB
The treatment regimen and schedule for EPTB cases will remain the same as for pulmonary TB (2HRZE/ 4HRE). However, the duration of the continuation phase in EPTB may be extended in special situations such as TB Meningitis, bone and spine TB etc.
Role of Surgery in EPTB Cases
- Surgery is sometimes required for the diagnosis of EPTB. It is reserved for management of late complications of the disease.
Monitoring Treatment Response
- Response to treatment in EPTB may be best assessed clinically. Clinical follow-up is the most important criterion for the follow-up of EPTB patients. The clinician can assess the patient’s condition by checking weight gain and a decrease/ increase in presenting clinical symptoms.
- Investigations such as Acid-fast Bacilli (AFB) microscopy, chest X-ray, liver function tests, serum creatinine, and USG-abdomen can be used to monitor the treatment status.
The treatment support and other monitoring activities remain the same as for pulmonary TB.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Index TB Guidelines on Extra-pulmonary Tuberculosis for India, Central TB Division, 2016.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What is the standard treatment duration for most EPTB cases?
2 weeks
1 month
6 months
3 years
3
The treatment regimen and schedule for EPTB cases will remain the same as for pulmonary TB (2HRZE/ 4HRE).
Yes Yes In which cases can the treatment duration exceed 6 months in EPTB?
TB meningitis
TB of the bone and joint
Depending on the clinician’s decision
All of the above
4
EPTB treatment duration can be extended beyond 6 months in TB meningitis, TB of bone and joint (including TB otitis media), and if recommended by the clinician.
Yes
Yes
Management of Patients with Treatment Interruptions
ContentTreatment interruption is defined as a patient-initiated episode in which the patient discontinues TB treatment. All efforts must be made to ensure that TB patients do not interrupt treatment or are not lost to follow-up. Action should be taken to promptly retrieve patients who fail to come for their daily dose by the treatment supporter
The management of treatment interruptions is made based on the following criteria:
i. Type of case: Whether new, relapse or failure
ii. Duration of treatment taken: Less than one month/ more than one month. This helps in assessing the risk of the presence of drug resistance.
iii. Duration of Interruption: Less than one month/ more than a month.
If treatment interruption is more than one month, the outcome is declared as ‘lost to follow up’.
If a patient returns to the health facility after interrupting treatment for more than one month, the patient sample needs to be subjected to Drug Susceptibility Testing (DST) to determine resistance/ sensitivity status to anti-TB drugs.
In case the interruption is for less than one month, the same treatment regimen is completed to complete all doses.
Modes of Retrieval
TB treatment is supervised by a trained treatment supporter (a health worker, family member or community volunteer). The residential address is verified for all TB patients by home visits. However, in case of treatment interruption, patient retrieval action is required.
Retrieval can be done by the following modes:
1. Retrieval of patients interrupting treatment within 24 hours of discontinuation is done by the Treatment Supporter (TS) or Accredited Social Health Activist (ASHA)/ Auxilliary Nurse Midwife (ANM)/ Multipurpose Worker (MPW). The reason for interruptions should be reviewed carefully and efforts made to counsel and bring the patient back for treatment.
2. If the TS is not successful in retrieving such patients, it should be reported to the next higher level of supervisors, like Senior Treatment Supervisor (STS), and they should take all efforts to counsel and retrieve the patient.
3. If the patient interrupts treatment on more than one occasion, the Medical Officer of the Peripheral Health Institute (MO-PHI) should visit the patient’s home. The MO-PHI should give intensive counselling to the patient and may provide additional support to continue the treatment without interruption.
4. Innovative use of information and communication technologies for treatment adherence monitoring through 99 DOTS, Medication Event Reminder Monitor (MERM), etc. are also beneficial in finding missed doses and initiating retrieval action by the health staff.
Resources
1. Training Modules (1-4) for Programme Managers and Medical Officers.
2. Guidelines for PMDT in India, 2021.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test If treatment interruption is more than one month, the outcome is declared as ‘lost to follow-up'. True False 1 If treatment interruption is more than one month, the outcome is declared as ‘lost to follow-up'. Yes Yes Prevention of Drug Resistance
ContentThere are five principal ways to prevent Drug-resistant Tuberculosis (DR-TB), as given in the figure below.
Image
Figure: Five Principal Ways to Prevent DR-TB; Source: Guideline for PMDT in India, 2021.
- Drug resistance cannot be prevented by mere diagnosis and treatment of DR-TB.
- Basic TB diagnostic and treatment services should receive priority for the prevention of drug resistance.
- Systems for early detection and treatment of DR-TB should be integrated into the existing TB services and the general health system.
- Healthcare facilities and congregate settings should be provided with proper infection control measures.
- Transmission should be prevented by addressing non-specific determinants like access to care, comorbidities and awareness.
Resources
- Guidelines for PMDT in India, 2021.
- Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-resistant Tuberculosis.
Kindly provide your valuable feedback on the page to the link provided HERE
Treatment Regimen for Non-Mycobacterium Tuberculosis [NTM]
ContentThe suggested treatment regimen covering maximum non-Mycobacterium Tuberculosis (NTM) mainly Mycobacterium Avium Complex (MAC) is as follows:
- Rifampicin (R) 450-600 mg OD
- Ethambutol (E) 800-1200 mg OD
- Clarithromycin (Clr) 1 gm OD (split into two doses)
- Add injection Amikacin (Am) 750 mg – 1 gm thrice weekly for the first 2-3 months
Intensive Phase (IP) is for 3 months and can be extended to a maximum of 6 months with all four drugs.
Continuation Phase (CP) of treatment will be with the same drugs except for injectable. This should be continued for 12 months after sputum culture conversion. Drugs will be given as per the standard weight bands.
If the patient does not culture convert by end of 3 months, then species identification and Drug Susceptibility Testing (DST) are required for further management.
Management of complicated/ invasive TB disease:
- Recommended initial regimen for most patients with nodular/ bronchiectatic MAC lung disease:
- Thrice-weekly regimen including Clarithromycin 1000 mg or Azithromycin 500 mg, Ethambutol 25 mg/kg, and Rifampicin 600 mg administered three times per week.
- Recommended initial regimen for fibro-cavitary or severe nodular/ bronchiectatic MAC lung disease:
- Clarithromycin 500-1000 mg/day or Azithromycin 250 mg/day, Ethambutol 15 mg/kg/day, and Rifampicin 10 mg/kg/day (maximum, 600 mg).
Points to Note
- Intermittent drug therapy is not recommended for patients who have a cavitary disease, patients who have been previously treated, or patients who have moderate or severe disease.
- The primary microbiologic goal of therapy is 12 months of negative sputum cultures while on therapy; therefore, sputum must be collected from patients for Acid-fast Bacilli (AFB) examination throughout treatment on monthly basis in IP and quarterly basis in CP after culture conversion is achieved.
- Given these complexities, the treatment of NTM will be the prerogative of the Nodal Drug-resistant TB Centres (NDR-TBCs).
Resources
- Training Modules (1-4) for Programme Managers & Medical Officers (NTEP), 2020.
- British Thoracic Society Guidelines for the Management of Nontuberculous Mycobacterial Pulmonary Disease, 2017.
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
Kindly provide your valuable feedback on the page to the link provided HERE
-
Ph-Ch7: DS-TB Treatment and care
FullscreenCategorization of DSTB Treatment Regimen
ContentDaily Regimen is prescribed for Drug Sensitive TB patients (DSTB), where the patient needs to consume the FDC formulation daily.
Daily Regimen comprises the first line Anti TB drugs based on
- Age: Adult/ Pediatric
- Weight of the patient: Weight Bands
Age: Based on age, patients are categorized into
- Adults: The patient's age should be greater than 19 years
- Paediatrics: Patient's age up to 19 years and weight less than 39 Kgs
Weight Bands:
- Treatment dosages are based on TB patients’ weight.
- A weight band category is defined for Adults and Pediatric patients separately, and FDC are issued based on that weight category.
Treatment Regimen for DSTB – Adult
ContentIntensive Phase(IP): Consists of eight weeks (56 doses) of HRZE in daily dosages as per weight of patient.
Continuation Phase(CP): Consists of 16 weeks (112 doses) of HRE in daily dosages as per weight of patient.
For adults, there are five weight bands, as shown in the table below. The table also indicates the number of FDC tablets that have to be consumed in each weight band
Weight band category
Intensive phase(IP)
(HRZE - 75/150/400/275)
Continuation phase(CP)
(HRE - 75/150/275)
25–34 kgs
2
2
35–49 kgs
3
3
50–64 kgs
4
4
65–75 kgs
5
5
>=75 kgs
6
6
Regular monthly follow up of the patient needs to be done and if patient loses or gains approx. 5 kg weight and if weight band changes during the treatment, then the dose of the patient needs to be recalculated.
Treatment Regimen for DSTB - Pediatrics
ContentIntensive Phase (IP)
Consists of eight weeks (56 doses) of HRZ in daily dosages as per weight of patient.
Ethambutol (E) is given separately for children to monitor ophthalmic side effects.
Continuous Phase (CP)
Consists of 16 weeks (112 doses) of HRE in daily dosages as per the weight of the patient.
In Pediatric, there are six weight bands’s as shown in the table below. The table also indicates the number of FDC tablets that has to be consumed in each weight band
Weight Band category
Fixed-Dose Combinations (FDCs)
Intensive phase (IP)
(HRZE - 75/150/400/275)
Continuation phase (CP)
(HRE - 75/150/275)
4-7 kgs
1 1 8-11 kgs
2 2 12-15 kgs
3 3 16-24 Kgs
4 4 25-29 Kgs
3 + 1A 3 + 1A 30-39 Kgs
2 + 2A 2 + 2A Regular monthly follow-up of the paediatric patient needs to be done and if the patient weight crosses the range of the weight band during the treatment, then the weight band of the patient should be changed immediately.
Children above 39 kg shall usually be adolescents, the drug dosage requirement for them would be similar to adults
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
DS-TB Treatment – Patient Flow
ContentCommunity Health Volunteers(CHVs) have to refer the presumptive cases identified based on the r symptom screening to the nearest NTEP health facility for further investigation. Once Diagnosed with TB, the TB patients are initiated on the first-line TB treatment. Patients are also offered NAAT within a maximum of 15 days to rule out any drug resistance. If no drug resistance is detected, then the patient continues on the first-line TB treatment. TB patients are then clinically evaluated every month to check the progress of TB treatment.
The treatment duration of TB is divided into two phases - The Intensive Phase(IP) and the Continuation Phase(CP). Post-treatment completion, patients are then evaluated at intervals of 6,12,18 and 24 Months to ensure a relapse-free TB cure for the patient.
Figure: DSTB Treatment Flow
Adverse Drug Reactions(ADRs) to First Line Treatment
ContentSymptoms
Drug Responsible
Action to be taken by Community Health Volunteers
Gastrointestinal Symptoms
Any Oral Medications
-
Reassure patient.
-
Give TB Drugs with less water at a longer interval.
-
If symptom persists, refer to the nearest health facility
Itching/Rashes
Isoniazid
-
Reassure patient.
-
In case of severe itching, refer the patient to the nearest health facility
Tingling/ burning/ numbness in the hands & feet
Isoniazid
-
Refer the patient to the nearest health facility
Joint Pains
Pyrazinamide
-
Reassure patient.
-
Increase intake of liquids.
-
If severe, refer the patient to the nearest health facility
Impaired Vision
Ethambutol
-
Refer the patient to the nearest health facility
Ringing in the ears, Loss of hearing, Dizziness and loss of balance
Isoniazid, Rifampicin or Pyrazinamide
-
Refer the patient to the nearest health facility
Hepatitis: Anorexia/ nausea/ vomiting/ jaundice
Isoniazid, Ethambutol, Rifampicin or Pyrazinamide
-
If patient detected with signs of jaundice, refer the patient to the nearest health facility
-
-
PHI Pharmacist : DR-TB TREATMENT AND CARE
FullscreenDrug-Resistant Tuberculosis(DR-TB)
ContentWhat is Drug-Resistant Tuberculosis?
-
Drug-Resistant TB occurs when bacteria become resistant to the drugs used to treat TB. This means that the drug can no longer kill the TB bacteria.
-
Multidrug-resistant TB (MDR TB) is a type of DR-TB where TB bacteria is resistant to both Isoniazid and Rifampicin, the two most potent anti-TB drugs.
Figure: High Risk for Drug-Resistant Tuberculosis (DRTB)
Resources:
-
Goals of DR-TB Treatment
ContentGoals of Drug-resistant Tuberculosis (DR-TB) treatment under the National Tuberculosis Elimination Program (NTEP) are as follows:
Image

Figure: Goals of DR-TB Treatment; Source: Guidelines for PMDT in India, March 2021, p41.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- Technical and Operational Guidelines for TB in India, 2016.
Kindly provide your valuable feedback on the page to the link provided HERE
Screening for DR-TB
ContentAll patients diagnosed with TB should have universal access to rapid DST for at least Rifampicin and further DST for at least Fluoroquinolones among all TB patients with rifampicin resistance, i.e. UDST.
UDST tests are offered preferably before treatment initiation to a maximum within 15 days from diagnosis. Based on the UDST test result, if Rifampicin resistance is detected, the patient is shifted to DR-TB Treatment Regimen. If Rifampicin resistance is not detected, then first-line anti TB treatment is continued, and the patient is screened further on their follow-ups. If tested positive in sputum examination during any patient follow up, then sputum is sent for further drug resistance testing, and the patient is referred to PHI for follow-up.
Figure: Screening of patient for initiating DRTB Treatment from DSTB Treatment
Types of Drug Resistance Tuberculosis -DRTB
ContentResistant Sensitive
Unknown / Sensitive Types of Drug Resistance TB (DR TB) Resistance to Isoniazid (H) Resistance to Rifampicin (R) Resistance to Fluroquinolone (FQ)
- Ofloxacin,
- Levofloxacin,
- Moxifloxacin
Resistance to Group A Drugs
- Bedaquiline or
- Linezolid
H Mono / Poly Drug Resistance
- Resistant to Isoniazid (H)
- Sensitive to Rifampicin (R)
- Unknown / Sensitive to Fluoroquinolone (FQ) or Group A Drugs - Bedaquiline or Linezolid
Rifampicin Resistance (RR)
- Resistant to Rifampicin (R)
- Unknown / Sensitive to other drugs
Multi Drug Resistance TB (MDR TB)
- Resistant to Isoniazid (H) and Rifampicin (R)
- Unknown / Sensitive to Fluoroquinolone (FQ) or Group A Drugs - Bedaquiline or Linezolid
Pre-Extensive Drug Resistance (Pre -XDR)
-
Resistant to Isoniazid (H), Rifampicin (R) and any Fluroquinolone (FQ)
- Sensitive/ Unknown to Group A Drugs - Bedaquiline or Linezolid
Extensive Drug Resistance (XDR)
- Resistant to Isoniazid (H) , Rifampicin (R) and any Fluoroquinolone (FQ) and at least one additional Group A Drugs - (presently to either Bedaquiline or linezolid [or both])
Resources:
DR-TB Treatment Regimens
ContentDepending upon type of drug resistance, there are four broad DRTB Treatment regimen.
- H Mono/Poly Treatment Regimen(6-9 months)
- Shorter oral Bedaquiline containing MDR/RR-TB regimen(9-11 months)
- Shorter injectable containing regimen(9-11 months)
- Longer oral M/XDR-TB regimen(18-20 months)
Drugs administered for DRTB Regimen:
- Drugs are decided based on the drug resistance detected for a patient and will be informed by the medical officer.
- Injections might also be administered to the admitted patient.
- H Mono/Poly Regimen can be initiated at any health facility, while the other two regimen need to be initiated at N/DDR-TB Centre
Figure: Patient wise boxes(PWB) for DRTB Treatment
Pre-treatment Evaluation [PTE] of DR-TB Patients
ContentPTE Objective
Drugs used for the treatment of drug-resistant TB have significant adverse effects. Hence, there is a need for PTE to rule out any underlying condition at the baseline, like co-morbid conditions, radiological abnormalities, Electrocardiogram (ECG) changes, or biochemical derangements.
PTE is essential to identify:
- The patient's eligibility for initiation of a particular regimen
- Patients who require special attention during treatment
- Regimen modifications from the beginning of treatment
Table: Pre-treatment (PTE) for MDR/RR-TB patients Clinical Evaluation Lab based evaluation History and Physical Examination Random blood sugar (RBS) Height HIV testing following counselling Weight Complete blood count (Hb, TLC, DLC, platelet count) Psychiatric evaluation if required Liver function tests (including serum proteins) TSH levels Urine examination – routine and microscopic Serum electrolytes (Na, K, Mg, Ca) Urine pregnancy test (in women of reproductive age group) Chest X-ray ECG Important Points
- In the majority of Multidrug-resistant (MDR)/ Rifampicin-resistant Tuberculosis (RR-TB) patients, PTE can be done on an outpatient basis.
- The District TB Officer (DTO) and Medical Officer of the TB Unit (MO-TU) can arrange for PTE at the Nodal and District DR-TB Centre (N/DDR-TBC) or at the sub-district level health facility, wherever feasible.
- No additional investigations are required for H Mono/ Poly DR-TB patients unless clinically indicated.
- The PTE carried out at the time of treatment initiation can be considered valid for 1 month from the date of the test result and the patient can be re-initiated on a subsequent regimen considering the previously conducted PTEs.
- Active Drug Safety Management and Monitoring (aDSM) treatment initiation forms are required to be completed for all DR-TB patients at the time of initiation of each new episode of treatment.
- PTE should include a thorough clinical evaluation by a physician and expert consultation as per the need.
- Laboratory-based tests should be performed based on the drugs used in the treatment regimen.
- Pre-treatment evaluation should be made available free of charge to the patient.
Resources
Second Line anti TB drugs
ContentThe anti-TB drugs recommended for treatment of Multi- and Extensively Drug-resistant (M/XDR) TB patients are grouped into three groups – A, B and C (Figure below).
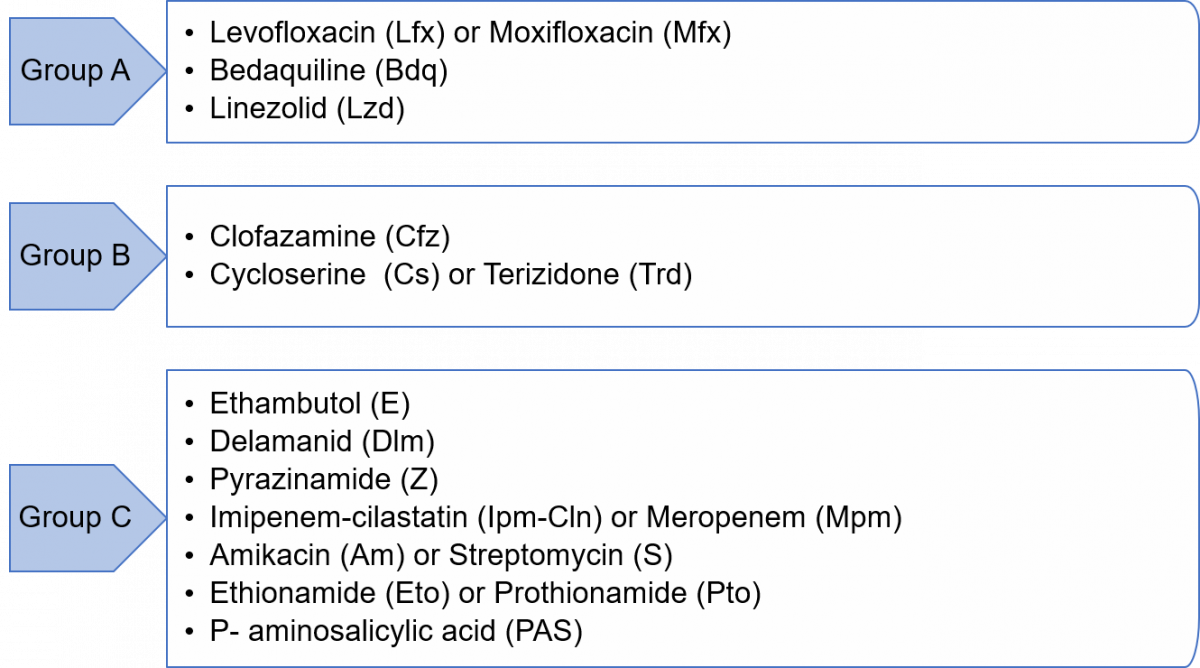
Figure: Groups A, B and C of Anti-TB Drugs used in Treatment of M/XDR-TB Patients
Grouping of drugs is done based on their efficacy, experience of use and drug class. This grouping is intended to guide the design of individualized, longer M/XDR-TB regimens (the composition of the recommended shorter MDR/RR-TB regimen is largely standardized).
Resources
- Guidelines for Programmatic Management of Tuberculosis in India, 2021.
- WHO Consolidated Guidelines on Tuberculosis, Module 4 - Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Newer Anti-TB Drugs
Content
Figure: Sirturo 100 mg Bedaquiline Tablets
- Newer anti-TB drugs are needed to improve the treatment outcomes of DR-TB, shorten the duration of treatment, address the problem of drug resistance, and have less toxic drugs.
- Five decades after the discovery of Rifampicin, two newer drugs with anti-TB effects were approved for the treatment of multidrug-resistant tuberculosis (MDR-TB) by the Central Drugs Standard Control Organization (CDSCO). These are:
- Bedaquiline (Bdq)
- Delamanid (Dlm)
- In July 2020, the Drug Controller General of India (DCGI) also approved a third newer drug - Pretomanid (Pa) to use under the Conditional Access Programme (CAP) under the National Tuberculosis Elimination Program (NTEP).
Resources
- The Use of Bedaquiline in the Treatment of Multidrug-resistant Tuberculosis, Interim Policy Guidance, WHO, 2013.
- The Use of Delamanid in the Treatment of Multidrug-resistant Tuberculosis in Children and Adolescents, Interim Policy Guidance, WHO, 2016.
- WHO Consolidated Guidelines on Tuberculosis, Module 4: Treatment- Drug-resistant TB Treatment.
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
Kindly provide your valuable feedback on the page to the link provided HERE
Weight Band-wise Dosages of DR-TB Drugs for Adults
ContentThe dosage for Drug-resistant TB (DR-TB) drugs used in the regimen by weight bands for adults are enumerated in the table below.
Table: Weight Band-wise Drug Dosage of DR-TB Drugs for Adults; Source: Guidelines for PMDT, India 2021, pp.51,64. SR NO
DRUGS 16-29 KG 30-45 KG 46-70 KG >70 KG 1 Levofloxacin (Lfx) 250 mg 750 mg 1000 mg 1000 mg 2 Moxifloxacin (Mfx) 200 mg 400 mg 400 mg 400 mg 3 High dose Mfx (Mfxh) 400 mg 600 mg 600 mg 600 mg 4 Bedaquiline (Bdq) Week 0–2: Bdq 400 mg daily
Week 3–24: Bdq 200 mg 3 times per week
5 Clofazimine (Cfz) 50 mg 100 mg 100 mg 200 mg 6 Cycloserine (Cs)3 250 mg 500 mg 750 mg 1000 mg 7 Linezolid (Lzd) 300 mg 600 mg 600 mg 600 mg 8 Delamanid (Dlm) 50 mg twice daily (100 mg) for 24 weeks in 6-11 years of age
100 mg twice daily (200 mg) for 24 weeks for ≥12 years of age
9 Amikacin (Am)1 500 m 750 mg 750 mg 1000 mg 10 Pyrazinamide (Z) 750 mg 1250 mg 1750 mg 2000 mg 11 Ethionamide (Eto)3 375 mg 500 mg 750 mg 1000 mg 12 Na - PAS (60% weight/ vol)2,3 10 gm 14 gm 16 gm 22 gm 13 Ethambutol (E) 400 mg 800 mg 1200 mg 1600 mg 14 Imipenem - Cilastatin (Imp-Cln)3 2 vials (1 g + 1 g) bd (to be used with Clavulanic acid) 15 Meropenems (Mpm)3 1000 mg three times daily (alternative dosing is 2000 mg twice daily 16 Amoxicillin-Clavulanate (Amx-Clv) (to be given with Carbapenems only) 875/125 mg bd 875/125 mg bd 875/125 mg bd 875/125 mg bd 17 High-dose H (Hh) 300 mg 600 mg 900 mg 900 mg 18 Rifampicin (R) 300 mg 450 mg 600 mg 750 mg 19 Pyridoxine (Pdx) 50 mg 100 mg 100 mg 100 mg 1For adults more than 60 yrs of age, dose of Second Line Injectable (SLI) should be reduced to 10 mg/kg (max up to 750 mg)
2In patients on Para-aminosalicylic Acid (PAS) with 80% weight/volume the dose will be changed to 7.5 gm (16-29 kg); 10 gm (30- 45 kg); 12 gm (46-70 kg) and 16 gm (>70 kg)
3Drugs can be given in divided doses in a day in the event of intolerance
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-resistant Tuberculosis, 2014.
Kindly provide your valuable feedback on the page to the link provided HERE
Treatment of DR-TB in Children
ContentThe principles of designing Drug-resistant TB (DR-TB) treatment regimens (Shorter or longer oral Multi (M)/ Extensively Drug-resistant TB (XDR-TB), and H mono/ poly DR-TB regimens in children are similar to adults:
- Children, aged 5 years to less than 18 years of age and weighing at least 15 kg, are eligible for both longer oral and shorter oral Bedaquiline-containing Multidrug-resistant (MDR)/ Rifampicin-resistant TB (RR-TB) regimens.
- Management of H mono/ poly DR-TB in children will be the same as in adults and child-friendly formulations can be used.
- The drug doses should be used as per paediatric weight bands.
- Bedaquiline (Bdq) tablets suspended in water have been shown to have the same bioavailability as tablets swallowed whole and therefore, should be used to treat DR-TB in children until a child-friendly formulation becomes available.
- Delamanid (Dlm) is already approved for treating M/XDR-TB under the National TB Elimination Programme (NTEP) for children from 6 years onwards.
- As in adults, the extension of Bdq beyond 6 months and concomitant use of Bdq and Dlm in special situations will apply to children as well.
- Treatment can be directly extended to 9 months in certain conditions like extensive disease, extrapulmonary TB, uncontrolled comorbidity, smear-positive cases at the end of the 4th month and when the regimen is modified.
- Shortening the total treatment duration to less than 18 months may be considered in children without the extensive disease.
- For children under 5 years of age, where neither Bdq nor Dlm is approved yet, the longer oral M/XDR-TB regimen should be suitably modified as per the replacement drug. A suitable regimen can be designed considering child-friendly formulations where Bdq can be replaced with Amikacin (Am), Pyrazinamide (Z) or Ethionamide (Eto) in the initial phase.
- Children below 5 years are not excluded from short-course regimens, instead receive short course injectables till further evidence on the use of Bdq is available.
- The use of injectable agents in children should be exceptional and limited to salvage treatment and be monitored for early detection of ototoxicity.
- Meropenem is the preferred drug over imipenem in TB meningitis considering the risk of seizures in children due to Imipenem.
Additional Information
- Achieving an appropriate dose in children aged 3-5 years will be easier when the special formulation dispersible 25 mg tablet used in trials in these age groups becomes available.
- The recent data review for the World Health Organization (WHO) guidelines suggested that there are no additional safety concerns for concurrent use of Dlm with Bdq.
- For treatment and management of adverse drug reactions in children, there should be provision for treatment in consultation with a specialist.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- Consolidated Guidelines on Tuberculosis: Module 4 - Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Adverse Drug Reactions(ADRs) to Second Line Treatment
ContentCommon Adverse events to second line treatment are as below
Figure: Adverse Drug Reaction to Second line drugs
Adverse events should be identified, monitored and be referred to
- Nearest treating doctor for minor symptoms or
- District DR-TB Centres for major symptoms
If required, hospitalization can be done at the District DR-TB Centers where inpatient facility is available or referred to a Nodal DRTB Centre for admission
Reporting of Adverse Events and Serious Adverse Events
ContentAll serious and non-serious adverse events which are possibly, probably or very likely related to any anti-TB drug need to be reported by the physician to the National TB Elimination Programme (NTEP).Serious Adverse Events (SAE) needs to be reported to the nearest ADR monitoring centre (AMC) and Central TB Division (CTD) within 24 hours. Any death of a patient occurring during treatment, regardless of causality, must be reported as an SAE.
aDSM-treatment review form to be filled whenever the DR-TB patient develops any SAE
- The primary responsibility of filling up the aDSM forms will be with the nodal officer of the DR-TB centre with the help of a senior medical officer (SMO) or medical officer (MO) designated.
- It is essential that Nikshay data entry are being done on regular basis by statistical assistant at the NDR-TBC and senior DR-TB TB-HIV supervisor at the DDR-TBC centre.
- Forms should be maintained in hard copies until the ADR module is active in Nikshay.
Once relevant forms of aDSM are filled in Nikshay, information is directly communicated to the pharmaco-vigilance programme of India (PvPI) through the Vigiflow=connecting bridge for signal generation.
Resources
-
Ph-Ch9: Shorter Oral Bedaquiline-containing MDR/RR-TB Regimen
FullscreenShorter oral Bedaquiline-containing MDR/RR-TB regimen
ContentBased on the World Health Organization (WHO) treatment guidelines, 2020 recommendations, the National TB Elimination Programme (NTEP) have decided to transition from the current shorter injectable-containing Multi-drug Resistant (MDR)/ Rifampicin-resistant TB (RR-TB) regimen to the shorter oral bedaquiline-containing MDR/RR-TB regimen in the year 2021.
Salient Features of the Shorter Oral Bedaquiline-containing MDR/RR-TB Regimen
- This regimen will be used in patients >5 years of age weighing 15 kg or more.
- The regimen will be expanded in a phased manner starting with selected states to gain programmatic experience to guide future expansion within 2021.
- The regimen consists of an initial phase of 4 months that may be extended up to 6 months and a continuation phase of 5 months, giving a total duration of 9-11 months. Bdq is used for a duration of 6 months.
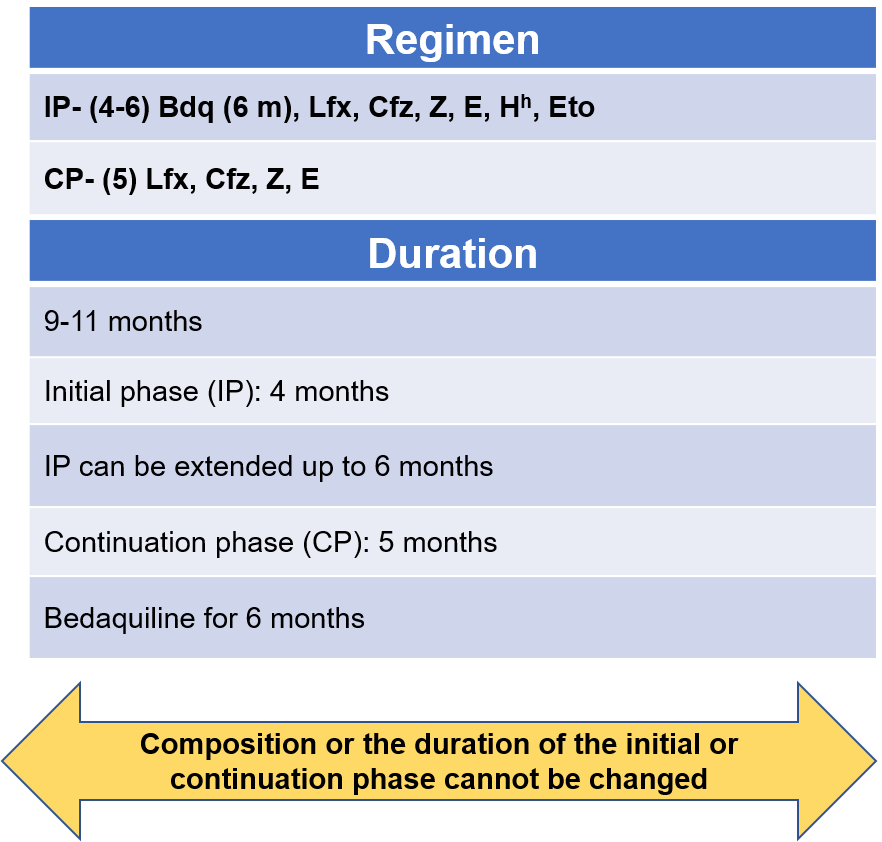
Figure 1: Regimen and duration of shorter oral Bdq-containing MDR/RR-TB regimen
Abbr: Bdq - Bedaquiline, Lfx- Levofloxacin, Cfz- Clofazamine, Z- Pyrazinamide, E- Ethambutol, Hh- High-dose Isoniazid, Eto- Ethionamide
Points to Note
- From the start to the end of 4 months these drugs are used: Bedaquiline, Levofloxacine, Clofazamine, Pyrazinamide, Ethambutol, high-dose Isoniazid, Ethionamide
- From the start of 5 months to the end of 6 months (If IP not extended): Bdq, Lfx, Cfz, Z, E
- From the start of 7 months to the end of 9 months: Lfx, Cfz, Z, E
If the IP is extended up to 6 months, then all 3 drugs Bdq, Hh and Eto are stopped together
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- WHO Consolidated Guidelines on Tuberculosis, Module 4 - Treatment: Drug Resistant TB Treatment.
Kindly provide your valuable feedback on the page to the link provided HERE
Shorter Oral Bedaquiline-containing MDR/RR-TB Regimen: Treatment Extension
ContentThe total duration of treatment in this regimen is 9-11 months with Intensive Phase (IP) at least 4 months and Continuation Phase (CP) for 5 months. Treatment extension of IP is done up to 2 months based on follow-up results and is indicated in the algorithm presented in the figure below.
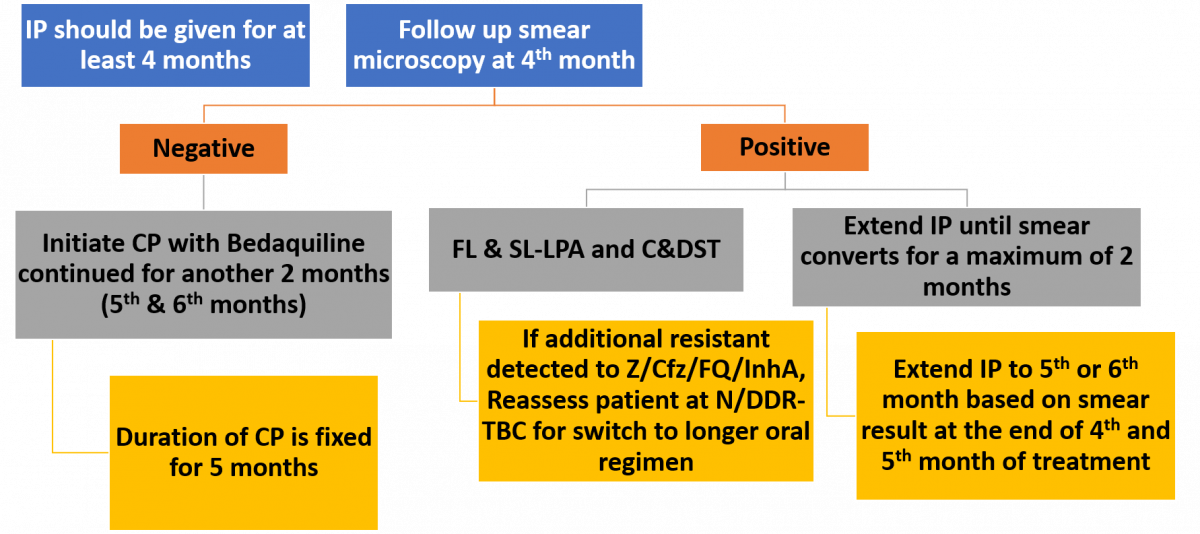
Figure: Treatment Extension/ Regimen Change Based on Follow up Smear/ Culture/ DST Results
Abbr: FL & SL- LPA- First Line & Second Line- Line Probe Assay, C&DST- Culture and Drug Susceptibility Test, Z- Pyrazinamide, Cfz- Clofazimine, FQ- Fluoroquinolone, N/DDR-TBC- Nodal/ District DR-TB Centre
Resources
- Guidelines for Programmatic Management of Tuberculosis in India, 2021.
- WHO Consolidated Guidelines on Tuberculosis: Module 4 – Treatment: Drug-resistant TB Treatment, 2020.
Shorter Oral Bedaquiline-containing MDR/RR-TB Regimen: Drug Dose Administration
ContentDrug dose administration for shorter/ longer oral Bedaquiline (Bdq)-containing Multidrug-resistant (MDR)/ Rifampicin-resistant (RR)-TB regimen depends on the factors described below.
- The dosage of second-line anti-TB drugs would vary as per the weight of the Drug-resistant TB (DR-TB) patients. There are five weight bands in adult patients (≥ 18 years): <16 kg, 16-29 kg, 30-45 kg, 46-70 kg and >70 kg. The weight bands of adult patients for Drug-sensitive TB (DS-TB) patients are different compared to DR-TB patients.
- All morning doses should be supervised by the treatment supporter via Directly Observed Treatment, Short-course (DOTS).
- In patients with drug intolerance, Cycloserine (Cs), Ethionamide (Eto) and Sodium (Na) Para Aminosalicylic Acid (PAS), can be given in two divided doses. Pyridoxine should be provided as part of the regimen till the end of treatment for all patients.
Change in Weight Bands during Treatment
- For adult DR-TB patients whose weight increases or decreases by 5 kg or more compared to baseline weight and crosses the current weight band during the course of the treatment, the weight band must be changed at the time of issuing next month's box to the treatment supporter of the patient.
- For paediatric patients, the drug dosage should be adjusted immediately once the weight of the patient crosses the range of the weight band. Counsel the patient about the change in dose.
Key Considerations for Newer Drugs
- Avoid milk-containing products with drugs: The calcium in the milk can decrease the absorption of Fluoroquinolones (FQs).
- Avoid large fatty meals: Fat impairs the absorption of anti-TB drugs (Cs, Isoniazid (H), etc.).
Resources
Shorter Oral Bedaquiline-containing MDR/RR-TB Regimen: Dosage of Drugs for Adults
ContentIn adults, the dosage of drugs for a shorter oral Bedaquiline (Bdq) - containing Multi-drug Resistant (MDR)/ Rifampicin-resistant Tuberculosis (RR-TB) regimen, varies according to their weight.
The table below provides drug dosages for adult patients, according to their weight bands, in a shorter oral Bedaquiline-containing MDR/RR-TB regimen.
Table: Weight-bandwise Dosages for Adult Patients on Shorter Oral Bdq-containing MDR/ RR-TB Regimen Sr No
Drugs
16-29 kg
30-45 kg
46-70 kg
>70 kg
1
High dose H (Hh)
300 mg
600 mg
900 mg
900 mg
2
Ethambutol (E)
400 mg
800 mg
1200 mg
1600 mg
3
Pyrazinamide (Z)
750 mg
1250 mg
1750 mg
2000 mg
4
Levofloxacin (Lfx)
250 mg
750 mg
1000 mg
1000 mg
5
Bedaquiline (Bdq)
Week 0–2: Bdq 400 mg daily
Week 3–24: Bdq 200 mg 3 times per week
6
Clofazimine (Cfz)
50 mg
100 mg
100 mg
200 mg
7
Ethionamide (Eto)*
375 mg
500 mg
750 mg
1000 mg
8
Pyridoxine (Pdx)
50 mg
100 mg
100 mg
100 mg
*Drugs can be given in divided doses in a day in the event of intolerance. Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- The Use of Bedaquiline in the Treatment of Multidrug-resistant Tuberculosis: Interim Policy Guidance, 2013.
Kindly provide your valuable feedback on the page to the link provided HERE
Possible Adverse Events Due to Drugs in Shorter Oral Bedaquiline-containing MDR/RR-TB Regimen
ContentDrugs that are part of the shorter Bedaquiline (Bdq)-containing regimen have some typical side effects which need close monitoring of Drug Resistant-TB (DR-TB) patients while providing the treatment.
Table: Possible adverse events due to drugs in the shorter oral Bedaquiline-containing MDR/RR-TB regimen; Source: Guidelines for PMDT in India, 2021.
Adverse Drug Events Causative Drugs QT prolongation Bdq, Fluoroquinolone (FQ), Clofazimine (Cfz) Rash, allergic reaction and anaphylaxis Any drug Gastrointestinal symptoms Ethionamide (Eto), Pyrazinamid (Z), Ethambutol (E), Bdq, Cfz, FQs, Isoniazid(H) Diarrhoea and/or flatulence Eto Hepatitis Z, H, Eto, Bdq Giddiness Eto, FQ, Z Hypothyroidism Eto Arthralgia Z, FQ, Bdq Peripheral neuropathy H, FQ, rarely Eto, E Headache Bdq Depression FQ, H, Eto Psychotic symptoms Isoniazid (H), FQ Suicidal ideation H, Eto Seizures H, FQ Tendonitis and tendon rupture FQ Vestibular toxicity (tinnitus and dizziness) FQs, H, Eto Optic neuritis E, Lzd, Eto, Cfz, H Metallic taste Eto, FQs Gynaecomastia Eto Alopecia H, Eto Superficial fungal Infection and thrush FQ Dysglycaemia and Hyperglycaemia Eto Resources
Kindly provide your valuable feedback on the page to the link provided HERE
-
Ph-Ch10: Longer Oral M/XDR-TB Regimen
FullscreenLonger Oral M/XDR-TB: Regimen and Duration
ContentLonger oral Multi (M)/ Extensive Drug-resistant (XDR) -TB treatment is specified with a definite regime and duration.
Regimen: (18-20) Levofloxacin (Lfx), Bedaquiline (Bdq) (6 months or longer), Linezolid# (Lzd), Clofazimine (Cfz), Cycloserine (Cs) (# dose of Lzd will be tapered to 300 mg after the initial 6–8 months of treatment)
- Duration: 18-20 months
- No separate Intensive Phase (IP) and Continuation Phase (CP).
- Bdq will be given for 6 months and extended beyond 6 months as an exception.
- Pyridoxine should be given to all Drug-resistant TB (DR-TB) patients as per the weight bands.
- For Extensively Drug-resistant TB (XDR-TB) patients, the duration of a longer oral XDR-TB regimen would be for 20 months.
Resources
- Guidelines for Programmatic Management of Drug-Resistant Tuberculosis in India, March 2021.
- WHO Consolidated Guidelines on Tuberculosis: Module 4 – Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Treatment Extension in Longer Oral M/XDR-TB Regimen
ContentThe total duration of a longer oral Multidrug/ Extensively drug-resistant TB (M/XDR-TB) regimen is 18–20 months.
Image
Figure: Protocol for Treatment Extension in Longer Oral M/XDR-TB Treatment Regimen
Extension of Bedaquiline (Bdq) beyond 6 months is to be considered in patients in whom an effective regimen cannot otherwise be designed.
- If any additional resistance to Group A, B or C drugs in use is detected, the patient needs to be reassessed at the Nodal/ District Drug-resistant Tuberculosis Centre (N/DDR-TBC) for modification of a longer oral M/XDR-TB regimen immediately on receiving the report.
- A treatment duration of 15–17 months after culture conversion is suggested for most patients. The duration may be modified according to the patient’s response to treatment.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- WHO Consolidated Guidelines on Tuberculosis: Module 4 – Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Adverse Drug Reactions due to Longer oral M/XDR-TB Regimen
ContentThe table below showcases the adverse drug events that may be caused by drugs used for longer oral Multi (M)/ Extensively Drug-resistant TB (XDR-TB) regimen. In these situations, replacement drugs are used instead of these drugs.
Table: Possible Adverse Drug Events in the Longer Oral M/XDR-TB Regimen
ADVERSE DRUG EVENTS
DRUGS
QT prolongation
Bedaquiline (Bdq), Fluoroquinolone (FQ), Clofazimine (Cfz) Rash, allergic reaction and anaphylaxis Any drug
Gastrointestinal symptoms
Ethionamide (Eto), P-Aminosalicylic Acid (PAS), Pyrazinamide (Z), Ethambutol (E), Bdq, Cfz, Linezolid (Lzd), FQs Diarrhoea and/or flatulence
PAS, Eto
Hepatitis
Z, Eto, PAS, Bdq
Giddiness
Amikacin (Am), Eto, FQ and/or Z
Haematological abnormalities
Lzd
Hypothyroidism
Eto, PAS
Arthralgia
Z, FQ, Bdq
Peripheral neuropathy
Lzd, Cycloserine (Cs), Am, FQ, rarely Eto, E
Headache
Bdq, Cs
Depression
Cs, FQ, Eto
Psychotic symptoms
Cs, Isoniazid (H), FQ
Suicidal ideation
Cs, Eto
Seizures
Cs, H, FQ
Tendonitis and tendon rupture
FQ
Nephrotoxicity (renal toxicity)
Am
Vestibular toxicity (tinnitus and dizziness
Am, Cs, FQs, Eto, Lzd
Hearing loss
Am Optic neuritis
E, Lzd, Eto, Cfz
Metallic taste
Eto, FQs
Electrolyte disturbances (Hypokalaemia and Hypomagnesaemia
Am
Gynaecomastia
Eto
Alopecia
Eto
Superficial fungal infection and thrush
FQ
Lactic acidosis
Lzd
Dysglycaemia and Hyperglycaemia
Eto
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- WHO Consolidated Guidelines on Tuberculosis: Module 4 - Treatment: Drug Resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Dosages of M/XDR-TB Drugs for Adult in Longer Oral M/XDR-TB Regimen
ContentIt is important to know the dosages of Multi (M)/ Extensively Drug-resistant TB (XDR-TB) drugs for adults on a longer oral M/XDR-TB regimen.
The table below shows the M/XDR-TB regimen drugs for adults weight band-wise, used in longer oral M/XDR-TB regimen customized for India by national experts.
Table: Dosages of M/XDR-TB Drugs for Adults in Longer Oral M/XDR-TB Regimen Sr.No
Drugs
16-29 kg
30-45 kg
46-70 kg
>70 kg
1
Levofloxacin (Lfx)
250 mg
750 mg
1000 mg
1000 mg
2
Moxifloxacin (Mfx)
200 mg
400 mg
400 mg
400 mg
3
High dose Mfx (Mfxh)
400 mg
600 mg
600 mg
600 mg
4
Bedaquiline (Bdq)
Week 0–2: Bdq 400 mg daily
Week 3–24: Bdq 200 mg 3 times per week
5
Clofazimine (Cfz)
50 mg
100 mg
100 mg
200 mg
6
Cycloserine (Cs)3
250 mg
500 mg
750 mg
1000 mg
7
Linezolid (Lzd)
300 mg
600 mg
600 mg
600 mg
8
Delamanid (Dlm)
50 mg twice daily (100 mg) for 24 weeks in 6-11 years of age
100 mg twice daily (200 mg) for 24 weeks for ≥12 years of age
9
Amikacin (Am)1
500 mg
750 mg
750 mg
1000 mg
10
Pyrazinamide (Z)
750 mg
1250 mg
1750 mg
2000 mg
11
Ethionamide (Eto)3
375 mg
500 mg
750 mg
1000 mg
12
Na - PAS (60% weight/ vol)2,3
10 gm
14 gm
16 gm
22 gm
13
Ethambutol (E)
400 mg
800 mg
1200 mg
1600 mg
14
Imipenem-Cilastatin (Imp-Cln)3
2 vials (1g + 1g) bd (to be used with Clavulanic acid)
15
Meropenems (Mpm)3
1000 mg three times daily (alternative dosing is 2000 mg twice daily) (to be used with Clavulanic acid)
16
Amoxicillin-Clavulanate (Amx-Clv) (to be given with Carbapenems only)
875/125 mg bd
875/125 mg bd
875/125 mg bd
875/125 mg bd
17
Pyridoxine (Pdx)
50 mg
100 mg
100 mg
100 mg
1For adults more than 60 years of age, the dose of Second-line Injectable (SLI) should be reduced to 10 mg/kg (max up to 750 mg).
2In patients of Para Amino Salicylic Acid (PAS) with 80% weight/ volume the dose will be changed to 7.5 gm (16-29 kg); 10 gm (30-45 Kg); 12 gm (46-70 kg) and 16 gm (>70 kg).
3Drugs can be given in divided doses in a day in the event of intolerance.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- WHO Consolidated Guidelines on Tuberculosis: Module 4 – Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
-
Ph-Ch11: Isoniazid (H) Mono/Poly DR-TB Regimen
FullscreenRegimen, Duration and Dosage for Isoniazid [H] Mono/Poly DR-TB Regimen
ContentIsoniazid (H) mono/ poly Drug-resistant TB (DR-TB) regimen has the following regimen, duration and dosage of drugs.
Regimen: (6 or 9) Lfx R E Z
Dosage
- The dosage of drugs would vary as per the weight of the patients.
- Adult patients (≥ 18 years) would be classified in weight bands of <16 kg, 16-29 kg, 30-45 kg, 46-70 kg and 70 kg. The drug dosages by these weight bands are shown in the table below.
- All drugs in the regimen are to be given on a daily basis under observation.
Table: Drugs used in H Mono/ Poly DR-TB Regimen by Weight bands for Adults. Source: Guidelines for PMDT, India, 2021, p79.
SR. NO
DRUGS
16-29 KG
30-45 KG
46-70 KG
>70 KG
1
Rifampicin (R)
300 mg
450 mg
600 mg
750 mg
2
Ethambutol (E)
400 mg
800 mg
1200 mg
1600 mg
3
Pyrazinamide (Z)
750 mg
1250 mg
1750 mg
2000 mg
4
Levofloxacin (Lfx)
250 mg
750 mg
1000 mg
1000 mg
Duration
- H mono/ poly DR-TB regimen is for 6 or 9 months with no separate Intensive Phase (IP)/ Continuation Phase (CP).
- In exceptional situations of unavailability of loose drug R or E or Z, the use of 4 FDC (HREZ) with Levofloxacin (Lfx) loose tablets may be considered as an option rather than not starting the H mono/ poly DR-TB patients on treatment.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- WHO Consolidated Guidelines on Tuberculosis: Module 4 - Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Adverse Drug Events: H Mono/Poly DR-TB Regimen
Contenthe potential adverse drug events that can occur when using drugs in the H mono/ poly DR-TB regimen are tabulated below:
Table: Possible Adverse Events due to Drugs in H Mono/ Poly DR-TB Regimen; Source: Guidelines for PMDT, India, 2021, p83.
ADVERSE DRUG EVENTS SUSPECTED DRUG(S) Hepatitis Rifampicin (R), Pyrazinamide (Z) QT prolongation Fluoroquinolone (FQ), Clofazimine (Cfz) Rash, allergic reaction and anaphylaxis Any drug Gastrointestinal symptoms Z, Ethambutol (E), Cfz, FQs Giddiness FQ, Z Arthralgia Z, FQ Peripheral neuropathy FQ, E Depression FQ Psychotic symptoms FQ Seizures FQ Tendonitis and tendon rupture FQ Vestibular toxicity (tinnitus and dizziness) FQ Optic neuritis E, Linezolid (Lzd), Cfz Metallic taste FQ Superficial fungal infection and thrush FQ Resources
- Guidelines for Programmatic Management of Drug Resistant Tuberculosis in India, March 2021.
- WHO Consolidated Guidelines on Tuberculosis: Module 4 - Treatment: Drug resistant TB Treatment, 2020.
- Technical and Operational Guidelines for TB in India, 2016.
Kindly provide your valuable feedback on the page to the link provided HERE
-
Ph-Ch12: TB Infection treatment and care
FullscreenTB Infection
Content-
TB Infection (or previously known as Latent TB infection) is a stage in between uninfected and having active TB. In this stage the person has no symptoms and can only be identified using laboratory tests.
-
The vast majority of infected people may never develop TB disease. However, to achieve TB elimination, it is important to treat TB infection in people at risk of developing active TB disease.
-
It is a state of persistent immune response to stimulation by Mycobacterium tuberculosis antigens with no evidence of clinically manifested active TB.
-
There is no single acceptable/reliable test for direct identification of Mycobacterium tuberculosis infection in humans. Tuberculin Skin Test (TST) and Interferon-gamma release assay (IGRA) are commonly used tests for identifying TB infection.
Resources:
-
Testing for TB Infection
ContentFor TB infection, there are two recommended tests which can be used to identify such patients.
Tuberculin Skin Test (TST)
The skin test is done by injecting a small amount (0.5 ml) of TB antigens into the top layer of skin on your inner forearm. If one has ever been exposed to TB bacteria (Mycobacterium tuberculosis), there will be a reaction indicated by the development of a firm red bump (induration) >= 10 mm at the site within 2 days.
Image
Figure: Tuberculin Skin Test
Interferon-gamma release assay (IGRA)
IGRA is a Blood test. If one has been exposed to TB bacteria, the white blood cell in the blood will release a substance called gamma interferon when the cells are exposed to specific TB antigens.
Image
Figure: Interferon-gamma release assay (IGRA)
Resources:
- Latent Tuberculosis Infection Guideline
- Guideline for Programmatic Management of Tuberculosis Preventive Treatment in India
Kindly provide your valuable feedback on the page to the link provided HERE
TB Preventive Therapy
ContentTPT treatment options recommended under NTEP include:
- 3-month weekly Isoniazid and Rifapentine (3HP)
- 6-months daily isoniazid (6H)

Table 1: TPT Options for Target Population; Source: (Guidelines for Programmatic Management of Tuberculosis Preventive Treatment)

Table 2: TPT dosage based on age and weight band recommended by NTEP; Source: Guidelines for Programmatic Management of Tuberculosis Preventive Treatment
Resources
- Guidelines for Programmatic Management of Tuberculosis Preventive Treatment
- National Strategic Plan for TB Elimination
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test TPT options recommended under NTEP include which of the following? 3-month weekly Isoniazid and Rifapentine (3HP) Rifampicin 6-months daily isoniazid (6H) 1 and 3 4 TPT options recommended under NTEP include 3-month weekly Isoniazid and Rifapentine (3HP) and 6-months daily isoniazid (6H). Yes Yes Target groups for TPT
ContentThe NTEP has prioritized the target population for TPT based on elevated risk of progression from infection to TB disease or increased likelihood of exposure to TB disease.
The target populations have been divided into two groups:
- Household contacts of bacteriologically confirmed pulmonary TB patients notified in Nikshay from public and private sector.
Target Population
Strategy
- People living with HIV (+ ART)
- Adults and children >12 months
- Infants <12 months with HIV in contact with active TB
- HHC below 5 years of pulmonary* TB patients
TPT to all after ruling out active TB disease - HHC 5 years and above of pulmonary* TB patients#
TPT among TBI positive# after ruling out TB disease #Chest X Ray (CXR) and TBI testing would be offered wherever available, but TPT must not be deferred in their absence
*Bacteriologically confirmed pulmonary TB patients to be prioritized for enumeration of the target population for TPT
- Expanded to other risk groups
Target Population
Strategy
Individuals who are:
- on immunosuppressive therapy
- having silicosis
- on anti-TNF treatment
- on dialysis
- preparing for organ or hematologic transplantation
TPT after ruling out TB disease among TBI positive
-
Ph-Ch13: TB-Comorbidities and special situations
FullscreenComorbidity & special situation with TB
ContentSeveral medical conditions are risk factors for TB and poor TB treatment outcomes. Similarly, TB can complicate the course of some diseases. Therefore, it is important to identify these comorbidities in people diagnosed with TB to ensure early diagnosis and improved outcomes. When these conditions are highly prevalent in the general population, they can significantly contribute to the TB burden. Consequently, reducing the prevalence of these conditions can help prevent TB.
TB shares underlying social determinants with many of these conditions. Addressing the social determinants of health is a shared responsibility across disease programmes and other stakeholders within and beyond the health sector.
Figure: Various comorbid and special situation related with tuberculosis
HIV in TB Patients
ContentThe primary impact of HIV on TB is that the risk of developing TB becomes higher in patients with HIV. Overall, HIV-infected persons have an approximately 8-times greater risk of TB than persons without HIV infection.
Screen TB PLHIV patients for symptoms of TB and HIV
Figure: Screening steps for TB - HIV patients
Treatment for TB HIV Patients
- All TB patients who have been diagnosed and registered under NTEP should be referred for screening for HIV.
- Referral of TB patients for screening for HIV and its recording & reporting is the responsibility of the Peripheral Health Institutions(PHI) where TB treatment is initiated.
- TB patients diagnosed with HIV will receive the same duration of TB treatment with daily regimen as non-HIV TB patients.
- TB patients must be referred to the nearest ART(Anti - Retroviral Treatment) centre for management of HIV.
Diabetes in TB Patients
ContentAs a consequence of urbanization as well as social and economic development, there has been a rapidly growing epidemic of Diabetes Mellitus(DM). India has the second largest number of diabetic people in the world.
Screen TB patients for symptoms of diabetes
Figure: Screening steps for TB - Diabetic Patients
Treatment for TB Diabetes Patients
- All TB patients who have been diagnosed and registered under NTEP will be referred for screening for Diabetes.
- Referral of TB patients for screening for DM and its recording & reporting is the responsibility of the Peripheral Health Institutions(PHI) where TB treatment is initiated.
- TB patients diagnosed with diabetes will receive the same duration of TB treatment with daily regimen as non-diabetic TB patients.
- TB patients must be referred to the nearest healthcare facility for management of DM.
- Regular monitoring of blood sugar levels is advised.
Malnutrition in TB Patients
ContentMalnutrition refers to deficiencies, excesses or imbalances in a person’s intake of energy and/or nutrients. The term malnutrition covers 2 broad groups of conditions.
- One is ‘undernutrition’—which includes stunting(low height for age), wasting(low weight for height), underweight(low weight for age) and micronutrient deficiencies or insufficiencies(a lack of important vitamins and minerals).
- The other is overweight, obesity and diet-related non communicable diseases (such as heart disease, stroke, diabetes, and cancer).
Screen TB Malnutrition patients for nutritional needs
Figure: Screening Steps for TB - Malnutrition patients
Treatment for TB Malnutrition Patients
Cases of TB with SAM and moderate undernutrition should be referred to the nearest health facility of NTEP for further management. Special focus should be given to the following categories:
- Children below five years
- School-age children and adolescents(Up to age 18 years)
- Adults, including pregnant and lactating women, with active TB and SAM
Alcoholism in TB Patients
ContentAbout 10% TB deaths globally have been attributed to alcohol as a risk factor(WHO, Global TB Report 2017). Alcohol abuse is associated with threefold increase in risk of contracting tuberculosis.
Side effects of anti TB drugs in this situation might get aggravated.
Figure: Impact of Alcoholism on TB patients
Treatment for Alcoholic TB Patients:
- Patients with TB and a history of alcohol use should be referred to the nearest health facility of NTEP to manage TB and alcoholism.
- While registering as a TB case, the status of alcohol use should be recorded in the patient records. If the TB patient is an alcohol user, he/she should be counselled to quit it. If the patient doesn't quit alcohol, s/he may be referred to the nearest alcohol de-addiction facility.
- The patient should be assessed at every follow-up visit for TB and the status of use of alcohol.
- At the end of treatment, his/her status of alcohol use should be recorded on the treatment card. If the patient has not quit alcohol, he/she should be referred to the nearest alcohol de-addiction facility and Alcohol Anonymous wherever available.
Tobacco in TB Patients
ContentAlmost 38% of TB deaths are associated with the use of tobacco. The prevalence of TB is three times higher among ever-smokers as compared to that of never-smokers. Mortality from TB is three to four times higher among ever-smokers as compared to never-smokers. Smoking contributes to 50% of male deaths in the 25-69 age group from TB in India.
Figure: Impact of Tobacco on TB patients
Treatment for TB - Tobacco Patients:
- While registering as a TB case, the status of tobacco use is recorded on the TB treatment card.
- If the TB patient is a smoker or tobacco user, he/she is counselled to quit tobacco use. The patient is assessed at every visit for follow up for TB and the status of tobacco use.
- At the end of treatment, his/her status of tobacco use is recorded in the treatment card. If the patient has not quit tobacco use, he/she will be referred to the nearest Tobacco Cessation Clinic(TCC) or Quit Line or M-Cessation Initiative.
Silicosis in TB Patients
ContentSilicosis is a progressive and disabling interstitial lung disease caused by inhalation and deposition in the lungs of particles of free silica.
Mutual Risk of TB and Silicosis
- TB is a clinical complication of silicosis, called silico-tuberculosis. Silica-exposed workers with or without silicosis are at increased risk for TB. There is also an increased risk of extrapulmonary TB in individuals exposed to silica.
- The risk of a patient with silicosis developing TB is 2.8 – 3.9 times higher than a healthy individual.
- The risk of TB relapse in patients with silicosis is approximately 1.5 times higher than in patients without silicosis.
The presence of silica particles in the lung and silicosis may:
- Facilitate initiation of TB infection and progression to active TB
- Exacerbate the course and outcome of TB, including prognosis and survival
Diagnosis
The diagnosis of silicosis is made based on a history of exposure to silica accompanied by a clinical and radiological profile consistent with the disease.
Under the Integrated Management Algorithm for TB disease and TB infection released by the National TB Elimination Programme (NTEP), patients with silicosis are first screened according to the four-symptom complex to rule out/in active TB and tested for TB accordingly.
If active TB is ruled out >> Refer for Tuberculin Skin Test (TST)/ Interferon Gamma Release Assay (IGRA) >> Positive test >> Evaluate with Chest X-ray (CXR) >> Commence TB Preventive Therapy (TPT) irrespective of CXR results.
CXR often indicates TB in silicosis patients earlier than the clinical symptoms, and regular radiographic screening is required for early TB detection. Radiographic comparison of serial films is done with particular attention to:
- Rapid appearance of new opacities, symmetric nodules or consolidation and the finding of pleural effusion or excavations.
- Cavitation is the strongest indicator of probable silico-tuberculosis.
Other diagnostic tools that can help in diagnosis are:
- Chest Computed Tomography (CT) scan
- Bronchoscopy with bronchoalveolar lavage in conjunction with transbronchial biopsy
- Spirometry
Treatment and Follow-up
To keep the disease from getting worse, all silicosis patients need to eliminate any more exposure to silica. Supportive measures include the use of cough medicines, bronchodilators, oxygen therapy and pulmonary rehabilitation.
TB treatment in patients with silicosis is challenging, perhaps due to impairment of macrophage function by free silica and/or poor drug penetration into fibrotic nodules. Usual anti-TB drugs with directly observed therapy are recommended but for an extended duration of at least 8 months, to reduce the chances of relapse.
Follow-up of patients with silicosis and TB follow the same schedule as is in prevailing guidelines.
Prevention
TB prevention in silicosis patients is essential and includes:
- Active surveillance of vulnerable groups including workers
- Adoption of measures to reduce exposure to silica dust
- Patients with silicosis are eligible for TPT after ruling out active TB
NTEP is in the process of engaging with the Ministry of Labour and Mining to identify high priority districts with stone crushing units/ mining industry. Specific guidelines will be developed to support persons with an occupational risk for TB and provide access, diagnosis and treatment services from the programme.
Resources
- NTEP at a Glance; Comprehensive Clinical Management Protocol of Tuberculosis, 2022.
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Silico-tuberculosis, Silicosis and Other Respiratory Morbidities Among Sandstone Mine-workers in Rajasthan - A Cross-sectional Study, Saranya Rajavel et al., 2020.
- Mini-review: Silico-tuberculosis; Massimiliano Lanzafame et al, 2021.
- Immunity to the Dual Threat of Silica Exposure and Mycobacterium tuberculosis, Petr Konečný et al., 2019.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following statement/s about silicosis and TB is/are incorrect?
TB is a clinical complication of silicosis, called silico-tuberculosis.
Silica-exposed workers with or without silicosis are at increased risk for TB and EPTB.
TB in patients with silicosis is easily diagnosed clinically as the patient coughs up silica particles.
TB treatment in patients with silicosis is often of extended duration to prevent relapse.
3
Clinical diagnosis of active TB superimposed on silicosis is often difficult, particularly in the initial phases, when clinical manifestations may not be indicative and radiological alterations can be indistinguishable from those due to the pre-existing silicosis.
Yes Yes Cancer in TB patients
ContentRelationship between Cancer and Tuberculosis (TB)
TB and malignancy may be related in the following four ways:
- TB as a marker for occult cancer: Occult cancer may lead to locally-reduced infection barriers and/or generalised immunosuppression, rendering a cancer patient susceptible to TB infection/ reactivation.
- TB as a risk factor for cancer: TB may increase the risk of cancer locally and systemically through chronic inflammation, fibrosis and production of carcinogenic molecules.
- Shared risk factors for TB and some cancers: Shared risk factors such as smoking, alcoholism, Chronic Obstructive Pulmonary Disease (COPD) and immunosuppression, including HIV, may lead to both TB and cancer, affecting both prevalent and subsequent cancer risk.
- Treatment of cancer-fueling TB: Many cancers are treated with immunosuppressants or steroids. These drugs might induce immunosuppression in the patients undergoing treatment for cancer and hence, a flare-up of TB.
Mutual Risk of Cancer and TB
- TB patients are 2-11 times more likely than non-TB patients to develop lung cancer, according to studies.
- After cancer diagnosis, the incidence of TB also increases, both in the short term and long-term.
- All types of cancer increase the risk of the development of active TB, but with varying degrees. Haematologic cancer patients had the highest rates of active TB, followed by head and neck cancers, lung cancer and breast cancer patients.
There is intrinsic immunosuppression due to the cancer itself, immunosuppressive effects of chemotherapy, or other host factors (e.g., smoking, malnutrition) that may increase the susceptibility to both cancer and TB. Thus, there is increased incidence of TB in cancer patients, and vice-versa.
Diagnosis of TB in Cancer Patients: Under the Integrated Management Algorithm for TB disease and TB infection released by the National TB Elimination Programme (NTEP), cancer patients are first screened according to the four-symptom complex to rule out/in active TB and all presumptive TB cases need to undergo testing for TB.
Co-existence of TB and cancer poses a diagnostic challenge since clinical and radiological presentations between TB and cancers are similar, hence the need for bidirectional screening. E.g., if biopsy specimens reveal infiltration by malignant cells, still send sample for microbiological confirmation of M. tuberculosis. Thus, allowing for accurate diagnosis and initiation of anti-TB treatment instead of attributing clinical deterioration to chemotherapy complications and progression of underlying malignancy.
Diagnosis of lung cancer in TB patients is usually done in consultation with a clinical specialist and can include examination of induced sputum specimens for malignant cells, as well as use of other diagnostic tools such as Computed Tomography (CT) scans, bronchoscopy, Positron Emission Tomography (PET) scans, Magnetic Resonance Imaging (MRI), histopathology and the use of biological markers.
Treatment
TB treatment in cancer patients uses the standard DS-TB/DR-TB regimens and course, except that the treating physician should assess the drug interactions between anti-TB and anti-cancer drugs. For cancer treatment, drugs may have to be modified to accommodate anti-TB treatment and to aid better prognosis of the TB outcome. However, all decisions must be taken by a competent specialist after examining the individual case.
Curative resection, chemotherapy and radiation therapy are the mainstay treatment options for cancer in TB patients. Co-existence of TB in cancer patients necessitates anti-TB treatment with extended duration, if required. Follow-up during and after treatment also follows prevailing guidelines.
Prevention
Under the NTEP, TB prevention in cancer patients is essential and includes:
- Regular screening for signs and symptoms of TB infection among all patients on immunosuppressive therapy and anti-Tumour Necrosis Factor (TNF) medicines.
- Education and referral of patients who do not have TB symptoms for TB infection testing/assessment of their eligibility for TPT.
Resources
- NTEP at a Glance; Comprehensive Clinical Management Protocol of Tuberculosis, 2022.
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Tuberculosis and Risk of Cancer: A Danish Nationwide Cohort Study, D. F. Simonsen et al., International Journal of Tuberculosis and Lung Diseases, The Union, 2014.
- Increased Risk of Active Tuberculosis after Cancer Diagnosis, Dennis F. Simonsen et al., Journal of Infection, 2017.
- Pulmonary Tuberculosis as Differential Diagnosis of Lung Cancer; MLB Bhatt et al., South Asian Journal of Cancer, 2012.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following statement/s about cancer and TB is/are incorrect?
Under NTEP, regular screening for signs and symptoms of TB infection among all patients on immunosuppressive therapy and anti-TNF medicines is done.
TB increases the risk of developing cancer, but cancer patients do not usually get TB.
Sputum smear microscopy is important when diagnosing TB in cancer patients.
All of the above
2
There is mutual risk between cancer and TB. TB increases the risk of developing cancer, and cancer patients are more likely to develop TB.
Yes Yes Pregnancy and Lactation in TB Patients
ContentThe presence of tuberculosis disease during pregnancy, delivery, and postpartum is known to result in unfavourable outcomes for both pregnant women and their infants. These outcomes include a roughly two-fold increased risk of preterm birth, low birth weight, intrauterine growth restriction, and a six-fold increase in perinatal death.
Screen TB patients in Pregnancy & Lactating Patients
Figure: Screening Steps in special situation - Pregnancy and Lactating TB Patients
Treatment for TB - Pregnant & Lactating Patients
- Cases of pregnant/lactating women with active TB should be referred to the nearest health facility of NTEP for further management.
- They should be continued on iron and folic acid and other vitamins and minerals to complement their maternal micronutrient needs.
- In situations when calcium intake is low, calcium supplementation is recommended as part of antenatal care.
COVID-19 in TB patients
ContentTuberculosis and COVID-19 are infectious diseases which primarily attack the lungs. They present with similar symptoms of cough, fever and difficulty in breathing, although TB disease has a longer incubation period and a slower onset of disease.
Screen patients for symptoms of TB and COVID-19
Figure: Screening steps for TB - COVID 19 Patients
Management of TB & COVID-19 Patients
People with TB are likely to be at increased risk of COVID-19 infection, illness and death. So, TB patients should take precautions as advised by health authorities to be protected from COVID-19 and continue their TB treatment as prescribed.
Prevention: While both TB and COVID-19 are spread by close contact between people, the exact mode of transmission differs. Thus, the patient should be explained the following measures to control disease spread.
- Apart from that keeping rooms well ventilated, avoiding crowds and Respiratory precautions are thus important in the control of COVID-19 and TB Disease
-
PHI Pharmacist : GENERAL CONCEPTS IN ADHERENCE MANAGEMENT
FullscreenTB Treatment Adherence
ContentTuberculosis(TB) is curable if patients are treated with effective, uninterrupted anti-tuberculous treatment. Treatment adherence is critical for curing individual patients, controlling the spread of infection in the community, and minimizing the development of drug resistance.
Adherence to treatment means that a patient follows the recommended course of treatment by taking all the prescribed medications for the entire length of time, as necessary. In other words, “right dose for the right duration”.
In Drug Sensitive Tuberculosis(DSTB), a TB patient completes 168 doses of TB treatment and adheres to TB treatment.
Importance of Treatment adherence
ContentAdherence to tuberculosis(TB) treatment is important for promoting individual and public health. Poor adherence to TB treatment results in:
- More individual suffering and death,
- Costly treatment as treatment regimens lengthen and
- Increases the risk for Drug Resistant Tuberculosis
Proper treatment of all forms of TB is critical to reducing individual morbidity and mortality and to interrupting transmission among family and community members.
Recording and Monitoring Adherence
ContentRecording of Treatment Adherence can be done as
- Manually by DOT/Health Care Provider in TB Treatment Card of a patient.
- Self-reported by Patient using digital tools for reporting adherence using 99 DOTS and MERM technologies.
Monitoring Treatment Adherence:
All TB patients should be monitored to assess their response to TB treatment. Nikshay Adherence calendar has a colour legend for various doses taken by a patient
Figure: Sample Nikshay Adherence Calendar in web and Mobile App
COLOUR LEGEND DOSE DESCRIPTION Treatment Start /End Denotes Treatment start and End Date Digitally Reported Dose Denotes that the patient has successfully called the Toll Free Number displayed on the envelope Manually Reported Dose Indicates that the staff has marked manually confirmed dose for the day Unreported Dose Indicates that there was no call event received on Nikshay for that day Manually Reported Missed Dose Indicates that the staff has marked a manually confirmed missed dose for the day Digitally Reported(From Shared Phone Number) Indicates that the patient has been calling from a shaed number(A mobile number that is common for more than one patient) Image
Figure: DSTB Treatment Card (Paper)
Digital Adherence Monitoring Technologies
Content99DOTS is a low-cost digital adherence technology built-in Nikshay that uses inexpensive packaging(envelopes or stickers) with medication that enables people taking medication to engage with their treatment daily. This packaging, distributed to TB patients taking medications, has a hidden number behind perforated flaps on the external envelope; in some cases, the number may be fixed outside the medication blister or pill bottle. This number can be a toll-free number that can be called to register daily adherence or a code sent by SMS, USSD, or other communication channels. Calling or messaging the number is free!
Figure: 99 DOTS Envelope
MERM: The Medication Event Reminder Monitor(MERM) is a digital pillbox that provides daily pill-taking reminders and facilitates remote monitoring of medication adherence. This system provides visual and audible reminders for both daily dosing and refill,.transmits this data to a server so that healthcare providers can remotely visualize patients’ dosing histories to support enhanced adherence counselling.
Figure: MERM Box
Recording manual doses in Nikshay
ContentManual recording of Adherence in Nikshay:
in Nikshay, Adherence can only be recorded only if there is corresponding dispensation being issued to a Patient
Figure: Steps to record manual dose in Nikshay
Recording in Patient Treatment Card:
Figure: Filled Treatment card for TB Patient
Recording missed doses in Nikshay
ContentMissed Dose recording in Nikshay:
For recording missed doses in Nikshay, following steps should be followed:
Treatment Support
ContentA person affected by TB requires support throughout the course of treatment and beyond that. The support to a TB patient is essential to ensure that s/he completes the treatment without affecting her/his quality of life (QoL). Keeping the patient as the central figure in the continuum of care, and ensuring social and personal circumstances are supportive (not only meeting immediate requirements of medical treatment) is the key to treatment support.

Figure: Key Components of Treatment Support
Resources
National Strategic Plan for Tuberculosis Elimination 2017–2025, RNTCP, 2017.
A Patient-centred Approach to TB Care, WHO, 2018.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
DOT is the only treatment support provided to TB patients.
True
False
2
Ensuring social and personal circumstances are supportive for treatment adherence and not just medical requirement is the key to treatment support.
Treatment supporter to TB Patient
ContentA Treatment Supporter can be any person such as a Medical Officer, MPWs, community volunteers working with the program etc. Even a patient’s relative or family member can be a Treatment Supporter.
As per NTEP guidelines, salaried NTEP/General Health System staff may also be assigned as treatment supporters for a patient. However, they will not be eligible for any honorarium.
A patient can only be linked to one treatment supporter at a time in Nikshay.
-
-
M-3: PHI Pharmacist: General concepts and Principles of SCM in NTEP
Fullscreen-
Ph-Ch15: Key Concepts and Principles in SCM
FullscreenSupply Chain Management
ContentSupply Chain Management (SCM) is the handing of flow of goods and material from point of origin to point of consumption, with the objective to ensure that the supplies are present for utilization without any interruption. It covers everything from procurement and sourcing of raw materials to delivery of final product to the consumer, along with the related logistics. It will also include the related information systems that enable monitoring and exchange of information.
Effective SCM ensures the following:
- Continuous availability of quality-assured medicines/ products at the right time and at all healthcare levels.
- Minimizes wastage by preventing expiry of drugs at all levels, maintenance of adequate stock levels and accurate records.
- Maximizes patient care by coordination in all departments and by minimizing human errors/ medication errors.
- Economically viable by minimizing monetary loss (e.g., through pilferage) and optimizing cost via bulk purchasing or according to consumption needs.
Robust supply chain management systems have two main components:
- Physical flow: Involved the movement and storage of supplies
- Information flow: Allows the various stakeholders to coordinate and control the flow of supplies
Resources
- NTEP Training Modules 1-4 for Programme Managers & Medical Officers, 2020.
- NTEP Training Modules 5-9 for Programme Managers & Medical Officers, 2020.
- Guidelines for Programmatic Management of Drug-resistant TB, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following statements are correct about supply chain management?
It is useful to ensure a continuous supply of good quality medicines.
It is an essential activity that must be undertaken by health programmes.
It helps reduce the cost burden on the healthcare system.
All of the above
4
Effective SCM is an essential activity that ensures a continuous supply of good quality medicines and cost optimization.
Drug distribution flow
ContentUnder the National TB Elimination Programme (NTEP), the anti-TB drugs are procured at the centre level by the Central TB Division (CTD), Ministry of Health and Family Welfare (MoHFW), and supplied to the central warehouses.
From the central level warehouses, the drugs are supplied to different State Drug Stores (SDS) and further distributed to District Drug Stores (DDS) and sub-district level (TB Unit (TU) Store and Peripheral Health Institute (PHI)).
This movement of drug flow is monitored in real-time through Ni-kshay Aushadhi.

Figure: Flowchart Showing the Overview of Distribution of Drugs
Abbr: CMSS: Central Medical Services Society; GDF: Global Drug Facility; CTD: Central TB Division; GMSD: Government Medical Store Depot; SDS: State Drug Store; DDS: District Drug Store; TU: TB Unit; PHC: Primary Health Centre; PHI: Peripheral Health Institute.
Resources
Stock types
ContentVarious stocks are maintained at different levels. To facilitate the monitoring of the quantity of these stocks, these are classified as follows:
- Active Stock: It refers to those stocks which have passed all quality parameters and those which are ready to use/ dispatch for consumption. This is the heart of a warehouse and mostly uses the major chunk of storage. The First Expiry First Out (FEFO) principle will apply to this section of the drug stock.
- Quarantine Stock: The stock which is pending for quality testing or not yet prepared for active usage is called quarantine medicines. This stock is kept in a separate area that is called the quarantine area and is not to be disbursed for usage until they are declared as active stock.
- Safety Stock: Buffer stock or safety stock is the amount of stock or medicine set aside to meet the requirements of the facility/ store at the time of an emergency like unforeseen demand or depleting stock. However, this stock should be frequently checked for expiry and replenished at right time to prevent its expiry.
- Damaged Stock: The medicines or stocks which are found damaged during the delivery at a particular facility/ warehouse in terms of packaging/ leakage/ broken, are to be identified and kept separately as damaged stock. The idea is to return them to the supplier with the proper Damage Stock Report Form. The pharmacist needs to mark such damaged stock in the delivery challan at the time of the receipt.
- Substandard Stock: Substandard medicines/ items are products that do not meet the quality standards and specifications. These items should be kept separately to avoid their use. These stocks need to be reported to the parent store. As per the directions, these stocks either need to be returned to the supplier or disposed of in accordance with the biomedical waste management guidelines.
- Lost in Transit Stock: It refers to the stock which is either misplaced/ lost during transportation. The pharmacist needs to report such stock in the delivery challan at the time of the receipt and the same needs to be reported to the supplying store immediately.
- Expired Stock: Ideally, the warehouse should not have an expired medicine/ item if a proper FEFO mechanism is adopted for dispatch. However, in certain situations, drugs/ items may get expired and may not be suitable for usage as recommended by the manufacturer. Such stock is called Expired Stock. These expired drugs/ items need to be kept separately in a demarcated area and are labelled as expired drugs/ items and are to be disposed of, in accordance with the prevailing biomedical waste disposal guidelines after obtaining necessary approvals.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct Answer
Explanation Page ID
Part of Pre-Test
Part of Post-Test
Which of the following is true regarding the use of medicines which are kept in quarantine?
Can be used in an emergency.
Can be used before the quality test result.
Can never be used.
Can be used if the particular item passes the quality test or is declared as active stock.
4
Quarantine medicines are not to be disbursed for usage until they are declared as active stock. Yes
Yes
Minimum and maximum stock
ContentMinimum Stock
A minimum stock level is a threshold value that indicates the level below which actual medicine stock should not normally be allowed to fall.
In other words, a minimum stock level is a minimum quantity of a particular drug/ medicine that must be kept at all times.
The main factors to consider when fixing the minimum stock level are:
- Average consumption
- Time needed to procure/ receive from supplies/ reporting facility, i.e., Lead time
- Reorder level (a fixed stock level between the maximum and minimum stock levels, at which a request for supply will be placed)
The minimum stock level can be calculated by applying the following formula:
Minimum Stock Level = Reorder level - (Average consumption per time period under consideration x Time taken for delivery)
(time period may be day/ week/ month/ quarter)
Maximum Stock
A maximum stock level is the upper limit of stock that should not be exceeded under normal circumstances without the prior agreement of the management.
The aim of setting a maximum stock level is to maintain the inventory level at the warehouse.
The main factors to consider when fixing the maximum stock level are:
- Average consumption
- Availability of storage space
- Economic order quantity
- Time needed to procure/ receive from supplies/ reporting facility
- Cost of carrying inventory or cost of storage
The maximum stock level can be calculated by applying the following formula:
Maximum Stock Level = Reorder level + Reorder quantity - (Minimum consumption per time period under consideration x Minimum time taken for delivery)

Figure: Stock Re-ordering Level; Source: Inventory Management.
Resources
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
The stock of drugs should not normally fall below the minimum stock level.
True
False
1
A minimum stock level is a threshold value that indicates the level below which actual medicine stock should not normally be allowed to fall. In other words, a minimum stock level is a minimum quantity of a particular drug/ medicine that must be kept at all times.
Yes
Yes
First Expiry First Out [FEFO]
ContentThe principle of First-Expired, First-Out (FEFO) means that the drugs which are due to expire first, are to be issued first.
The FEFO principle ensures that the product with the shortest expiry date is utilised at the earliest within its shelf-life.
Following the FEFO principles, the stocks need to be placed/ arranged/ stacked in a sequential manner.
Steps Followed for Implementing FEFO
Image
- Check Expiry Date
- The expiry date of the stock need to be checked at the time of receipt of supplies with the release order/issue voucher.
- The ‘Expiry Dates’ should be marked in bold letters, 3” to 4” in size, on the drug cartons with a marker pen, for easy identification and control of drugs immediately on their arrival.
- The pharmacist need to record for expiry date of the stock in the Ni-kshay Aushadhi or in stock register.
- Storing Supplies with Different Dates of Manufacture and Expiry in Different Batches
- Different batches of supplies with different dates of manufacture and expiry should be stored separately.
- Supplies that are past their date of expiry should never be stored with the items which are still being used and the storekeeper should ensure that there is no stocking of supplies beyond their date of expiry.
- Checking the Utilisation Pattern Before Issuing Drugs
- The storekeeper should strictly follow FEFO principles to ensure that all short-expiry drugs should be distributed to the State/ District/TU/ Peripheral Health Institute based on the utilisation pattern of each.
- The storekeeper is also expected to install appropriate tools to periodically monitor controls over the expiry position of drugs held in stocks mainly through storage of drugs of a particular description at one place, expiry-wise stacking and marking expiry dates on cartons/ drug boxes with marker pens.
- The Pharmacist need to check for Expiry date from the physical stock and Ni-kshay Aushadhi prior to issue.
- In case of short-expiry supplies, the distribution should be on the rational basis keeping in view the utilization pattern to ensure judicious consumption.
- Frequent Checks/ Physical Verification
- Frequent check and physical verification to be carried out by the supervisory officer on regular basis. This ensures that the older drugs are being used first and that none of the drugs are past their date of expiry.
Resources
- Module for STS - Part 2: Ensuring Proper Registration and Reporting, CTD, MoHFW, India.
- Training Modules (5-9) for Programme Managers and Medical Officers, CTD, MoHFW, India.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test The principle of FEFO means that the 'drugs which are due to expire first, are to be issued first.’ TRUE FALSE 1 The principle of FEFO means that the 'drugs which are due to expire first, are to be issued first.’ Yes Yes - Check Expiry Date
Management of short expiry drugs
ContentThe short expiry drugs are the drugs which are left with a short shelf-life and need to be utilised immediately to avoid their expiry.
Shelf-life of a drug is defined as a period during which the drug will last without deterioration, provided all precautions for good storage practices have been undertaken. The shelf-life of anti-TB drugs ranges from 3-5 years after which the chances of losing efficacy and probability of side effects increase rapidly. Therefore, it is important to ensure that appropriate steps are taken as soon as the drugs reach the critical stage to ensure their usage well within their shelf-life.
Identification of Short Expiry Drugs
- Short expiry depends on two main factors, duration of the treatment and the time taken for transit from one level to the next lower level, i.e., from State Drug Stores (SDS) to the District TB Centre (DTC) --->Tuberculosis Unit (TU) ---> Peripheral Health Institute (PHI).
- Whenever the drugs are dispatched, the transit duration (approx.3 months), possible treatment interruption (approx. 1 month), a probable extension of the Intensive Phase (1 month) and the buffer stocking norm under each facility should be taken into account, to calculate if the drug is expiring shortly.
Principles of Management of Short Expiry Drugs
- For the drugs whose expiry date is mentioned only as month and year, the last day of that particular month should be considered as the date of expiry.
- Expiry-wise stacking of the drugs, marking of expiry dates on cartons/ drug boxes with marker pens and periodic monitoring of the expiry position of the drugs.
- The expiry date should be highlighted in yellow to flag attention to the drugs facing the risk of expiry.
- First-Expiry-First-Out (FEFO) principle should be strictly followed in the case of short-expiry drugs which means the drugs near to expiry should be issued first.
- All the details about the drug quantity and expiry date should be recorded and reported in Ni-kshay Aushadhi.
- A review of drug adequacy should be conducted monthly/quarterly by the officer in charge to identify any stock imbalances or excessive short expiry drugs and implement corrective measures accordingly.
- The distribution of short expiry drugs on a rational basis, keeping in view the utilisation pattern of each district to ensure timely consumption of close to expiry drugs.
Resources
- Standard Operating Procedure Manual Procurement & Supply Chain Management, CTD, MoHFW, India, 2018.
- Procurement, Supply Chain Management & Preventive Maintenance, Module 6, CTD, MoHFW, India.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test If the date of expiry is mentioned as 'Dec-2022', what is the last date of expiry for that drug? 1-Dec-2022 10-Dec-2022 31-Dec-2022 None of the above 3 For the drugs whose expiry date is mentioned only as month and year, the last day of that particular month should be considered as the date of expiry. Yes Yes Maintaining buffer stock
ContentBuffer stock refers to a reserve that is used in unforeseen emergencies. It is also known as strategic stock or safety stock. This mandates close monitoring of drug stocks and maintaining buffer stock at all levels following the stocking norms to ensure an uninterrupted supply of drugs.

Importance of Maintaining Buffer Stock
- To cover for delays/ disruptions (if any) in the supply chain.
- To manage instances where more patients are initiated on treatment than the actual expected patients in a particular month.
- To ensure that no patient is sent back due to a shortage of drugs at any point in time.
- For smooth functioning of the programme on a national level.
Buffer stock to be maintained at different levels under NTEP
For adult drugs ( 3-3-2-2) State Drug Store District Drug Store Tuberculosis Unit Peripheral Health Institution 3 months 3 months 2 months 1 month For paediatric drugs (3-3-4) 3 months 3 months 4 months Not stocked at PHI level Resources
- Standard Operating Procedure Manual Procurement & Supply Chain Management, CTD, MoHFW, India, 2018.
- Guidelines for PMDT in India, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
At the state level, it is essential to maintain buffer stocks equivalent to how many months?
1
2
3
4
3
At the state level, buffer stocks equivalent to 3 months at SDS should be maintained.
Yes
Yes
Lead time
ContentLead time is defined as the time interval between the order generation for a product and its receipt/ availability for use. Lead time for a product depends upon the type of product, quantity available in the market/ manufacturer and the weather conditions in which it is transported.
In supply chain management lead time plays a very important role as it is mandatory to place reorders in time to avoid stocking out the product. Poorly managed lead time can lead to stock out and leads to delays in supplying the product to clients or end users.
Lead Time = Reordering delay (Time period) + Supply Delay (Time period)

Figure: Lead Time in Supply Chain Management
Benefits of Reduction in Lead Time
- Minimises stock-outs
- Helps to get medicines/ items on time
- Reduces the wastage of inventory
- Gives the estimation of demand
How to Reduce the Lead Time
- Stop ordering surplus inventory
- Keep an eye on the inventory level
- Cut out as many steps as possible
- Maintain the inventory as per the storage capacity
- Continuous follow-up with the supplier or the facility
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct Answer
Correct explanation Page ID
Part of Pre-Test
Part of Post-Test
Poorly managed lead time leads to stock-outs.
True
False
1
Poorly managed lead time can lead to stock out and leads to delays in supplying the product to clients or end-user. Yes
Yes
Nikshay for drug dispensation to patients
ContentN-ikshay platform has a module for drug dispensation to patients. This feature is used for:
- Adding details of the product and quantity of drugs issued to patients.
- Printing and downloading the details of drugs dispensed as a prescription to share with the patients.
- Saving the time spent in repetitive data entry by copying previous dispensation details.
- Logging details of drugs that are returned by patients.
- Ensuring timely dispensation of drugs to patients by accessing the list of patients whose refill is due through the ‘Refill Due Task List’.
The stepwise details of adding dispensation are shown in the figure below.
Image
Figure: Workflow for "Add Dispensation" on Ni-kshay; Source: Ni-kshay Portal.
Steps for Dispensation to Patients in Ni-kshay
- Click on the ‘Add Dispensation’ button.
- Search by episode ID or dispensation ID.
- Enter dispensation details:
- Enter the “Date of Prescription”.
- The type of regimen gets auto-populated based on the test results.
- Enter the “Date of Dispensation”.
- “Weight Band” is getting auto-populated.
- The phase also gets auto-populated based on the test.
- Enter the “Current Weight”.
- Enter drug issuing facility details.
- Select the State.
- Select the District.
- Select the “Drug Issuing Facility Type”.
- Select the “Drug Issuing Facility Name”.
- Enter Product Details.
- Click on “Add” if required to add more product(s).
- Select the “Source” from the list.
- Select the prescribed product name from the drop-down option, it is a mandatory field.
- It is an auto-populated field based on the chosen product.
- Enter the “Quantity” as per the prescription, it is a mandatory field.
- Select the quantity less than or equal to the available quantity.
- Enter Refill Details.
- Enter the dosing start date as per the prescription, it is a mandatory field.
- Enter the number of days of dispensation as per the prescription, it is a mandatory field.
- Enter remarks, if any.
In case a patient returns drugs, the same can be recorded under Return Dispensation.
Resources
Assessment
Question
Answer 1
Answer 2
Correct Answer
Correct Explanation
Page ID Part of Pre-Test
Part of Post-Test
Ni-kshay can be used for entering details of drugs returned by patients
TRUE
FALSE
1
Ni-kshay drug dispensation module is used for:
- Adding details of the product and quantity of drugs issued to patients.
- Printing and downloading the details of drugs dispensed as a prescription to share with the patients.
- Saving the time spent in repetitive data entry by copying previous dispensation details.
- Logging details of drugs that are returned by patients.
- Ensuring timely dispensation of drugs to patients by accessing the list of patients whose refill is due through the ‘Refill Due Task List’.
Yes
Yes
Essentials for Inventory Management
ContentInventory Management (IM) is a systematic approach to ordering, receiving, storing, issuing and reordering drugs and other commodities. IM is a critical element in supply chain management which ensures the availability of the right products in the right place at the right time.
Image
Figure: Overview of Inventory Management in NTEP
Abbr: SDS: State Drug Store; DTC: District Tuberculosis Centre, NTEP: National Tuberculosis Elimination Programme.
Under the National TB Elimination Programme (NTEP), IM refers to the activities carried out by the officer-in-charge of logistics and includes the following:
- Determination of Stock Status at the SDS and DTCs/ Subordinate Stocking Points: The pharmacist will determine the drug stock status of their store and of all the sub-units up to PHIs through Ni-kshay Aushadhi.
- Review of Adequacy of Stock: The Pharmacist will analyse the adequacy of stocks on the basis of the available stock and estimated consumption as per the stocking norms.
- Correction of Imbalances through Transfers: Based on the review of drug adequacy, the officer-in-charge will flag all the sub-stores that are significantly under or overstocked.
- The needs of sub-stores flagged as understocked will be addressed through the Additional Drug Request (ADR) or Drug Transfer Advice (DTA) mechanism.
- The stocks at the sub-stores flagged as overstocked or with close to expiry drugs will also be corrected by the DTA mechanism.
- These transfers will only be authorised by the State TB Officer (STO)/ District TB Officer (DTO)/ officer-in-charge and should be recorded in Ni-kshay Aushadhi.
- Replenishment of Stock: The stocks at the stores are replenished on a quarterly basis, pursuant to the review and validation of the reports available in the Ni-kshay Aushadhi.
Resources
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which drug-stocking point/s are required to fill the QRPML?
SDS
DDS
TU
All the above
4
For the purpose of IM, all the drug-stocking points are required to fill and submit Quarterly/ Monthly Report on Programme Management & Logistics (QRPML).
Yes
Yes
-
Ph-Ch16: Drugs and consumables in NTEP
FullscreenTypes of drugs and consumables in NTEP
ContentNational TB Elimination Programme (NTEP) has established a robust supply chain management to ensure an uninterrupted supply of drugs and consumables across the country.
The drugs, diagnostic equipment, etc., are procured mainly through the central level and the states are granted permission to procure some consumables through the local state or district level while abiding by the NTEP guidelines.
1. Anti-TB Drugs
The various type of anti-TB drugs are classified as follows:
Image
2. Consumables
Various consumables used are:
Image
Resources
- Standard Operating Procedure Manual Procurement & Supply Chain Management, CTD, MoHFW, India, 2018.
- Procurement, Supply Chain Management & Preventive Maintenance, Module 6, CTD, MoHFW, India.
- Guidelines on Programmatic Management of Drug-resistant TB (PMDT) in India, NTEP, CTD, MoHFW, India, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which group of second-line drugs does Delamanid belong to?
Group A
Group B
Group C
Group D
3
Delamanid is a Group C second-line drug.
Yes
Yes
Drugs, injectables and related supplies in NTEP
ContentUnder the National TB Elimination Programme (NTEP) a comprehensive supply management system is maintained through Ni-kshay Aushadhi wherein all the stocking points and implementing health facilities are required to update the stock utilisation, consumption, requirement and expiry on a near to real-time basis. The requirement of all items at all levels is then calculated based on the data reported.
Injectables under NTEP
- The injectables used in TB treatment under NTEP are as follows:
- Amikacin
- Streptomycin
- Kanamycin
- Capreomycin
- Amongst these, Amikacin and Streptomycin, have been downgraded to Group C under the World Health Organisation's (WHO) reclassification of anti-TB drugs and are not included if an adequate regimen can be built without them.
- Kanamycin and Capreomycin are also no longer recommended for use.
- They are currently used only in special situations where the regimen cannot be completed and are supplied as Type B boxes.
- The District TB Officer (DTO) is responsible for issuing the injectables and the Peripheral Health Institute Medical Officer (PHI-MO) along with the Directly Observed Treatment (DOT) provider is responsible for making suitable arrangements during the intensive phase of the treatment for daily injections.
Other Related Supplies
- The other supplies required whenever the injectable TB treatment regimen is used are as follows:
- Water container
- Disposable tumblers
- Sterile water
- Disposable needles and syringes
- Cotton
- Methylated spirit
- In order to ensure accurate DOT, the DOT centre should have all the related supplies matched to the number of injection vials that are stocked in the centre.
- There should also be a sufficient number of disposable needles and syringes for giving injections along with cotton and methylated spirit to ensure that the injections are always given under sterile conditions.
- An adequate supply of sterile water, with enough water containers and disposable tumblers, must be ensured.
Procurement Injectables and Related Supplies under NTEP
The procurement of second-line drugs under the programme is done centrally depending on the policies and funding mechanism either through the Central Medical Services Society (CMSS) or through the Global Drug Facility (GDF). These are then distributed to implementing levels via State Drug Stores (SDS), District Drug Stores (DDS), Tuberculosis Unit (TU) and PHI. Other treatment-related supplies can also be procured at the state/ district level following NTEP guidelines/ General Financial Rules (GFR).
Resources
- Standard Operating Procedure Manual Procurement & Supply Chain Management, CTD, MoHFW, India, 2018.
- Procurement, Supply Chain Management & Preventive Maintenance, Module 6, CTD, MoHFW, India.
- Guidelines on Programmatic Management of Drug-resistant TB (PMDT) in India, CTD, MoHFW, India, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
All the injection-related supplies should be matched to the number of injection vials stocked.
True
False
1
All the injection-related supplies should be matched to the number of injection vials stocked.
Yes
Yes
- The injectables used in TB treatment under NTEP are as follows:
Laboratory consumables
ContentThe National TB Elimination Programme (NTEP) laboratory network is composed of National Reference Laboratories (NRLs) at the national level, at the state level Intermediate Reference Laboratories (IRLs) and Culture & Drug Susceptibility Testing (C&DST) laboratories and at the peripheral level Designated Microscopy Centres (DMCs).
Each of these laboratories is responsible for performing various functions at its own levels.

Figure: Flowchart of Laboratory Consumables
Table: Laboratory Consumables
Laboratory Consumables
Description
- Cartridge-based Nucleic Acid Amplification Tests (CBNAAT) machines and Cartridges
- The CBNAAT machines and cartridges are procured by Central TB Division (CTD) and supplied to state/ district/ CBNAAT sites based on their requirement.
- Cartridges are supplied based on the stock availability, consumption and expected case load.
- Recording, reporting and monitoring of cartridges are done through Ni-kshay Aushadhi.
- Binocular Microscope (BM) and LED Fluorescence microscopy (LED-FM)
- The procurement of both items is undertaken by CTD and then delivered to the states/ districts.
- All LED-FM/ BMs should be covered by annual maintenance contracts by states/districts, at the end of their warranty periods.
- NTEP guideline recommends 1 BM for every Designated Microscopy Centre (DMC) and LED FMs only for the high case load facilities with >25 slides per day.
- Along with public sector DMCs, NTEP may also supply BMs to DMCs established in other sectors like ESIS, Public Sector Undertakings, Medical College, etc., if required.
- Sputum containers
Calculation of requirement of sputum containers:
For diagnosis:
- During the first week of each quarter, the number of new pulmonary smear-positive cases registered and treated during the last quarter in the district should be determined and this number should be multiplied by 10.
- 10 is the average number of symptomatic required to be examined for detecting one case of new pulmonary smear-positive tuberculosis and it includes all types of patients.
- Since two sputum specimens are taken for each symptomatic patient, further multiply the number obtained above by 2.
- The final number derived would be the required no. of slides for diagnosis.
For follow-up:
- Two follow-up specimens are taken for the majority of patients (one at the end of the intensive phase and the other at the end of treatment), therefore one sputum container is needed for each follow-up.
- On the last working day of the quarter, count the number of sputum containers in stock and subtract from the required number as calculated above.
- Allow sufficient reserve stock for three months, add 10% to account for wastage of sputum containers, and account for the sputum containers in stock.
- Slides
- One slide is used to examine one specimen in a sputum container. Therefore, order a slightly higher number of slides, than the required no. of sputum containers to account for unavoidable breakage of slides.
- Order for both sputum containers and slides should be placed during the first week of the quarter.
- The supplies will be procured by the state/ district and supplied to all the peripheral health institutions in the district.
Resources
- Training Module (1-4) for Programme Managers and Medical Officers, NTEP, MoHFW, 2020.
- Procurement, Supply Chain Management & Preventive Maintenance, Module 6, CTD.
- Module for Laboratory Technicians, CTD, MoHFW, India, 2005.
- Standard Operating Procedure Manual Procurement & Supply Chain Management, CTD, MoHFW, India, 2018.
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Identify the correct statement from the options given below.
The CBNAAT machines and cartridges are procured at the district level as per the requirement.
The CBNAAT machines and cartridges are procured centrally and supplied to state/ district/ CBNAAT sites based on their requirement.
The CBNAAT machines and cartridges are procured at the Designated Microscopy Centre level as per the requirement.
The CBNAAT machines and cartridges are procured at the Tuberculosis Unit level as per the requirement.
2
The CBNAAT machines and cartridges are procured centrally and supplied to state/ district/ CBNAAT sites based on their requirement.
Yes
Yes
99 DOTS and MERM boxes
Content99 DOTS
99 DOTS is an IT-enabled ‘pill-in-hand’ adherence monitoring system implemented by the National TB Elimination Programme (NTEP) for all Drug-sensitive TB (DS-TB) patients on a daily regimen.
Mechanism of 99 DOTS
- In this system, the medicine blister packs (Figure 1) are wrapped with envelopes which have unique toll-free phone numbers printed on them.
- Each time a patient dispenses the pills, they break through perforated flaps on the back of the envelope, revealing a hidden phone number.
- The patient is expected to give a call to this toll-free number from his/her registered mobile number to report that they have consumed the medication.
- This is documented and updated against the patients’ adherence record in Ni-kshay.
- The sequence of hidden numbers cannot be predicted by patients but is known by the system for each month of medication prescribed.
- If the call is not received from the patients by 3:00 p.m., an SMS reminder is sent to the patients on their registered mobile number.
- If the patient still does not consume medications, the issue is escalated to the authority chain till corrective action is taken.
- Additionally, the patient can also be remotely followed up with help of Call Centres or using an Interactive Voice Response (IVR).
Printing of 99 DOTS Envelopes
- Specification for the printing of 99 DOTS envelopes is provided by Central TB Division (CTD) to all states and the envelopes are printed at the state level and then distributed to the districts.
- The cost of printing and distribution of these envelopes should be budgeted in the state Programme Implementation Plan (PIP).
Advantages of 99 DOTS
- Enables the NTEP staff to prioritise patients who need to be visited and counselled.
- Empowers patients to be able to take charge of their own treatment.

Figure1: 99-DOTS Blister Pack

Figure 2: Colour-coded adherence calendar output of 99-DOTS patients based on calling
Medication Event Reminder Monitor (MERM) Box
The Medication Event Reminder Monitor (MERM) Box is an electronic pill box specially designed to monitor Multidrug-resistant TB (MDR-TB) treatment.
Mechanism of MERM
- Medications are dispensed in blister packs and each drug is placed in a different partitioned compartment within the pillbox.
- The MERM box contains a removable electronic battery-powered module when triggered by a magnetic sensor captures and stores data each time the container is opened, as a proxy for medication ingestion.
- The MERM is programmed to provide audio-visual reminders to the patients to take medications at a specific time of the day.
- The visual reminder consists of:
- Green light: Corresponds to a label encouraging the patient to take a dose.
- Yellow light: Alerts patients about the need to refill medications.
- Red light: Indicates a low battery and the need to replace the MERM’s battery.
- The audio reminder consists of a ringing sound that would occur at the same time as the visual dose-taking reminder.
- The data from the MERM boxes is transmitted every 72 hours using cellular networks and recorded on a computer server.
- Each patient’s adherence history is presented as a colour-coded calendar (Figure 2) in which:
- Green suggested that the MERM was opened on a given day: Suggesting probable medicine was consumed.
- Red suggested that the device was not opened: Suggesting that medicine was probably not consumed.
- In case there is a series of possible missed doses, i.e., red-coloured calendar days, it would result in automated SMS notifications to the patients and also prompt the system to address the interrupting patients who are potentially at higher risk for unfavourable outcomes.
Advantages of MERM box
- Facilitates the identification of high-risk patients and prompt intervention by the system to improve adherence.
- Facilitates storage and organisation of the multiple medications of the MDR-TB regimens.
- Reduces the required frequency of patient visits to a health facility in comparison to facility-based DOT.

Figure 3:Medication Event Reminder Monitor (MERM) Box
Resources
- Procurement, Supply Chain Management & Preventive Maintenance, Module 6, CTD, MoHFW, India.
- 99DOTS: A Low-Cost Approach to Monitoring and Improving Medication Adherence. In Tenth International Conference on Information and Communication Technologies and Development (ICTD ’19), Cross et al., Ahmedabad, India, 2019.
- 99 DOTS. International Journal of Contemporary Medical Research, 2016;3(9):2760-2762.
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What is the meaning of ‘Red-coloured calendar days’ received through the MERM box data?
Series of consumed doses.
Series of missed doses.
Series of missed calls to the toll-free number.
None of the above
2
Red-coloured calendar days in the MERM box data mean a series of missed doses.
Yes
Yes
General stocks and materials
ContentInformation Education and Communication (IEC) Materials
- The purpose of the IEC materials is to create awareness and disseminate information about the disease (signs and symptoms) diagnosis, and treatment to increase accessibility and utilisation of services among the general population.
- IEC material also encourages the build-up of health-seeking behaviour among the masses in keeping with the focus on promotive and preventive health.
- Under IEC, posters, flyers, leaflets, brochures, booklets, etc. are printed and circulated. It is the responsibility of the state to print IEC material in various languages and distribute it among the general population.
- The surplus material is stored at the State Drug Store (SDS) for further distribution as and when required.
Printed Materials
As per the National TB Elimination Programme (NTEP) norms, the districts must use several forms and registers to record the diagnostic and treatment activities. In addition to these, the districts should maintain an adequate supply of printed material for the latest programmatic guidelines. These include the following:
Forms
- NTEP request for examination of biological specimens: Used to request tests such as sputum smear microscopy, Nucleic Acid Amplification Test (NAAT), Line Probe Assay (LPA), culture and Drug Susceptibility Test (DST).
- Treatment card (TB and Drug-resistant TB (DR-TB)): This card contains important information about a patient, such as their name, age, sex and address; type of disease; regimen prescribed; duration of treatment; etc.
- Patient’s identity card (TB and DR-TB patients): The front part of the ID card has patient information, name and address of the TB Unit (TU)/ district and treatment details of the patient including disease classification, type of patient, sputum results, category and information on the date of starting treatment. The back portion of the ID card has the results of the follow-up sputum examination, appointment dates for visits for drug administration and treatment outcome.
- Referral form for treatment (TB and DR-TB): Used when referring patients for treatment to other peripheral health institutions.
- Transfer form: This form is to be used when transferring registered patients on treatment from one reporting unit to another.
- TB notification forms
Registers
- Tuberculosis laboratory register: Used to record the results of sputum smear examinations at the microscopy centres
- Culture and DST laboratory register: Used to record the results of NAAT, LPA, culture and drug sensitivity testing
- Tuberculosis notification register: Contains information on all TB patients registered in the area
- Stock register: Used for recording the information on the stock of drugs and consumables received and issued by the health unit
- Reconstitution register: Used for recording the receipt of drugs of patients who have defaulted, died, failed treatment or transferred out
- Referral for treatment register: Maintained in all big hospitals and medical colleges where large numbers of cases are expected to be diagnosed and referred for treatment to other reporting units
Tablets
NTEP has provided tablet computers to all the key staff with the objective to support the system of capturing important information on a real-time basis. Distribution and storage of these tablet computers is another activity of the drug stores.
Programmatic guidelines
- Technical and Operational Guidelines
- National Guidelines on Programmatic Management of Drug-resistant TB
- National Guidelines on Partnerships
- Desk Reference (Charts on diagnostic algorithm, dosage of anti-TB drugs, any other)
- Laboratory Manual for Sputum Smear Microscopy and NTEP Laboratory Network guidelines for Quality Assurance of smear microscopy for diagnosing TB
- Guidance document on Nutrition Support to TB patients
- Other relevant documents/ guidelines/ circulars circulated by the Central TB Division (CTD).
It is the responsibility of the state to determine once a year the number of forms and registers that would be needed during the following year. The states must ensure that there is an adequate supply of all the forms, registers and guidelines within the state and that sufficient funds are available for the same.
Once printed, all the forms, registers and guidelines are stored at the SDSs from where they are further distributed to the districts and other health units.
Resources
- Technical and Operational Guidelines for Tuberculosis Control, Central TB Division, Ministry of Health and Family Welfare, Government of India, 2005.
- Training Modules (5-9) for Programme Managers & Medical Officers. Central TB Division, Ministry of Health and Family Welfare, Government of India, 2020.
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What is the purpose of the referral form for treatment?
Referring patients for treatment to other peripheral health institutions.
Transferring registered patients on treatment from one reporting unit to another.
Both 1 and 2
None of the above
1
The referral form for treatment is used when referring patients for treatment to other peripheral health institutions.
Yes
Yes
Various stocking points in NTEP
ContentUnder the National TB Elimination Programmme (NTEP), there are various stocking points at different levels which help in the storage and distribution of supplies to ensure their uninterrupted availability at all levels.
The various stocking points under NTEP are:
Image
Abbr: GMSD: General Medical Stores Depot; CMSS: Central Medical Services Society; SDS: State Drug Store; DDS: District Drug Store; TU: TB Unit; PHI: Peripheral Health Institute; HF: Health Facility.
Resources
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which stocking point/ points have a reserve stock of drugs for three months?
State Drug Store
District Drug Store
TU Drug Store
Both state and district drug stores
4
As per the standard NTEP norms, both SDS and DDS should have a reserve stock of drugs for three months.
Yes
Yes
-
PHI Pharmacist : INFORMATION SYSTEMS IN NTEP SCM
FullscreenNi-kshay Aushadhi
ContentNi-kshay Aushadhi is a web-based portal that deals with the management of stocks (anti-TB drugs, consumables and other commodities) across all the stocking points across the National TB Elimination Programme (NTEP), i.e., Government Medical Store Depot (GMSD), Central Medical Services Society (CMSS) warehouses, State Drug Stores (SDS), District Drug Stores (DDS), TB Units (TUs) including Peripheral Health Institutes (PHIs).
Ni-kshay Aushadhi also helps in real-time management of stock position, providing expiry details of commodities, routine/ Additional Drug Request (ADR) Requirements, and patient-wise consumption of drugs at all levels.
Table 1: Nikshay Aushadhi Stakeholders
User Services Central TB Division (CTD)
1. Quantification
2. Purchase Order (PO) generation
3. Quality control
4. State warehouse Drug Transfer Advice (DTA)
5. Monitoring of nation-wide stock & expiry
CMSS warehouse
1. Quantification
2. Purchase request generation
3. Advance shipment details
4. Supplier delivery details
5. Release Order (RO) to SDS
6. Acknowledge desk
7. Transfer of drugs to other warehouses
GMSD
1. Quantification
2. Acknowledge desk
3. Advance shipment details
4. Transfer of drugs to other warehouses
Supplier
1. View Purchase Order (PO) and delivery schedule
2. Enter dispatch details
3. View receipt
4. Demand vs issue
SDS/ DDS/ Drug-resistant TB Centre (DR-TBC)/ TU
1. Routine/ ADR & dispatch to sub-stores
2. Acknowledge desk
3. Transfer of drugs to other warehouses
4. Issue voucher DTA
5. Box preparation, box modification, unpacking and box completion
6. Local purchase
PHI
1. Routine/ ADR
2. Acknowledge the receipt of drugs
3. Issue to patient
4. Return from patient
The Ni-kshay Aushadhi can be used for the following purposes:
- Quantification and forecasting
- Monitoring and distribution
- Data management and analysis
- Recording and reporting of the drugs related data
- Training and capacity building
- Quantification of drugs
- Issue/ dispatch
- Return of drugs
- Drug request management - Routine/ ADR
- Stock management (like drug inventory, Physical Stock Verification (PSV))
- Packaging/ repackaging
- Receive from store/ Acknowledge desk
- Quality control management
Image
Figure: Supply chain management in NTEP through Ni-kshay Aushadhi; Source: Ni-kshay Aushadhi Manual
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct Answer Correct Explanation Page ID Part of Pre-Test Part of Post-Test Ni-kshay Aushadhi can be used for the quantification and forecasting of drug stocks. True False 1 The Ni-kshay Aushadhi can be used for the following purposes:
- Quantification and forecasting
- Monitoring and distribution
- Data management and analysis
- Recording and reporting of the drugs-related data
- Training and capacity building
- Quantification of drugs
- Issue/ dispatch
- Return of drugs
- Drug request management - Routine/ ADR
- Stock management (like drug inventory, PSV)
- Packaging/ Repackaging
- Receive from store/ Acknowledge desk
- Quality control management
- Miscellaneous
Yes Yes Nikshay Aushadhi - Alert Dashboard
ContentNi-kshay Aushadhi offers a utility-based broadcasting window that alerts the user about the management of event-based and job-based activities that need immediate attention.
This utility in Ni-kshay Aushadhi is known as the Alert Dashboard and primarily gives alerts about drugs with near expiry and drug acknowledgements that are pending.

Figure: Ni-kshay Aushadhi Alert Dashboard; Source: Ni-kshay Aushadhi Portal.
Drug expiry alert: This alert lists out all the drugs from the inventory of the store that is going to expire in the next three months. The utility of this alert is to make necessary arrangements beforehand that will ensure that these drugs are utilized before their expiry dates.
Acknowledgement pending alert: This alert lists out all the transfers/requests made by different sources whose acknowledgement is pending for more than 15 days.
Resources
Ni-kshay Aushadhi Manual, Central TB Division, Ministry of Health and Family Welfare, Government of India
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
The drug expiry alert lists out the drugs that will expire in what duration? Next 3 months Next 3 days
Next 3 years
Next 3 weeks
1
Drug expiry alert lists out all the drugs from the inventory of the store that is going to expire in the next three months.
Yes
Yes
Nikshay Aushadhi-Reports
ContentNi-kshay Aushadhi allows the users to view a number of autogenerated reports.
These reports available under the Acknowledgement desk of Ni-kshay Aushadhi are listed below:

Figure 1: Reports in Ni-kshay Aushadhi

Figure 2: Reports section in Ni-kshay Aushadhi; Source: Ni-kshay Aushadhi Portal.
Definition of the Reports
Report
Description
Expiry Details
This report gives the description of expired drugs in the store. The report can be viewed on the basis of drug categories and for any facility mapped with the store
Stock in Hand Record
This report gives a description of available drug stocks in the store. The report can be viewed on the basis of drug categories and for any facility mapped with the store
Stock Ledger Report
This is a digital stock register wherein you can check all the details relevant to a specific drug during a specified period of time. The details include opening balance, received quantity, issued quantity, and closing balance.
Issue Register
This is a digital record of supplies issued by a Store to its mapped stores and facilities
Box Preparation Register
This is a digital record of drug boxes prepared by a store.
Damaged/ Lost Item Details
This is a digital record of damaged and lost items at a particular store. The report can be viewed on the basis of the drug category and for any facility mapped with the store.
Receive from Third Party Report
This is a digital record of receipt of supplies from any facility mapped as a third party with a particular store. The report can be viewed separately for all the mapped third parties and for a specified duration of time.
Transfer Order
This report is a digital record of outward transfers made by a store.
Issue to Third Party Report
This is a digital record of supplies issued to any facility mapped as a third party with a particular store. The report can be viewed separately for all the mapped third parties and for a specified duration of time.
Receipt Register
This is a digital record of supplies received by a store. The receipts can be viewed on the basis of category as well as for a specified period of time.
Write-Off Details
This is a digital record of drugs condemned by the stores.
Resource
Ni-kshay Aushadhi Manual, Central TB Division, Ministry of Health and Family Welfare, Government of India.
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What does the stock ledger report contain?
Opening and closing balance
Received quantity
Issued quantity
All the above
All the above
A stock ledger is a digital stock register wherein you can check all the details relevant to a specific drug during a specified period of time. The details include opening balance, received quantity, issued quantity, and closing balance.
-
-
M-4: PHI Pharmacist: Inventory Management in NTEP
Fullscreen-
Pharmacist: Overview of Inventory managament in NTEP
FullscreenEssentials for Inventory Management
ContentInventory Management (IM) is a systematic approach to ordering, receiving, storing, issuing and reordering drugs and other commodities. IM is a critical element in supply chain management which ensures the availability of the right products in the right place at the right time.
ImageFigure: Overview of Inventory Management in NTEP
Abbr: SDS: State Drug Store; DTC: District Tuberculosis Centre, NTEP: National Tuberculosis Elimination Programme.
Under the National TB Elimination Programme (NTEP), IM refers to the activities carried out by the officer-in-charge of logistics and includes the following:
- Determination of Stock Status at the SDS and DTCs/ Subordinate Stocking Points: The pharmacist will determine the drug stock status of their store and of all the sub-units up to PHIs through Ni-kshay Aushadhi.
- Review of Adequacy of Stock: The Pharmacist will analyse the adequacy of stocks on the basis of the available stock and estimated consumption as per the stocking norms.
- Correction of Imbalances through Transfers: Based on the review of drug adequacy, the officer-in-charge will flag all the sub-stores that are significantly under or overstocked.
- The needs of sub-stores flagged as understocked will be addressed through the Additional Drug Request (ADR) or Drug Transfer Advice (DTA) mechanism.
- The stocks at the sub-stores flagged as overstocked or with close to expiry drugs will also be corrected by the DTA mechanism.
- These transfers will only be authorised by the State TB Officer (STO)/ District TB Officer (DTO)/ officer-in-charge and should be recorded in Ni-kshay Aushadhi.
- Replenishment of Stock: The stocks at the stores are replenished on a quarterly basis, pursuant to the review and validation of the reports available in the Ni-kshay Aushadhi.
Resources
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which drug-stocking point/s are required to fill the QRPML?
SDS
DDS
TU
All the above
4
For the purpose of IM, all the drug-stocking points are required to fill and submit Quarterly/ Monthly Report on Programme Management & Logistics (QRPML).
Yes
Yes
Stocking Norms
ContentThe National TB Elimination Programme (NTEP) strives to ensure an uninterrupted supply of drugs, and stocking norms have been developed by the Central TB Division (CTD) to help achieve this goal.
The drug stocks equivalent to 10 months of consumption, shall be maintained with implementing states.
The table shows the quantity of reserve stocks at each level at the start of the quarter (considering the receipt from one higher level).
Table: Stocking norms for First line anti-TB drugs for adults to be followed at each level Level Stock for Utilisation (Months) Reserve Buffer Stock (Months) Drug Requirements State Drug Store (SDS) 0 3 (Quarterly consumption / 3) X 10 – (existing stock in SDS including stocks at all districts at end of the quarter) District Drug Store (DDS) 0 3 (Quarterly consumption / 3) x 7 – (Existing stock in District TB Centre (DTC), TB Unit (TU) and Peripheral Health Institution (PHI) drugstores at end of the quarter) TU Drug Store 0 2 (Quarterly consumption / 3) x 4 – (existing stock in TU including PHI drug stores at end of the quarter) PHI 1 1 (Monthly consumption x 2) – (existing stock in PHI at end of the month) Based on the state stock availability and consumption, the stock is supplied from SDS to the district drug store to its TUs and then to the PHIs. This stocking pattern may be denoted as the 3-3-2-2 (SDS-District-TU-PHI) inventory-stocking norm, aggregating 10 months of inventory at the state level.
- At the start of the quarter, PHIs are supplied with a stock of 2 months (as shown in the table above)
- Every month, they are supplied with stock from the TU based on consumption, which helps to maintain 1 month reserve stock for utilization at the PHI
- This reserve stock helps the PHI to provide drugs if more patients are put on treatment in a particular month and to provide cover for delays in supplies from TU
- Thus, no patient is sent back due to a lack of drugs
- For the TU level to ensure that the PHIs have 1-month utilization stock plus 1-month reserves, it needs to have a reserve stock of 2 months at the beginning of the quarter
- In this way, the continuous supply of drugs is maintained
Paediatric Stocking Norms
Paediatric drug stocks equivalent to 10 months' consumption will also be kept, but paediatric boxes are not expected to be kept at PHI levels. The stocking of paediatric boxes has been limited to the TU level only.
The paediatric stocking pattern may be denoted as the 3-3-4 (SDS-District-TU) inventory stocking norm, aggregating 10 months of inventory at the state level.
Table: Stocking Norms for Second-line Anti-TB Drugs for Adults; to be Followed at Each Level. Level Stock for utilisation Reserve stock Drug requirements SDS 0 Months 3 months (Quarterly consumption/3) X 12 – (existing stock in SDS including stokes at all districts at the end of the quarter) DTC drug store 0 Months 3 months (Quarterly consumption/3) X 9 – (existing stock in DTC drug store including TU & HF drugs stores at the end of the quarter) TU drug store 0 Months 2 months (Quarterly consumption/3) X 6 – (existing stock in TU including HF drugs stores at the end of the quarter) Health facility 0 Months 2 months Reserve stoke in HF at the end of the month Treatment supporter 2 months 0 Months Two-monthly PWB under utilisation Figure: Stocking Norms for Second-line Anti-TB Drugs for Adults; to be Followed at Each Level
Abbr: TU: TB Unit; DTC: District TB Centre; SDS: State Drug Store; PWB: Patient-wise Box; HF: Health Facility.
Level
Stock for utilization
Reserve stock in months of full TPT courses
Drug requirements
Treatment supporter
One full TPT course per beneficiary
0 month
Full TPT course under utilization
HF drug store
0 month
2 month
Reserve stock in HF at end of the month
(2 x total TPT beneficiaries on Full TPT course for HF)
TU drug store
0 month
2 months
(Quarterly consumption/ 3) x 5 – (existing stock in TU including HF drug stores at end of the quarter)
DTC drug store
0 month
3 months
(Quarterly consumption/ 3) x 8 – (existing stock in DTC drug store including TU & HF drug stores at end of the quarter)
SDS
0 month
3 months
(Quarterly consumption/ 3) x 11 – (existing stock in SDS including stocks at all districts at end of the quarter)
Figure: Stocking norms for full TPT courses at various stocking points
Resources:
- NTEP Training Modules 5-9 for Programme Managers & Medical Officers, 2020.
- Standard Operating Procedures Manual for State Drug Stores, NTEP, 2012.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test How much stock of first-line anti-TB drugs should be available at a PHI at any given moment? 1 2 3 4 2 2 months' stock of drugs must be available at the PHI level Which of the following stocking norms are implemented by the NTEP? 2-2-3-4 (SDS-District-TU-PHI) inventory-stocking norm 2-3-4 (SDS-TU-PHI) inventory stocking norm 3-3-4 (SDS-District-TU) inventory stocking norm None of the above 3 The paediatric stocking pattern may be denoted as the 3-3-4 (SDS-District-TU) inventory stocking norm, aggregating 10 months of inventory at the state level.
-
PHI Pharmacist : INDENTING AND RECEIPT
FullscreenIndenting in NTEP
ContentAn indent is an official order or requisition for medicine and supplies from a medical store and the process of requesting is called indenting.
Under National Tuberculosis Elimination Programme (NTEP), online indenting of drugs and consumables is done using the Ni-kshay Aushadhi web portal.
There are different types of requests raised through Ni-kshay Aushadhi:
- Quarterly request
- From State to Central TB Division (CTD), District Drug Store (DDS) to State Drug Store (SDS) and Tuberculosis Unit (TU) to District Drug Store (DDS) on a quarterly basis.
- Quarterly replenishment of drug stocks with districts shall be based on the reports submitted by them in NI-kshay Aushadhi, providing complete details of opening and closing stocks, receipts, consumption and anticipated requirement.
- Monthly request
- From Peripheral Health Institution (PHI) to DDS on a monthly basis.
- Additional Drug Request (ADR)
- Supplies to District TB Centres (DTCs) against Additional Drug Requests (ADRs): There are likely to be occasions when the quarterly supply of drugs to DTCs as above, is insufficient to meet the needs of the district and additional drugs are required in advance of the next quarterly shipment. In such cases, the concerned DTC is required to prepare and submit an Additional Drug Request to the State TB Officer (STO), providing details in support of the supplementary requirement.
- The need for an ADR arises only if the more patients put on treatment in the previous month in a quarter goes up, resulting in an insufficient stock in the store. To get the additional supply from CTD/ SDS/ DDS/ TU, an ADR for each item needs to be submitted by the SDS in charge/ District TB Officer (DTO)/ Medical Officer- Tuberculosis Control (MO-TC). Before sending the ADR, one should consider and track the drugs that have been already released and are being transported from central/ state/ district/ TU stores.

Figure: Different Types of Drug Requests as Part of Indenting in NTEP through Ni-kshay Aushadhi Web Portal; Source: Ni-kshay Aushadhi Portal.
Resources
- Standard Operating Procedures Manual for State Drug Stores, Central TB Division, MoHFW, GoI, 2012.
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What is the mode of indenting in NTEP?
Through phone call
Through Ni-kshay Aushadhi's web portal
Through letter
Through email
2
Under National Tuberculosis Elimination Programme (NTEP), online indenting of drugs and consumables is done using the Ni-kshay Aushadhi web portal.
Yes
Yes
- Quarterly request
Process of Requesting Supplies
ContentProcess of Requesting Supplies in Ni-kshay Aushadhi
Depending upon the requirement of drugs and other supplies, the following two types of requests are generated through Ni-kshay Aushadhi:
1. Request for routine quarterly supplies
After the analysis of information provided in the QRPML, the pharmacist determines the drug requirements of the district for the next quarter and accordingly generates a request for the supply of the same through Ni-kshay Aushadhi. Such requests are known as the request for routine quarterly supplies.
2. Request for the supply of additional drugs/Additional Drug Requests (ADR)
In case, the quarterly supply of drugs is insufficient to meet the needs of the district, additional drugs are required. A request generated on Ni-kshay Aushadhi for the supply of these requests is known as Additional Drug Requests (ADR).
Process overview

Detailed stepwise procedure:
Step 1: Go to the Ni-kshay Aushadhi website and click on login. Enter your user ID, Password, and then captcha text and click login.
Step 2: Reach the Quarterly/Monthly/ADR Request window following the path Home>Services>Drug request Management> Quarterly/Monthly/ADR Request Advice and select your store. Click on the ‘generate request’ tab to raise a new request.

Figure 1: Creating a new drug request; Source: Ni-kshay Aushadhi Portal.
Step 3: Specify the type of the request (quarterly/monthly requests or ADR), select the indenting store and press the 'go' tab.
Step 4: A list of the drugs will appear in the subsequent window. Choose the drug(s) to be requested either by searching the name in the search tab or by selecting the drug(s) directly from the list. Fill in the average quarterly consumption and the required quantity of the drug in the relevant fields and click save to generate the indent.

Figure 2: Drug requesting window in Ni-kshay Aushadhi; Source: Ni-kshay Aushadhi portal
The indent generated can be viewed, modified, or cancelled from the main menu of ‘Quarterly/ Monthly/ ADR Request Advice, window.

Figure 3: Indent generated
Source: Ni-kshay Aushadhi portal
Resource
Ni-kshay Aushadhi Manual-Central TB Division, Ministry of Health and Family Welfare, Government of India.
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
The request for drugs is put on which window of Ni-kshay Aushadhi? Quarterly/Monthly/ADR request advice window Acknowledge desk
Dispatch desk
None of the above
1
Reach the Quarterly/Monthly/ADR Request window following the path Home>Services>Drug request Management> Quarterly/ Monthly/ ADR Request Advice and select your store.
Yes
Yes
Procedures following the receipt of supplies
ContentThe State Drug Store (SDS) pharmacist should follow certain procedures after receipt of supplies.

Figure 1: Overview of procedures following receipt of supplies by a State Drug Store (SDS)
Visual Inspection :
- The check shall be limited to visual inspection and count of the number of cartons received and matching the same with the Issue Voucher and Challan. The Storekeeper will not ordinarily open sealed cartons unless the seal and/or exterior suggest damage or shortage or there have been frequent shortages observed in the recent past.
- In case, where the GMSD/CMSS has opted to make part shipments, the Storekeeper shall record details of drugs received and the balance quantity pending supply. The Storekeeper shall follow-up closely with the supplier.
Shortages and/ or transit damages:
- In the case of shortage/ damage determined by the Storekeeper through visual inspection s/he shall take the precaution of opening the seals of all cartons received and carefully checking their contents down to the lowest packaging unit.
- Ideally, SDS should take custody only of undamaged stock from the perspective of the drugs in question being in a good enough condition to be administered to patients. SDS storekeeper shall segregate and preserve damaged stocks till further instructions are received.
Recording and Reporting
- In the case of shortage/ damage/ discrepancy in the quantity of drugs actually received vis-à-vis that indicated as per the transmission/ authorization document, record complete details of the same in the ‘Remarks’ column of the SR & NA and highlight the same.
- In case transmission documents are received prior to receipt of drugs, entry shall not be made in the SR on the basis of such documents viz. RO, Issue Voucher / Challan.
- Alternatively, if drugs are received prior to receipt of transmission documents, entry in SR shall be made only after their receipt and confirmation as to the quantity supplied by respective sending unit.)
Resources
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which document should be received before or along with the consignment from GMSDs?
State Issue Voucher (SIV)
CTD-Release Order (CTD-RO)
District Issue Voucher (DIV)
Quarterly Report on Programme Management & Logistics (QRPML)
2
Upon the receipt of consignment from GMSDs the pharmacist will ensure that a release order from the CTD-Release Order (CTD-RO), issued by the Central TB division is received either before or along with the consignment.
Yes
Yes
-
PHI Pharmacist : ISSUE AND CONSUMPTION
FullscreenConsumption of supplies
ContentNTEP provides quality drugs to all the diagnosed TB patients without any interruption. Under NTEP, 1st line drugs are being provided in monthly blister strips of Fixed Dosage Combination (FDC) for Drug Sensitive TB patients according to their weight-bands. For drug resistant TB patients, drugs are provided in monthly boxes depending upon their weight-band and resistance pattern (Mono-resistance, poly-drug resistance, Multi Drug Resistance, Extensive Drug Resistance).
Different Supplies are utilized at different locations.
Supplies to patient from PHI
Patients to receive drugs for the treatment of drug sensitive TB or drug resistant TB by DOTS Provider or Treatment Supporter as per the regimen prescribed by the doctor. The DOTS Provider or Treatment Supporter shall receive drugs from Peripheral Health Institution (PHI). PHIs shall issue drugs on monthly basis against the unique Notification ID generated by Nikshay through Nikshay Aushadhi.
Supplies to ART Centre
Drugs which are required to be issued to Anti Retroviral Therapy (ART) Centre for the TB-HIV patient under collaboration of TB and National AIDS Control Organization (NACO), will require to be issued through Nikshay Aushadhi in order to capture the stock being consumed by these ART centres. Programme is in integration NACO and in future Nikshay Aushadhi shall have direct request from ART Centre through their system and accordingly, drug shall be released.
Supplies to Private Sector and Supplies to Lab
Private pharmacies will be involved in dispensation of anti-TB drugs supplied from NTEP to give access to TB patients who seek care in private sector, after consultation with private practitioners. To support the pharmacies for arranging such mechanism for keeping NTEP supplied Fixed Dose Combination (FDC), District TB Officer (DTO) may consider incentives to such pharmacies. NTEP should also arrange for regular uninterrupted drug supply. Monthly PHI report should be used for drug inventory management.
Supplies to Lab
Cartridges/chips are supplied based on the stock availability, consumption and expected cases load. Recording, reporting and monitoring of cartridges/chips is done through Nikshay-Aushadhi.
Supplies to Nodal/District Drug-Resistant TB Centres (N/DDRTBC)
Drugs are issued to the DDSs/NDRTBC based on requirement. At the same time drugs are received from Government Medical Store Depots (GMSDs) .
The drugs are also issued to patients from DR-TB centres, such as Bedaquline or Delamanid. In Nikshay Aushadhi application, the DRTB stores are mapped onto a PHI login id. A DRTB centre which is associated with a PHI, is added on that PHI login id. The user can select the stores either PHI or DRTB, as per the requirement, to use any process.
Medical supplies to Non-TB patents:
The State Drug Store (SDS) shall supply full courses of TB Preventive Therapy (TPT) per person with a buffer stock of 3 months to all the districts on quarterly basis, districts will supply further with a buffer stock of 2 months to all TUs on monthly basis and TUs will supply further with a buffer stock of 2 months to all Health Facility on a monthly basis.
Resources
1. Nikshay Aushadhi User Manual
2. NTEPTrainingModules5to9 Central TB Division, MoHFW, GoI 2020
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Consumption of supplies available at PHI store TU store
DDS
NDRTBC
All of the above
Consumption of supplies available at all levels Adding and Printing Dispensation
ContentVideo fileReturning Dispensation
ContentVideo fileAdd and view prescription
ContentVideo fileVideo : Add and view prescription
Dispensation Correlation
ContentVideo fileViewing Refill Task List
ContentVideo file
-
PHI Pharmacist : STOCKING NTEP DRUGS IN PRIVATE SECTOR
FullscreenStocking NTEP drugs in private sector-Overview and significance
ContentOverview of National TB Elimination Program (NTEP) Drug Logistics for Private Sector
The partnership option envisioned under NTEP should ensure an uninterrupted supply of anti-TB drugs at the state/ district/ sub-district and facility level for private sector facilities.
- For private practitioners/ medical stores/ other partners registered as Peripheral Health Institute (PHI) under Ni-kshay, drugs will be issued from their concerned TB Units (TUs).
- For non-registered private practitioners/ medical stores/ other partners under Ni-kshay, drugs will be issued as a third-party option and consumption of same should be recorded as ‘Misc. Consumption’ in Ni-kshay Aushadhi.
- The drugs are to be supplied to the private sector not more than twice a month.
Significance of stocking drugs in the private sector
- >40% of the patients in India attend private healthcare facilities initially for TB care and nearly 50% of the retreatment cases notified under NTEP are treated in the private sector before reaching NTEP. This data suggests inadequate TB treatment and could potentially develop drug resistance.
- Additionally, gaps in TB care cascade and subsequent delays in treatment initiation have also been associated with private providers.
- With the implementation of Universal Health Coverage (UHC), India has been working relentlessly to ensure that everyone receives healthcare services with minimum out-of-pocket expenditure.
- With the same motive, the NTEP recommends that all TB patients who seek care in the private sector in India also come under the ambit of the programme and should have access to the same quality of diagnostics, drugs and community-based services as public-sector patients.
- In a vast country like India, exploring partnerships with private sector service providers can strengthen supply chain management and ensure last-mile delivery of drugs.
- Therefore, provision for availing correct TB treatment from the private sector should be a fundamental right of every TB patient and is an important consideration with respect to reducing the incidence of drug-resistant TB in India as well as bettering the TB treatment outcome. Hence, it is also essential to stock NTEP drugs in the private sector.
Resources
- Guidelines on Programmatic Management of Drug-resistant TB (PMDT) in India; CTD, MoHFW, India, 2021.
- Procurement, Supply Chain Management & Preventive Maintenance, Module 6; CTD, MoHFW, India.
- From Where are Tuberculosis Patients Accessing Treatment in India? Results from a Cross-sectional Community-based Survey of 30 Districts;PLoS One, 2011.
- The Number of Privately-treated Tuberculosis Cases in India: An Estimation from Drug Sales Data. Lancet Infectious Disease, 2016.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following options is incorrect with respect to stocking NTEP drugs in the private sector?
Reduces the gaps in TB care
Reduces treatment outcome
Reduces expenditure for patients
Ensures last mile delivery of anti-TB drugs.
2
Stocking NTEP drugs in the private sector could help reduce the gaps in the TB care cascade, may contribute to better treatment outcomes, helps reduce patient expenditure, and ensures last-mile delivery of anti-TB drugs.
Yes
Yes
Process of stocking drugs in Private Sector
ContentThe private sector is the first point of care for nearly 50% of the patients with Tuberculosis (TB) and even then, the gaps in the TB care cascade and inadequate treatment are reported more in the private sector. The National Strategic Plan (NSP) 2017- 2025 has identified private sector engagement under the National TB Elimination Programme (NTEP) as a key priority in delivering quality ‘Standards for TB Care in India’ (STCI) services to the entire population. NTEP has implemented a policy of free drugs to all TB patients seeking treatment from public/private sectors.
Process of Stocking NTEP Drugs in the Private Sector
NTEP has utilized the partnership option of Patient-Provider Support Agencies (PPSA), where the private sector providers are contracted under the programme for effectively managing TB in the private sector.
The PPSA personnel are responsible for facilitating the process of stocking TB drugs in private sector.
Identifying the patient:
- Once the patients are diagnosed of TB at the private health facilities (HF), they must be notified to the NTEP and registered through Nikshay on a real time basis.
- Following registration, a drug dispensation module is created for each private notified patient on Nikshay by the PPSA user, where in all the details of the drug to be issued to the patient should be added.
Evaluating patient load:
- The drugs are issued to the private sector stocking points based on the number of patients notified and started treatment in the private health facilities, as reported on Nikshay each month as well as the expected number of patients forecasted.
- PPSA is responsible for ensuring real time notification as well as forecasting and regular supply of drugs to private health establishments and logistics management in co-ordination with NTEP.
Location
- PPSA will facilitate identification of health facilities (HF) and chemists for Fixed Drug Combinations (FDC) management and dispensing activities who will then enter into a Letter of Arrangement (LOA) with district NTEP for FDC management and dispensing activities if medicines are stored there.
- 1-2 Chemist shop in each ward (need-based) where FDC could be dispensed should be identified , to ensure patients find it easier to collect medicines nearer to their house.
- Alternately, the sputum collection point for private notified patients i.e., a Urban Primary Health Centre(UPHC) can be used to dispense FDCs to private TB patients.
Treatment regimen an drug requirement
- Currently NTEP’s FDC for Drug Sensitive (DS) TB treatment are available at the private sector facilities free of cost to the patients.
- Once DS TB diagnosis is established, the HF themselves may be encouraged to provide 1 strip of FDC or 3 days loose medicines (as applicable) to the patient.
- For Drug Resistant (DR) TB, initiation of treatment for DR TB will preferably be at the District DR TB sites or NTEP engaged private sector DR-TB site with NTEP DR TB medicines and the PPSA will facilitate the entire process.
Stock availability and expiry management
- PPSA will manage the FDC logistics from the respective Urban TU to the HF / empanelled chemists through Nikshay application which is integrated with the Nikshay Aushadhi through backend APIs (Application Programming Interface) and physical stock register.
- Average of two months stocks with the chemists with monthly replenishment is desired.
- PPSA should ensure that there is no expiry of FDC’s at the chemist. Coordinate with NTEP for forecasting and regular supply of drugs to private health establishments and logistics management.
- PPSA should ensure sleeving the FDC strips with the appropriate 99 DOTS sleeves before delivering to the chemists.
- Prescriptions containing NTEP FDC drugs will have to be honoured by the empanelled Chemists and all private sector consumption points must compulsorily fill the schedule H1 to prevent any indiscriminate use of anti TB drugs.
Resources
- National Strategic Plan for Tuberculosis Elimination 2017–2025, CTD, MoHFW, India.
- Procurement, Supply Chain Management & Preventive Maintenance, Module 6, CTD, MoHFW, India.
- The Number of Privately-treated Tuberculosis Cases in India: An Estimation from Drug Sales Data, Lancet Infectious Diseases, 2016, pii: S1473-309930259-6.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Fill in the blank
The credit/ debit of stock in the private sector is facilitated through ……
Private Provider
Treatment Supporter
Patient
Nikshay
4
The credit/ debit of stock in the private sector is facilitated through Nikshay
Yes
Yes
Monitoring and expiry management of drugs in Private sector
ContentMonitoring the supply chain of anti TB drugs and appropriate management of drug expiry is important:
- to ensure an uninterrupted supply
- to avoid delays in treatment initiation
- to prevent drug stock imbalances.
Monitoring and Expiry Management of National TB Elimination Porgramme (NTEP) Drugs in the Private Sector
1) Personnel
- The monitoring and expiry management of NTEP drug stocks in the private sector is managed by the Patient Provider Support Agency (PPSA) contracted under the NTEP.
- The PPSA identifies the stocking points for the private sector based on their TB notification rate as well as the patient reach.
- The PPSA will be responsible to ensure that sufficient stock is available at the private sector stocking unit and also to manage the transport of the drugs from the district to the empanelled chemists and other providers.
2) Assessment of stock requirement
- The supply of drugs to private sector stocking points should only be undertaken based on the number of regimen-wise new patients initiated on treatment as notified on Nikshay and calculated number of future patients for a particular period.
- Therefore, for smooth monitoring of private drug stocks, they must ensure that all the diagnosed TB patients in the private sector are notified on Nikshay.
- The dispensation of drugs to private sector patients is fulfilled through Ni-kshay which is integrated with Ni-kshay Aushadhi via backend APIs (Application Programming Interface).
3) Stock availability and expiry management
- Fixed Drug Combinations (FDCs) for DS TB treatment are stocked at the private sector health facilities and PPSA personnel should ensure the same.
- Drug inventory records such as the FDC prescriptions/voucher invoice from the private sector stocking points should be reviewed by the PPSA personnel and also cross-checked with Nikshay records.
- The drugs are to be supplied to the private sector stocking points for not more than twice a month.
- The private sector chemist also needs to maintain a separate Schedule H1 register that includes the patient's identity, prescribing doctor's contact information, drug name and dispensed quantity, and date.
- In any case of drugs being returned or drugs that are expiring, the same should be updated on Nikshay using the return dispensation module and should be transferred back to the parent store via the PPSA.
- In no case, more than 60 days of FDC should be issued to a single patient at once.
Resources
- Guidance Document on Partnerships, CTD, MoHFW, India, 2019.
- Guidelines for Programmatic Management of Drug-resistant TB (PMDT) in India, NTEP, CTD, MoHFW, India, 2021.
- Procurement, Supply Chain Management & Preventive Maintenance, Module 6, CTD, MoHFW, India.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
How many times a month can the drugs be supplied to the private sector stocking points?
Only once
Maximum twice
Maximum three times
Maximum four times
2
The drugs are to be supplied to the stocking points for not more than twice a month.
Yes
Yes
-
PHI Pharmacist : EXPIRY MANAGEMENT
FullscreenOverview of Expiry management of supplies
ContentMeaning and Purpose of Expiry Management
To ensure timely consumption of supplies, the Pharmacist/storekeeper is expected to keep a track of the expiry dates of the drugs and other commodities held in stores. Expiry date reflects the period after which a drug or any other product is known to lose its strength, quality and purity and the time-period ranging from the manufacturing date to the expiry date is referred to as the Shelf-life. The processes involved in ensuring that the supplies are utilized within their shelf life without any wastage is known as the “Expiry Management”.
Supplies that get expired:
Under NTEP following supplies come with an expiry date and must be utilized within their shelf life
S.No.
Supply
Expiry date/shelf-life
1
Anti-TB drugs
2-5 years from the date of manufacturing
2
Xpert MTB/RIF Cartridges
2 years from the date of manufacturing
3
TrueNat MTB chips
2 years from the date of manufacturing
4
TrueNat MTB-RIF Chips
2 years from the date of manufacturing
Resources
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What does expiry management ensure?
Timely utilisation of drugs before losing its efficacy.
Reduction in wastage of drugs and lab consumables.
Redirecting drugs to different treatment centres for utilisation before expiry.
All of the above
4
Yes
Yes
Forecasting the expiry of supplies
ContentForecasting the expiry of supplies
In order to ensure the timely consumption of supplies it is important to develop mechanism to periodically monitor control over expiry position of the supplies held in stocks. Reviewing of reports generated by Nikshay Aushadhi can help forecasting the expiry of drugs and taking appropriate actions to ensure consumption of these supplies before their expiry dates. Some of these reports are listed below:
Drug expiry alert: This alert lists out all the drugs from the inventory of the store that are going to expire in the next three months.

Figure 1: Drug expiry alert
Source: Nikshay Aushadhi portal
Stock ledger report and Stock in hand reports: These reports give a list of drugs available at a particular store and details about their available stock and consumption status. These reports will highlight the stores that are overstocked based on their consumption pattern and might not be able to utilize the supplies within their expiry dates.

Figure 2: Stock in hand record
Source: Nikshay Aushadhi portal

Figure 3: Stock ledger report
Source: Nikshay Aushadhi portal
Once the stores having drugs with near expiry dates or those who are overstocked are identified the next step would be to calculate the consumption capacity of these stores based on their existing patient load and anticipated number of new patients to be added. This would help in forecasting drugs in stock that would be consumed before their expiry and those that will not.
Following format can be used for forecasting the consumption of the supplies before expiry:
Table 1: Format for forecasting consumption of supplies
Store
Drug
Expiry Date
Stock in Hand
Anticipated consumption by existing patients
Expected consumption by new patients
Total expected consumption
Excess quantity
Will the consumption happen within the expiry date? Yes/NO
Resources
Standard Operating Procedure Manual Procurement & Supply Chain Management, Ministry of Health and Family Welfare, Government of India 2018
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Drug expiry alert lists out drugs which have their expiry date in next:
6 months
3 months
1 month
15 days
2
Drug expiry alert lists out all the drugs from the inventory of the store that are going to expire in the next three months.
Follow-up actions to forecasting of expiry of supplies
ContentFollow-up actions to forecasting of expiry of supplies
Once the pharmacist has forecasted the supplies that may not be consumed within their expiry date, different scenarios may arise in order to manage these supplies efficiently. The scenarios are listed below:
Scenario 1: Supplies will not be consumed at a particular district but may be consumed in other districts of the same state
In this situation, the pharmacist should communicate the details of these supplies to the parent store and State TB Officer (STO). The STO upon receipt of the information will take following actions:
Issue to Sub-stores
After conducting requirement and utilization assessment of each district, STO will identify the needy district where the supplies can be transferred. Drug Transfer Advice (DTA) will be sent to both the stores by the STO.
Note: At least 5 months shelf life should remain before the drugs are diverted from one district to another district.
Other options
The STO can also explore the option of transferring such supplies to facilities outside of NTEP that can utilize these supplies. These facilities may include hospitals, dispensaries, or other facilities within the general health system.
Scenario 2: Supplies may not be consumed by any facility within the state
In this situation information about these supplies should be sent to the Central TB division and the STO with a request to divert these drugs to places where they can be utilized. CTD upon receipt of the information will take following actions:
Transfer to other states
On receipt of requests for diversion, CTD shall identify the States which can utilize these supplies within the given shelf-life. Drug Transfer Advice (DTA) will be sent by CTD to both the States for diversion of drugs.
Resources
Standard Operating Procedure Manual Procurement & Supply Chain Management, Ministry of Health and Family Welfare, Government of India 2018
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Minimum shelf-life of the drugs before inter district diversion should be
2 years
3 months
1 year
5 months
4
At least 5 months shelf life should remain before the drugs are diverted from one district to another district.
Disposal of expired supplies
ContentExpiry management of supplies is crucial to avoid financial losses and harm to patients.
If any drug expires due to reasons beyond control, the write-off of expired drugs should be as per the guidelines given in NTEP National Strategic Plan. As per NSP, the State is allowed to write off up to 2% of the cost of the annual supply of drugs on implementation of Drug Sensitivity Testing (DST) guided treatment and 2% cost of rapid molecular test cartridges. The expired stock should be disposed-off as per the Bio-medical Waste (Management and Handling) guidelines of Govt. of India.
Disposal of Expired/Discarded Medicines
Colour of the bag to be used: Yellow
Image
Figure 1: Disposal of expired supplies according to Bio-Medical Waste Management Rules 2016
Updating in Ni-kshay Aushadhi
To dispose of or remove the expired/rejected drugs from the online inventory, follow the steps below:
- Go to the ‘Write-Off/Disposal’ process in Stock Management,
- Click on the ‘Request’ button to generate the disposal request,
- Select the ‘Expired or Rejected’ category, and the system will show the respective drugs
- Select the drug with an expired batch and enter the quantity
- Click on the ‘Save’ button.

Figure 2: Write-off/disposal register in Nikshay Aushadhi Source: Nikshay Aushadhi portal

Figure 3: Entering details of expired drugs in the write-off/disposal register in Nikshay Aushadhi Source: Nikshay Aushadhi portal
Steps to follow
- After saving, select the request and click on the ‘Write-off’ button,
- Verify the drug details and select the type of write-off as ‘Burned/Buried’,
- Enter the ‘Remarks’, and click on the ‘Save’ button,
- System will generate the voucher, and the drug quantity will be deducted from the inventory.

Figure 3: Expired drug details in Nikshay Aushadhi Source: Nikshay Aushadhi portal
Condemnation of laboratory supplies

Figure 4: Process of condemnation of laboratory supplies which are non-functional, obsolete, non-reparable equipment in NTEP’s laboratories
Information is required in below mentioned format to condemn the lab equipment:

Figure 5: Form GFR 10 Source: General Financial Rules 2017, Ministry of Finance, Department of Expenditure, GoI
The request for the replacement of the equipment condemned has to be submitted to State TB Officer (STO)/Central TB Division (CTD) in the below-mentioned format:

Figure 6: Annexure 4 for details of equipment for condemnation Source: Guidelines for the condemnation and replacement of Tuberculosis (TB) laboratory equipment under the Revised National Tuberculosis Control Programme (RNTCP) 2019
Resources
1. Guidelines for Management of Healthcare Waste as per Biomedical Waste Management Rules, 2016
Assessment:
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Disposal of expired supplies is done in which colour bag? Yellow Red White Blue 1 Discarded or expired medicine in yellow coloured non-chlorinated plastic bags
-
-
M-5: PHI Pharmacist: Logistics and Distribution of Drugs and consumables
Fullscreen-
PHI Pharmacist : PACKAGING
FullscreenPackaging - Significance
ContentPackaging involves the process of packing loose second-line anti-TB drugs into one-monthly Patient-wise Boxes (PWBs) also known as the standardised drug boxes for shorter, longer Multidrug/ Rifampicin-resistant TB (MDR/RR-TB) and for H-mono/ poly Drug-resistant TB (DR-TB) regimen.
- The drug box preparation is preferably done at the State Drug Store (SDS) level. However, in states that have built the capacity of districts, the exercise of preparation of standard PWBs may also be conducted at District Drug Stores (DDS) under the guidance and supervision of the District TB Officer (DTO).
- The DDS is supplied monthly PWBs as per the standard regimens as well as loose medicines for replacement.
- Under certain circumstances, the drug box may also be prepared at the district level, like unpacking of unused/ partially used boxes and modification of regimen as per replacement advised by the DR-TB centre.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, NTEP, Central TB Division, Ministry of Health and Family Welfare, Government of India, 2021.
- Standard Operating Procedure Manual Procurement & Supply Chain Management, Central TB Division, Ministry of Health and Family Welfare, Government of India.
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which DR-TB regimen has only one standard PWB prepared for the entire duration of treatment?
Shorter oral Bdq-containing regimen
Longer oral M/XDR regimen
H - mono/ poly DR-TB regimen
None of the above
3
In comparison to other DR-TB regimens, a full treatment course should be prepared for the entire duration of 6 months.
Yes
Yes
Specification of boxes
ContentIn the National Tuberculosis Elimination Programme (NTEP), packaging of loose drugs into Type A, B & C boxes are done at the State Drug Stores (SDSs) under the guidance of the State TB Officer (STO)/ Medical Officer (MO)/ Drug logistics in-charge.
Specifications for packaging of patient-wise monthly drug box
Common for both Type A and Type B boxes
- Material: Punching ring flap model (1 side pin) 3 ply corrugated, top paper 230 gsm, ply 150 gsm and the inner wall of 180 gsm.
- Opening: From the top with the attached lid.
- Packing: Box should be stapled with heavy pins.
- Colour: Outer white and inner brown
Type A Box
- Size: 10.5” x 7.5” x 3.25” (inch)
- Partitions in the box: 3 ply white to white vertical and 12 horizontal, fitting in to vertical serially
- Size of partition: Horizontal: 7.5” x 2.75” – Vertical 10” x 2.75”
- In each Type A box, one pouch of silica gel desiccant of 4 gm weight should be kept.
- One monthly pouch of capsule Cycloserine and tablet Ethambutol each should be made from a plastic bag with a zip lock facility in which a 1 gm pouch of silica gel desiccant should be kept.
Type B box
- Size: 11” x 4” x 4” (inch)

Figure 1: Type A Box; Source: Guidelines on Programmatic Management of Drug-resistant TB (PMDT) in India; CTD, MoHFW, India, 2017.

Figure 2: Type B Box; Source: Guidelines on Programmatic Management of Drug-resistant TB (PMDT) in India; CTD, MoHFW, India, 2017.
Specifications for Labelling of Patient-wise Monthly Drug Box
- Once the patient-wise monthly drug box is prepared, labels for these drug boxes should also be prepared to contain all details about the drugs within the box and printed directly from the Ni-kshay Aushadhi system.
- Labels should be generated for each cycle of box preparation and contain expiry-wise drug content of the boxes and should be pasted over the boxes prepared during that cycle only.
- The label should be marked with a bold marker pen and pasted on the visible side of the carton.
- Labelling the drug boxes helps in facilitating the storekeeper to follow the First Expiry First Out (FEFO) principle, avoids excessive stocking of shortage drugs/ drug stock imbalances, enables issue of the regimen-wise box systematically and the barcode present on the label helps to ensure better inventory, tracking and supply chain management.
Resources
- Guidelines on Programmatic Management of Drug-resistant TB (PMDT) in India; CTD, MoHFW, India, 2017.
- Standard Operating Procedure Manual Procurement & Supply Chain Management; CTD, MoHFW,India,2018.
- Procurement, Supply Chain Management & Preventive Maintenance, Module 6; CTD, MoHFW, India.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What is the colour of the box used for packaging patient-wise monthly drugs?
Outer brown and inner white
Outer white and inner brown
Outer blue and inner white
Outer white and inner blue
2
The colour of the box used in the packaging of the monthly patient-wise box is outer white and inner brown.
Yes
Yes
Labelling the boxes
ContentImportance of Labelling the Drug Boxes
- It helps to identify regimen-wise boxes quickly
- It helps the storekeeper in practising the First Expiry First Out (FEFO) principle
- Ensures better inventory management
- Strengthens the tracking and supply chain through the bar code present on the label
Contents of the label

All Oral Longer Regimen for MDR/RR FQ Res or XDR TB
All Oral Longer Regimen for MDR/RR FQ Res or XDR TB Type A (30-45) [OLR A2]
S.No.
Drug Name
UOM
Strength(No.)
Batch No.
DOE
No. Of Unit
Dosage Per Day
1
Clofazimine 100mg [PC40]
Cap
100 MG
NCG2009A
Feb/2022
30
1.00
2
Cycloserine 250mg [PC24]
Cap
250 MG
ECE2023A
Dec/2021
60
2.00
3
Linezolid 600mg [PC38]
Tab
600 MG
BLN2001A
Dec/2022
30
1.00
4
Moxifloxacin 400mg [PC39]
Tab
400 MG
EMC62004A
Feb/2023
60
2.00
5
Pyridoxine 100mg [PC26]
Tab
100 MG
EPD92001A
Jan/2023
30
1.00
Lot No. : 2160010822
Total : 210
Date Of Expiry Of Box : Dec/2021
Figure 1: Drug Box label; Source: Packaging and Repackaging,Nikshay Aushadhi User Manual; CTD, MoHFW, India.
Method of Labelling the Drug Boxes

Figure 2:Label pasted on the drug box
- The labels should be pasted on the visible side of the carton.
- The label should be in bold colours for quick identification.
- There should be different coloured labels for different regimens as well as for the intensive and continuation phases.
- The label should be pasted in an oblong manner on the box to allow quick readability.
- The label should be generated through the Ni-kshay Aushadhi during each cycle of box preparation and printed directly from the system.
- The labels prepared for a particular cycle should be pasted over the boxes prepared during that cycle only.
Resources
- Standard Operating Procedure Manual Procurement & Supply Chain Management; CTD, MoHFW,India,2018.
- Procurement, Supply Chain Management & Preventive Maintenance, Module 6; CTD, MoHFW, India.
- Packaging and Repackaging,Nikshay Aushadhi User Manual; CTD, MoHFW, India.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
The labels prepared for a particular cycle may be pasted over the boxes prepared for any other cycle. True
False
2 The labels prepared for a particular cycle should be pasted over the boxes prepared during that cycle only. Yes
Yes
Types of monthly PWB
ContentThere are two types of monthly Patient Wise Boxes (PWB) issued to the TB patients.
1) Type A: Contains oral drugs that are used for treatment during both the Intensive Phase (IP) and Continuation Phase (CP).
2) Type B: Contains injectables which are prescribed for Intensive Phase (IP) only
Based on the regimen and weight band of the patients , PWB are prepared and issued to the patients.
Contents of PWB
- PWB for Shorter Oral Bedaquiline-containing MDR/RR-TB Regimen: Constitutes both Type A and Type B box
Type A box
Use in Intensive Phase (IP) as well as Continuation Phase (CP)
Drugs
Strength
16-29 kg
30-45 kg
46-70 kg
>70 kg
Tab. Levofloxacin*
250/ 500 mg
250 mg *30 tab
250 mg *30 tab + 500 mg *30 tab
500 mg *60 tab
500 mg *60 tab
Tab. Clofazimine
50/ 100 mg
50 mg *30 tab
100 mg *30 tab
100 mg *20 tab
100 mg *60 tab
Tab. Ethambutol
400/ 800 mg
400 mg *30 tab
800 mg *30 tab
400 mg *30 tab + 800 mg *30 tab
600 mg *60 tab
Tab. Pyrazinamide
500/ 750 mg
750 mg *30 tab
500 mg *30 tab + 750 mg *30 tab
500 mg *60 tab + 750 mg *30 tab
500 mg *30 tab + 750 mg *60 tab
Tab. Pyridoxine
50/100 mg
50 mg *30 tab
100 mg *30 tab
100 mg *30 tab
100 mg *30 tab
* When moxifloxacin is prescribed under exceptional conditions instead of levofloxacin, the modified box with moxifloxacin (normal dose) can be prepared from the standard box at DDS.
Type B box
Use in IP
Drugs
Strength
16-29 kg
30-45 kg
46-70 kg
>70 kg
Tab. Isoniazid
100/ 300 mg
300 mg *30 tab
300 mg *60 tab
300 mg *90 tab
300 mg *90 tab
Tab. Ethionamide
125/ 250 mg
125 mg *30 tab + 250 mg *30 tab
250 mg *60 tab
250 mg *90 tab
250 mg *120 tab
Bedaquiline bottle
100 mg
Jar of 188 tablets for full course
- PWB for Shorter Injectable-containing Regimen: Constitutes both Type A and Type B box
Type A box
Use in Intensive Phase (IP) as well as Continuation Phase (CP)
Drugs
Strength
16-29 kg
30-45 kg
46-70 kg
>70 kg
Tab. Moxifloxacin-High Dose
400 / 800 mg
400 mg *30 tab
400 mg *30 tab
400 mg *60 tab
400 mg *60 tab
Tab. Clofazimine
50/ 100 mg
50 mg *30 tab
100 mg *30 tab
100 mg *20 tab
100 mg *60 tab
Tab. Ethambutol
400/ 800 mg
400 mg *30 tab
800 mg *30 tab
400 mg *30 tab + 800 mg *30 tab
600 mg *60 tab
Tab. Pyrazinamide
500/ 750 mg
750 mg *30 tab
500 mg *30 tab + 750 mg *30 tab
500 mg *60 tab + 750 mg *30 tab
500 mg *30 tab + 750 mg *60 tab
Tab. Pyridoxine
50/100 mg
50 mg *30 tab
100 mg *30 tab
100 mg *30 tab
100 mg *30 tab
Type B box
Use in IP
Drugs
Strength
16-29 kg
30-45 kg
46-70 kg
>70 kg
Inj. Kanamycin
15mg/kg/day
500 mg *24 inj.
750 mg * 24 inj.
750 mg *24 inj.
1000 mg *24 inj.
Tab. Isoniazid-high dose
100/ 300 mg
300 mg *30 tab
300 mg *60 tab
300 mg *90 tab
300 mg *90 tab
Tab. Ethionamide
125/ 250 mg
125 mg *30 tab + 250 mg *30 tab
250 mg *60 tab
250 mg *90 tab
250 mg *120 tab
- PWB for Longer Oral M/XDR-TB Regimen : Constitutes only Type A box as there is no separate IP/CP under this regimen
Standard PWB
Continue till Complete Treatment
Drugs
Strength
16-29 kg
30-45 kg
46-70 kg
>70 kg
Tab. Levofloxacin
250 / 500 mg
250 mg *30 tab
500 mg *30 tab + 250 mg *30 tab
500 mg *60 tab
500 mg *60 tab
Tab. Linezolid#
600 mg
600 mg *30 tab#
600 mg *30 tab
600 mg *30 tab
600 mg *30 tab
Tab. Clofazimine
50/ 100 mg
50 mg *30 tab
100 mg *30 tab
100 mg *30 tab
100 mg *30 tab
Tab. Cycloserine
250 mg
250 mg *30 tab
250 mg *60 tab
250 mg *90 tab
250 mg *120 tab
Tab. Pyridoxine
50/100 mg
50 mg *30 tab
50 mg *30 tab
50 mg *30 tab
50 mg *30 tab
Bedaquiline bottle
100 mg
1 Jar (Jar of 188 tablets for full course)
# Tab. Linezolid available in 600 mg only. When prescribed with modified dose of 300 mg Once Daily (OD), patient should be advised to divide the pill in half.
- PWB for H-mono/poly DR-TB Regimen: Constitutes only Type A box as there is no separate IP/CP under this regimen
Standard PWB
Continue till complete treatment
Drugs
Strength
16-29 kg
30-45 kg
46-70 kg
>70 kg
Tab. Levofloxacin
250/ 500 mg
250 mg *180 tab
250 mg *180 tab + 500 mg *180 tab
500 mg *360 tab
500 mg *360 tab
Tab. Rifampicin
150/ 300/ 450 mg
300 mg *180 tab
450 mg *180 tab
300 mg *360 tab
300 mg *360 tab + 150 mg *180 tab
Tab. Ethambutol
400/ 800 mg
400 mg *180 tab
800 mg *180 tab
400 mg *180 tab + 800 mg *180 tab
800 mg * 360 tab
Tab. Pyrazinamide
500/ 750 mg
50 mg *180 tab
7750 mg *180 tab + 500 mg *180 tab
750 mg *180 tab + 500 mg *360 tab
750 mg *360 tab + 500 mg *180 tab
Tab. Pyridoxine
50/100 mg
50 mg *180 tab
100 mg *180 tab
100 mg *180 tab
100 mg*180 tab
In comparison to other DR-TB regimens, a full treatment course should be prepared for the entire duration of 6 months.
Resources
- Standard Operating Procedure Manual Procurement & Supply Chain Management, CTD, MoHFW,India,2018
- Procurement, Supply Chain Management & Preventive Maintenance, Module 6, CTD, MoHFW, India.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which type of drug box is issued to the patient on all oral H-mono/ poly regimen?
Type A
Type B
Type A & Type B
Type C
1
A patient initiated on all oral H-mono/poly DR-TB regimen will receive the monthly type A box.
Yes
Yes
-
PHI Pharmacist : PATIENT-WISE BOXES
FullscreenConstituents of Monthly Patient-wise Boxes [PWB] for Shorter Oral Bedaquiline-containing MDR/RR-TB Regimen
ContentThe patient on shorter oral Bedaquiline-containing multi-drug resistant (MDR)/rifampicin resistant TB (RR-TB) regimen shall be put on Type A and Type B box when initiated on treatment on a monthly patient wise box (PWB). Bedaquiline (Bdq) needs to be issued separately and stopped after 6 months. The patient should be provided with only Type A boxes when started on continuation phase (CP).
Table 1: Constituents of monthly-type A and B PWB of shorter oral Bedaquiline-containing MDR/RR-TB regimen; Source : Guidelines for PMDT, India 2021, p.132-133 TYPE A BOX
(USE IN IP AS WELL AS CP)
Drugs
Strength
16-29 kg
30-45 kg
46-70 kg
>70 kg
Tab. Levofloxacin#
250/500 mg
250 mg *30tab
250 mg *30tab + 500 mg *30tab
500 mg *60tab
500 mg *60tab
Tab. Clofazimine
50/100 mg
50 mg *30tab
100 mg *30tab
100mg *30tab
100 mg *60tab
Tab. Ethambutol
400/800 mg
400 mg *30tab
800 mg *30tab
400 mg *30tab + 800 mg *30tab
800 mg *60tab
Tab. Pyrazinamide
500/750 mg
750 mg *30tab
500 mg *30tab + 750 mg *30tab
500 mg *60tab + 750 mg *30tab
500 mg *30tab + 750 mg *60tab
Tab. Pyridoxine
50/100 mg
50 mg*30tab
100 mg*30tab
100 mg*30tab
100 mg*30tab
Type B Box
(Use in IP)
Drugs
Strength
16-29 kg
30-45 kg
46-70 kg
>70 kg
Tab. Isoniazid
100/300 mg
300 mg *30tab
300 mg *60tab
300 mg *90tab
300 mg *90tab
Tab. Ethionamide
125/250 mg
125 mg *30tab + 250 mg *30tab
250 mg *60tab
250 mg *90tab
250 mg *120tab
Bedaquiline bottle
100 mg
1 Jar (Jar of 188 tablets for full course)
# When moxifloxacin prescribed under exceptional condition instead of levofloxacin, the modified box with moxifloxacin (normal dose) can be prepared from standard box at district drug store (DDS)
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
-
Pharmacist: Longer Oral M/XDR-TB Regimen
FullscreenLonger Oral M/XDR-TB: Regimen and Duration
ContentLonger oral Multi (M)/ Extensive Drug-resistant (XDR) -TB treatment is specified with a definite regime and duration.
Regimen: (18-20) Levofloxacin (Lfx), Bedaquiline (Bdq) (6 months or longer), Linezolid# (Lzd), Clofazimine (Cfz), Cycloserine (Cs) (# dose of Lzd will be tapered to 300 mg after the initial 6–8 months of treatment)
- Duration: 18-20 months
- No separate Intensive Phase (IP) and Continuation Phase (CP).
- Bdq will be given for 6 months and extended beyond 6 months as an exception.
- Pyridoxine should be given to all Drug-resistant TB (DR-TB) patients as per the weight bands.
- For Extensively Drug-resistant TB (XDR-TB) patients, the duration of a longer oral XDR-TB regimen would be for 20 months.
Resources
- Guidelines for Programmatic Management of Drug-Resistant Tuberculosis in India, March 2021.
- WHO Consolidated Guidelines on Tuberculosis: Module 4 – Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Treatment Extension in Longer Oral M/XDR-TB Regimen
ContentThe total duration of a longer oral Multidrug/ Extensively drug-resistant TB (M/XDR-TB) regimen is 18–20 months.
ImageFigure: Protocol for Treatment Extension in Longer Oral M/XDR-TB Treatment Regimen
Extension of Bedaquiline (Bdq) beyond 6 months is to be considered in patients in whom an effective regimen cannot otherwise be designed.
- If any additional resistance to Group A, B or C drugs in use is detected, the patient needs to be reassessed at the Nodal/ District Drug-resistant Tuberculosis Centre (N/DDR-TBC) for modification of a longer oral M/XDR-TB regimen immediately on receiving the report.
- A treatment duration of 15–17 months after culture conversion is suggested for most patients. The duration may be modified according to the patient’s response to treatment.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- WHO Consolidated Guidelines on Tuberculosis: Module 4 – Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Adverse Drug Reactions due to Longer oral M/XDR-TB Regimen
ContentThe table below showcases the adverse drug events that may be caused by drugs used for longer oral Multi (M)/ Extensively Drug-resistant TB (XDR-TB) regimen. In these situations, replacement drugs are used instead of these drugs.
Table: Possible Adverse Drug Events in the Longer Oral M/XDR-TB Regimen
ADVERSE DRUG EVENTS
DRUGS
QT prolongation
Bedaquiline (Bdq), Fluoroquinolone (FQ), Clofazimine (Cfz) Rash, allergic reaction and anaphylaxis Any drug
Gastrointestinal symptoms
Ethionamide (Eto), P-Aminosalicylic Acid (PAS), Pyrazinamide (Z), Ethambutol (E), Bdq, Cfz, Linezolid (Lzd), FQs Diarrhoea and/or flatulence
PAS, Eto
Hepatitis
Z, Eto, PAS, Bdq
Giddiness
Amikacin (Am), Eto, FQ and/or Z
Haematological abnormalities
Lzd
Hypothyroidism
Eto, PAS
Arthralgia
Z, FQ, Bdq
Peripheral neuropathy
Lzd, Cycloserine (Cs), Am, FQ, rarely Eto, E
Headache
Bdq, Cs
Depression
Cs, FQ, Eto
Psychotic symptoms
Cs, Isoniazid (H), FQ
Suicidal ideation
Cs, Eto
Seizures
Cs, H, FQ
Tendonitis and tendon rupture
FQ
Nephrotoxicity (renal toxicity)
Am
Vestibular toxicity (tinnitus and dizziness
Am, Cs, FQs, Eto, Lzd
Hearing loss
Am Optic neuritis
E, Lzd, Eto, Cfz
Metallic taste
Eto, FQs
Electrolyte disturbances (Hypokalaemia and Hypomagnesaemia
Am
Gynaecomastia
Eto
Alopecia
Eto
Superficial fungal infection and thrush
FQ
Lactic acidosis
Lzd
Dysglycaemia and Hyperglycaemia
Eto
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- WHO Consolidated Guidelines on Tuberculosis: Module 4 - Treatment: Drug Resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Dosages of M/XDR-TB Drugs for Adult in Longer Oral M/XDR-TB Regimen
ContentIt is important to know the dosages of Multi (M)/ Extensively Drug-resistant TB (XDR-TB) drugs for adults on a longer oral M/XDR-TB regimen.
The table below shows the M/XDR-TB regimen drugs for adults weight band-wise, used in longer oral M/XDR-TB regimen customized for India by national experts.
Table: Dosages of M/XDR-TB Drugs for Adults in Longer Oral M/XDR-TB Regimen Sr.No
Drugs
16-29 kg
30-45 kg
46-70 kg
>70 kg
1
Levofloxacin (Lfx)
250 mg
750 mg
1000 mg
1000 mg
2
Moxifloxacin (Mfx)
200 mg
400 mg
400 mg
400 mg
3
High dose Mfx (Mfxh)
400 mg
600 mg
600 mg
600 mg
4
Bedaquiline (Bdq)
Week 0–2: Bdq 400 mg daily
Week 3–24: Bdq 200 mg 3 times per week
5
Clofazimine (Cfz)
50 mg
100 mg
100 mg
200 mg
6
Cycloserine (Cs)3
250 mg
500 mg
750 mg
1000 mg
7
Linezolid (Lzd)
300 mg
600 mg
600 mg
600 mg
8
Delamanid (Dlm)
50 mg twice daily (100 mg) for 24 weeks in 6-11 years of age
100 mg twice daily (200 mg) for 24 weeks for ≥12 years of age
9
Amikacin (Am)1
500 mg
750 mg
750 mg
1000 mg
10
Pyrazinamide (Z)
750 mg
1250 mg
1750 mg
2000 mg
11
Ethionamide (Eto)3
375 mg
500 mg
750 mg
1000 mg
12
Na - PAS (60% weight/ vol)2,3
10 gm
14 gm
16 gm
22 gm
13
Ethambutol (E)
400 mg
800 mg
1200 mg
1600 mg
14
Imipenem-Cilastatin (Imp-Cln)3
2 vials (1g + 1g) bd (to be used with Clavulanic acid)
15
Meropenems (Mpm)3
1000 mg three times daily (alternative dosing is 2000 mg twice daily) (to be used with Clavulanic acid)
16
Amoxicillin-Clavulanate (Amx-Clv) (to be given with Carbapenems only)
875/125 mg bd
875/125 mg bd
875/125 mg bd
875/125 mg bd
17
Pyridoxine (Pdx)
50 mg
100 mg
100 mg
100 mg
1For adults more than 60 years of age, the dose of Second-line Injectable (SLI) should be reduced to 10 mg/kg (max up to 750 mg).
2In patients of Para Amino Salicylic Acid (PAS) with 80% weight/ volume the dose will be changed to 7.5 gm (16-29 kg); 10 gm (30-45 Kg); 12 gm (46-70 kg) and 16 gm (>70 kg).
3Drugs can be given in divided doses in a day in the event of intolerance.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- WHO Consolidated Guidelines on Tuberculosis: Module 4 – Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Constituents of Patient-wise Boxes [PWB] for Isoniazid [H] Mono/Poly DR-TB Regimen
ContentStandard Patient-wise Boxes (PWBs) are constituted for TB patients initiated on Isoniazid (H) Mono/ Poly Drug-resistant TB (DR-TB) regimen.
This regimen has no segregation in terms of Intensive Phase (IP) or Continuation Phase (CP), hence drugs are provided in a single type of PWB.
Table: Constituents of standard PWB (6 months) of H mono/ poly DR-TB regimen; Source: Guidelines for PMDT, India 2021, p134
STANDARD PWB
CONTINUE FOR COMPLETE TREATMENT Drugs
Strength
16-29 kg
30-45 kg
46-70 kg
>70 kg
Tab. Levofloxacin
250/ 500 mg
250 mg *180 tab
250 mg *180 tab + 500 mg *180 tab
500 mg *360 tab
500 mg *360 tab
Tab. Rifampicin
150/ 300/ 450 mg
300 mg *180 tab
450 mg *180 tab
300 mg *360 tab
300 mg *360 tab + 150 mg *180 tab
Tab. Ethambutol
400/ 800 mg
400 mg *180 tab
800 mg *180 tab
400 mg *180 tab + 800 mg *180 tab
800 mg *360 tab
Tab. Pyrazinamide
500/ 750 mg
750 mg *180 tab
750 mg *180 tab + 500 mg *180 tab
750 mg *180 tab + 500 mg *360 tab
750 mg *360 tab + 500 mg *180 tab
Tab. Pyridoxine
50/100 mg
50 mg *30 tab
100 mg *30 tab
100 mg *30 tab
100 mg *30 tab
*No separate box for IP and CP.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- Central TB Division, MoHFW. Training Modules (5-9) for Programme Managers & Medical Officers, 2020.
- Standard Operating Procedure Manual - Procurement & Supply Chain Management, RNTCP.
- Technical and Operational guidelines for TB in India, 2016.
Kindly provide your valuable feedback on the page to the link provided HERE
-
PHI Pharmacist : Return and Reconstitution
FullscreenOverview : Return and Reconstitution
ContentReturn
- Return is the process of returning the drug to the parent/ issuing store. This is generally followed whenever there are situations like lost to follow-up, transfer out, death, etc.
- Ni-kshay Aushadhi is being used to record and report the process.
- At present, the return of drugs from the patient/ treatment supporters is taking place in Ni-kshay (in Drug Dispensation Module)
- All the unconsumed drugs should be brought back by the treatment supporter to the Peripheral Health Institute (PHI)---->Tuberculosis Units (TU)---->District TB Centre (DTC) within the shortest possible time in order to ensure that they can be re-used in the future.
- Return of Bedaquiline (Bdq): Partially used Bdq bottle should be sent back to State Drug Stores (SDS) wherein it will be accounted for.
- Return of Delamanid (Dlm): Leftover Dlm tablets should be returned back to the District Drug Stores (DDS).
Reconstitution
- Reconstitution is defined as the process of re-packaging the returned anti-TB drugs in the event of loss to follow-up/ death/ discontinuation for any reason, back into a full treatment course for issuing to other patients.
- If the expiry of the remaining drugs is less than six months, the same may be issued at the Nodal Drug-resistant TB Centre (NDR-TBC) for patients while they are admitted and later adjusted from the long expiry bottle that is issued on discharge.
- The reconstitution exercise is carried out only for the Bedaquiline drug and is done at the SDS.
- First Expiry First Out (FEFO) principle should be strictly followed while issuing re-constituted drugs to the patients and also be cautious about the reconstituted drugs belonging to the different expiry batches.
- The reconstituted drugs should be accounted for and reported in Ni-kshay Aushadhi through the Box-preparation module under the Packaging/ Re-packaging service.
Resources
- Standard Operating Procedure Manual Procurement & Supply Chain Management, CTD, MoHFW, India, 2018.
- Return from Patient, Ni-kshay Aushadhi User Manual, CTD, MoHFW, India.
- Packaging and Repackaging, Ni-kshay Aushadhi User Manual, CTD, MoHFW, India.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Where is the reconstitution of Bdq drugs carried out?
District Drug Store
State Drug Store
Tuberculosis Unit
Peripheral Health Institute
2
The reconstitution of Bdq drugs should be carried out only at the State Drug Store.
Yes
Yes
Process of Return of Drugs
ContentUnder the National TB Elimination Programme (NTEP), the return process is facilitated through the Ni-kshay Aushadhi.
Return from the sub store to the parent store
- This is used to return drugs from the sub-store to the parent store, like from the Peripheral Health Institute (PHI) drug store to the Tuberculosis Unit (TU) drug store.
Steps in Ni-kshay Aushadhi for returning from the sub store to the patient store

Flowchart 2: Process of return from the sub store to the parent store on Ni-kshay Aushadhi

Figure 2: 5 - Return Request Desk, 6 - Returning Drugs Entry, 7 - Return Voucher; Source: Return from Patient, Nikshay Aushadhi User Manual, CTD, MoHFW, India.
Resources
- Standard Operating Procedure Manual Procurement & Supply Chain Management, CTD; MoHFW,India,2018.
- Return from Patient, Nikshay Aushadhi User Manual, CTD, MoHFW, India.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Return of drugs from the parent store is facilitated on Ni-kshay Aushadhi through which of the following options?
Return from patient
Return Request Desk
Both of the above
None of the above
2
In Ni-kshay Aushadhi, return from the parent store is facilitated through the ‘Return Request Desk’.
Yes
Yes
Recording reconstitution in Nikshay Aushadhi
ContentBox reconstitution means to unpack the prepared boxes into loose medicine. The loose medicine is then added back to the inventory of the store where reconstitution is done. Any box whether complete, incomplete, or modified can be reconstituted. Reconstitution can be done at State Drug Store (SDS) and District Drug Store (DDS) level only and once reconstituted, the box will no longer exist in the inventory. The process of reconstitution in Nikshay Aushadhi is known as box unpacking and involves the following steps:

Figure 1: Overview of process of recording of reconstitution in Nikshay Aushadhi
Detailed procedure:
Step 1: Go to the Nikshay Aushadhi website and click on login. Enter your user ID, Password, the captcha text and click login.
Step 2: Reach the ‘Box unpacking’ window following the path Home-menu>services>packing/repacking>Box unpacking and select your store. Select the TB subcategory then drug name and click on the ‘go’ tab.
Step 3: The system will show all the available boxes (complete, incomplete, and modified) with batch number, expiry Date, stock Quantity, and Stock Status. Select the desired box to be unpacked.

Figure 2: Box unpacking window in Nikshay Aushadhi
Source: Nikshay Aushadhi portal
Step 4: Once selected the system will show details of the drugs in that box. Any quantity less than or equal to the stock quantity of that box can be unpacked. For example, if the stock quantity of the selected box is 100 then any number of boxes between 1 and 100 van be unpacked. Specify the number of the boxes to be unpacked and then click the ‘save’ tab to complete the process. Upon completion, the system will generate the ‘box unpacking complete’ alert. After unpacking the box, the drugs from the box will be added loose into the inventory.

Figure 3: Saving details of box reconstitution
Source: Nikshay Aushadhi portal
Resources
Nikshay Aushadhi Manual-Central TB Division, Ministry of Health and Family Welfare, Government of India
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Box unpacking can be done at
SDS
DDS
Both 1 and 2
At any store
3
Box unpacking can be done at SDS, and DDS level only
YES
YES
-
Pharmacist: Transportation
FullscreenTransportation of Supplies under NTEP
ContentTimely procurement and an uninterrupted supply of medicines and other consumables are important requirements for the successful implementation and sustainability of the programme.
In a vast country like India where >70% of the population resides in rural areas, it is a challenge to transport sputum samples, drugs, consumables and other items on time and subsequently may result in delayed diagnosis and treatment initiation.
To combat this, the National TB Elimination Programme (NTEP) developed a multi-sectoral engagement strategy and entered into agreements with various ministries like the railways, road transport, aviation and communications for transportation of NTEP supplies and specimen transport across the countries through one of these modes.
Various Transportation Modes Utilised under NTEP for the Transport of Drugs and Other Supplies
Transportation Service
Activity
Indian Railway
The railway network is utilised for the supply of drug consignments from State/ District drug stores to far-flung areas. Ministry of Railways has also extended support to NTEP in terms of supply chain management and technical support for the implementation of TB-related activities across the country through railway medical services.
Indian Postal Services
Provides universal access to the rapid diagnosis of TB by specimen transportation from peripheral health facility to TB diagnostic laboratory, maintaining specimen quality while also respecting the timelines; delivering drugs across the country; and also fulfilling the submission of the TB notification forms to the Nodal Officer.
Air Transport Services
NTEP undertakes the transportation of the equipment as well as drug consignments through air cargo from various warehouses to the State Drug Stores on a routine basis as well as during emergencies.
In some situations, where the sputum specimens are required to be transported to the reference laboratories from various parts of the country, air transport of specimens is carried out to ensure efficient and timely testing.
Couriers
Third-party courier services are identified by NTEP in almost every district in the country and are given the responsibility to transport supplies and specimens from one centre to another while strictly adhering to the guidelines. The District TB Officer (DTO) is responsible for ensuring the quality of the transportation process through these courier services.
Government Vehicles
Vehicles are provided to the Senior Treatment Supervisor (STS)/ Senior TB Laboratory Supervisor (STLS) which are utilised in supply chain management, i.e., to deliver medicines to patients' homes as well as to collect samples for testing and follow-up, from the patients in their homes.
Third-party Logistics (3PL)
Central TB Division (CTD) has offered 3PL services at the district level where the agency is providing the transport services to pick the supplies from the District Drug Stores (DDS) and supply them to the TB Unit (TU) level. At present, 3PL service is being offered to all the DDS under the NTEP.
Significance
-
Utilising the existing government facilities for the transport of supplies is a cost-effective strategy.
-
Quick transportation of specimens can lead to effective TB testing and enhance the resulting output.
-
Early diagnosis and treatment initiation can contribute to minimising the further transmission of disease.
-
Strengthening the NTEP's supply chain management system to ensure the last-mile delivery of drugs.
-
Timely availability of drugs and other related supplies can majorly contribute to the treatment outcome.
-
Reaching out to the key populations served by various ministries such as workers, miners, migrants, tribal populations, women & children, etc. who are also highly vulnerable to TB.
Resources
-
Procurement, Supply Chain Management & Preventive Maintenance, Module 6, CTD, MoHFW, India.
-
MoU between Ministry of Railways, GoI and Central TB Division, MoHFW, India, 2019.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following services does India Post provide in collaboration with NTEP?
Initiation of treatment
Changing treatment regimen
Transport of sputum specimens and other supplies.
All of the above
3
Indian post supports NTEP in specimen transportation from peripheral health facility to TB diagnostic laboratory as well as in the supply of drugs and other items.
Yes
Yes
-
Key considerations during transportation of Supplies
ContentTransportation in a supply chain refers to the movement of products from one location to another, which begins at the start of the supply chain as materials make their way to the warehouse and continue all the way to the end-user.
The following considerations should be kept in mind before transporting the supplies:
Packaging
Proper packing of supplies is the most important aspect of transportation. Following are the components of good packaging:
- Labelling: All the supplies should be labelled properly before transportation. The important information which should be displayed on the labels include product name/ content, product strength (for drugs only), batch number, date of manufacturing, date of expiry, and storage conditions requirement. Safety instruction in the form of labels (like fragile, temperature-sensitive, direction) should be pasted on the boxes.
- Radio Frequency Identification (RFID)/ Barcode Scanning: Barcoding of packages before transporting ensure better tracking of the packages. In addition, entering data using barcoding is fast and reliable, significantly reduces human error and increases efficiency, and easy identification of product information.
- Security: Supplies that are damaged upon arrival can cause major problems. Not only do we lose the cost of the original item and shipping, but we may also have to send replacements at an additional cost. Hence, it is important that the supplies are packed in such a manner that the packaging keeps them safe during the transit.
- Storage Conditions: Majority of the supplies transported under National TB Elimination Programme (NTEP) are temperature sensitive and fluctuations above or below the manufacturer’s labelled storage temperature range may adversely affect product quality. Hence, the supplies should be transported in such a manner that the transportation temperatures meet manufacturer’s instructions.
Resources
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Why is barcode important during transportation of drugs?
Fast and reliable data entry
Decreases scope for human error
Makes product identification easy
All the above
4
For ensuring better tracking and supply chain management, the packages should ideally be bar coded before transporting. Use of barcodes offer the following advantages:
• Entering data using bar coding is fast and reliable
• Significantly reduces human error and increases efficiency
• Easy identification of product information.
YES
YES
Supply to DDS/TU
ContentThe following supplies are sent to the District Drug Store (DDS)/ TB Units (TUs):
- Anti-TB drugs (first and second-line):
Drugs once received by the State Drug Store (SDS) are transported to the districts. The districts then transfer the drugs to the TUs which in turn supply them to the Peripheral Health Institutes (PHIs).
- Diagnostic materials
The following diagnostic materials will be supplied by the SDS to the DDS and TUs:
- Cartridge-based Nucleic Acid Amplification Testing (CBNAAT) machines and cartridges
- Truenat machines and chips
- Binocular Microscopes (BMs) and Light Emitting Diode (LED) Fluorescence Microscopes (FM)
- Laboratory consumables: Sputum containers, slides, and 50 ml centrifuge tubes.
- Treatment-related supplies
These include the following:
- Syringes
- Needles
- Water for injections
- Water containers
- Disposable tumblers, etc.
- Stationery, forms, Information, Education and Communication (IEC) materials
Different registers, forms, and IEC material will also be supplied from the SDS to the DDS/ TUs.
Transportation
The states may hire Third-party Logistics (3PL) for transporting these supplies to the DDS and TUs.
Resources
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What is included in the supplies from the SDS to the DDS and TUs?
Diagnostic materials
Anti-TB drugs and treatment-related supplies
Stationery, forms, IEC materials
All the above
4
The supplies from the SDS to the DDS and TUs include diagnostic materials, anti-TB drugs, treatment-related supplies, stationery, forms and IEC materials.
Yes
Yes
Supply from TU to PHI
ContentBased on the reports from Ni-kshay Aushadhi, the stock is supplied from SDS to the district drug store to its Tuberculosis Units (TUs) and then to the Peripheral Health Institutions (PHIs).
This is done through the transport agencies which is hired from Central /State level.
Below is the details of transport mechanism from SDS TO DDS & DDS TO TU.

Figure 1. Operational flow from SDS TO DDS

Figure 2. Operational flow from DDS TO TU
Resources
1. Standard Operating Procedure Manual Procurement & Supply Chain Management RNTCP, MoHFW, GoI 2018
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
PHI Stocks will be given for
One month
first month along with a reserve stock of one month
Two month along with a reserve stock of one month
Three month
2
PHI Stocks will be given for first month along with a reserve stock of one month
-
-
M-6: PHI Pharmacist: Supervision, Monitoring and Evaluation and QA
Fullscreen-
Ph-Ch29:Quality Assurance of Drugs
FullscreenWhat is Quality Assurance of Drugs in NTEP?
ContentProcurement of good quality anti-Tuberculosis (TB) drugs and ensuring the quality of drugs till the consumption point is one of the prime objectives of National TB Elimination Programme (NTEP).
To ensure the quality and efficacy of anti-TB drugs, a comprehensive NTEP Quality protocol has been developed and is being followed during the procurement mechanism and supply chain management of drugs up to the consumption points. Simultaneously, quality assurance of anti-TB drugs has also been aligned with Ni-kshay Aushadhi application for easy reporting and recording from the Central to the peripheral level.

Fig 1: Quality assurance of drugs under NTEP
Resources
1. Standard Operating Procedure Manual- Procurement & Supply Chain Management; RNTCP, MoHFW, GoI 2019.
2. NTEP training modules 5-9; Central TB Division, MoHFW, GoI 2020.
Assessment:
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What is included in the quality assurance of drugs under NTEP?
Pre-dispatch inspection
Post-dispatch inspection
All of the above
None of the above
3
NTEP protocol for quality assurance of drugs includes mandatory pre-dispatch inspection and post-dispatch inspection
Yes
Yes
Protocol of QA of drugs in NTEP
ContentQuality Assurance of Drugs in NTEP is it ensure that, Each drug used by a patient is safe, efficacious and has appropriate standards of quality.
Procurement of good quality anti TB drugs and ensuring quality of drugs till consumption point is one of the prime objectives of NTEP. To ensure quality and efficacy of anti TB drugs, a comprehensive Quality protocol has been developed and is being followed during the procurement mechanism and supply chain management of drugs up to the consumption points.
Sample Collection Protocol
Maintaining quality of drugs, a system of pre-dispatch & post-dispatch testing of drugs is established.
As per the protocol developed by CTD-
Random samples of First / second-line anti TB drugs shall be picked from all stocking points in the field.
Sent for testing by an independent drug testing laboratory contracted by CTD.
This should be done based on communication sent by CTD to the concerned states and districts.
Resources
1. NTEP Training Modules 5to9, Central TB Division, MoHFW, GoI 2020
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
State true or false:
First line anti-TB drugs are procured from WHO pre-qualified sources only
True
False
1
First line drugs are procured from World Health Organization (WHO) pre-qualified source & second line drugs from WHO Good Manufacturing Practices (GMP) compliant suppliers under domestic budget (DBS)/World Bank (WB) procurement.
Process for QA of drugs in NTEP
ContentPre -Dispatch Inspection
- CTD to procure drugs through the Procurement Agency
- Procurement Agency will award contract to the Manufacturer/Suppliers after following the technical specification
- As per Technical Specification, Manufacturer will conduct pre-dispatch inspection for Quality Check
- Once clean report is received, the drugs to be dispatch to the consignee (GMSD/CMSS/SDS
- CTD hires a Lab agency
- Lab Agency pick drugs from the sites as per directed by the CTD
- Picked drugs will be sent to Laboratories by agency for Testing
- Test report to be shared with CTD
- CTD to disseminate the reports to all level
Resources
- Standard Operating Procedure Manual-Procurement & Supply Chain RNTCP, MoHFW, GoI 2019
Assessment:
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Drugs for quality assurance are collected from each zone on a quarterly basis
True
False
1
- All implementing NTEP State Drug Stores (SDS), District Drug Stores (DDS), Central Medical Service Society (CMSS) warehouses/Government Medical Store Depots (GMSDs) and Tuberculosis Units (TUs) have been arranged on a zone-wise basis i.e. North, South, East and West.
- Each quarter, drug samples are collected from selected zone as per direction of the Central TB Division.
Collection of drugs for testing
ContentDirections for collection of drug quantities for testing
- Central Tuberculosis (TB) Division will issue directions every quarter to concerned Government Medical Store Depots (GMSDs) and states for the collection of drug samples as per National TB Elimination Programme (NTEP) Quality Assurance (QA) protocol.
- Directions will be accompanied by the name of the drugs and the number of batches to be collected from respective drug stores.
- Generally, at least two batch numbers of drug samples selected randomly shall be sampled for testing from GMSDs, State and District Drug Stores.
- From Tuberculosis Unit (TU), only one batch number of drugs may be sampled. In case of stock shortage, samples will not be taken from TU.
Table 1: Quantities as per formulations to be collected for testing
S.No
Formulation
Quantity for collection
1.
Tablet
10 strips
2.
Capsule
10 strips
3.
Injectable
80 vials
4.
DSTB-IP / (A) 4FDC
8 Blister Strips
5.
DSTB-CP (A) / 3FDC-A
8 Blister Strips
6.
DSTB-IP (P)/ 3FDC-P
8 Blister Strips
7.
DSTB-CP (P) / 2FDC-P
8 Blister Strips
Procedure for collection of drug samples for testing

Figure 1: Overview of collection and sending of drug samples for quality testing in NTEP
The following procedure should be followed for the collection of drug samples:
1. As far as possible, the officer-in-charge should draw drug samples from original, unopened boxes /containers/ packs.
2. The sample drawn shall be divided into two equal parts, one half to be sent to the contracted laboratory in sealed condition and another half to be retained at the drug store in sealed condition.
3. The sealed pack of drugs collected should indicate on its label or otherwise:
(1) Drug name
(2) Quantity
(3) Batch No.
(4) Date of Manufacturing
(5) Date of Expiry
(6) Supplier Name
(7) Procurement Agency
(8) Manufacturing License No.
(9) Source of collection besides caution (if any) printed on the label for use/ storage of the product.
4. Information as above should be repeated in a covering letter, sealed and sent along with the sealed sample to the laboratory.
5. A copy of the covering letter should also be sent to Central TB Division.
6. Sample quantities collected should be such that the samples collected can be analyzed twice (as indicated above, by dividing into two equal batches).
7. Half of the sample collected should be sent to the selected laboratory in a sealed condition and the remaining half-sample of the same batch should be retained in sealed condition at the concerned drug stores until the lab report on the sample is received.
8. Record the quantities issued to testing laboratories in the stock register and Ni-kshay Aushadhi.
Resources
1. Standard Operating Procedure Manual-Procurement & Supply Chain Management; RNTCP, MoHFW, GoI 2019.
Assessment:
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer Correct explanation Page id
Part of Pre-test
Part of Post-test
Drug samples collected for quality assurance should be divided into 2 equal parts.
True
False
1 The sample drawn shall be divided into two equal parts, one half to be sent to the contracted laboratory in sealed condition and another half to be retained at the drug store in sealed condition. Follow up after drug testing
ContentQuality Assurance (QA) reports
- The contracted laboratory for quality assurance of National TB Elimination Programme (NTEP) drugs shall share drug quality reports as per the defined timelines to Central TB Division (CTD).
- The stipulated time is about 20 days for parenteral formulations & about 15 days for other drugs (capsule/tablets).
- Once quality reports of drugs are shared by the contracted laboratory, the same shall be shared further with the states.
The sealed drug samples may be opened and used in case the lab report indicates acceptable quality. However, in case of drug samples are declared as sub-standard, necessary action shall be taken by the CTD.
CTD shall communicate to the State about the sub-standard drugs and update the reports in Ni-kshay Aushadhi. Consequently, said batches which are declared sub-standard, shall be segregated in the Ni-kshay Aushadhi.
Precautionary Measures in Case of Sub-standard Drugs
- Stocking units down the line shall immediately be instructed to stop further consumption and issues from the batch declared substandard.
- Specific instructions shall be given to stocking units / Directly Observed Therapy Shortcourse (DOTS) centres to replace unconsumed drugs of a substandard batch from boxes/ drugs allocated to patients with drugs of a different batch.
- Unconsumed/ unused substandard drugs shall be labelled ‘substandard’ and carefully segregated in stores, in such a way that there is no possibility of their being reissued to patients.
- A detailed record shall be kept of segregated substandard drugs taken.
- CTD shall take all further necessary action for declared sub-standard drugs with concerned procurement agencies.
Repeat Testing
The following procedure is to be followed in case of a declared sub-standard drug:
- Laboratory reports suggesting sub-standard drugs may be challenged/disputed by the manufacturer/ supplier and they may request CTD to carry out an additional laboratory test through an independent, government-approved agency, e.g. Central Drugs Laboratory (CDL), Kolkata.
- CTD shall accordingly give instruction to Central Medical Services Society (CMSS)/ concerned Government Medical Store Depot (GMSD)/ State Drug Store (SDS)/ District TB Centre(DTC) /Tuberculosis Unit (TU) for dispatching the sample retained in sealed condition, for another round of testing to CDL, Kolkata. If a repeat testing report suggests that the quality of drugs tested is good enough for general administration, then instructions shall be issued by CTD to CMSS/GMSD/ SDS/ DTC and Stocking Units to resume issues/ consumption thereof. In case repeat testing confirms the sub-standard quality of drugs, CTD shall send a copy of the report to the procurement agency for further necessary action.
Resources
1. Standard Operating Procedure Manual- Procurement & Supply Chain Management; RNTCP, MoHFW, GoI 2019.
Assessment:
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
In how many days should the Quality Assurance Report for parenteral formulations be available?
30 days
20 days
90 days
10 days
2
The stipulated time is about 20 days for parenteral formulations & about 15 days for other drugs (capsule/ tablets).
Recording of QA in Nikshay Aushadhi
ContentContent
After receiving directions about the collection of drug samples for QA from Central TB division, the respective stores need to record all the details in the Nikshay Aushadhi. Various steps involved in this process are as follows:
Process overview:

Detailed procedure
Step 1: Go to the Nikshay Aushadhi website and click on login. Enter your user ID, Password, captcha text and click login.
Step 2: Reach the ‘Drug Quality Inspection Issue Detail’ window following the path:
Home>Services>Quality Control Management> Drug Quality Inspection Issue Detail.
Step 3: Click on the ‘drug finder’ Tab and select drug and batch number required for testing and enter the quantity.
Note: This quantity has to be retained at respective drug store in sealed condition till further instructions from Central TB division.
Step 3: Click ok to save your selection and repeat Step 2 to add more drugs if any.
Step 3: Enter desired details- lab name, controller ID and Controller name in the relevant columns and click on ‘Save’ tab to complete the process.

Figure 1: Saving the details
Source: Nikshay Aushadhi portal
Resources
1.Standard Operating Procedure Manual Procurement & Supply Chain Management- Central TB Division, Ministry of Health and Family Welfare, Government of India 2018
2.Nikshay Aushadhi Manual-Central TB Division, Ministry of Health and Family Welfare, Government of India
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
How often the drugs from selected zones as per directions of CTD are goes for post procurement QA to the independent laboratory
Hired by NTEP?
Annually Monthly
Quarterly
weekly
Quarterly
QA post procurement-
Drugs lying at GMSDs, SDS, DDS and TU drug stores picked up for testing by an independent laboratory hired by the programme.
Quarterly collection of drugs from selected zones as per directions of CTD by NTEP hired independent laboratory
Desk monitoring of supply chain
ContentDesk monitoring of supply chain
Desk monitoring of supply chain refers to the process of remotely monitoring drug stores in the network for their activities and performance. Under NTEP, this process can be done through Nikshay Aushadhi. Nikshay Aushadhi may help in real-time monitoring of supply chain by generating various reports related to consumption, requirement, and expiry management. Following are the ways that will enable the officer-in-charge to effectively monitor the supply chain through Nikshay Aushadhi.
Generation and Analysis of reports
Nikshay Aushadhi autogenerates a number of reports that keep a track of the stock availability, consumption, and expiry of supplies. These include Stock in Hand Record, Stock ledger report, expiry details report, Issue report, Stock ledger report, receipt register and issue register.
Analysis of the reports enable the Officer in-charge to ensure that adequate stock of supplies for consumption is available at the stores. At the same time, it will highlight the stores that are overstocked, understocked, or have supplies that have a near expiry date. This would allow the supervisor to take timely actions to ensure that these imbalances are corrected without any wastage.
Random checks
In addition to reviewing and analysis of monthly/quarterly reports, the officer in-charge may randomly check the reports at any point in time to ensure that the records about the receipt and consumption of supplies are updated on real time basis.
Audit trails:
The officer in-charge can check the audit trails i.e., transaction related to the receipt and consumption of supplies by analyzing the reports to ensure that relevant records are maintained on real-time basis. The officer in-charge through this process would be able to check information about the receipt, consumption, and balance stock of any item in the inventory at random.
Performance of the sub-stores
Analysis of reports such as the enquiry status will enable the officer in-charge to assess the performance of the sub-stores in terms of their Nikshay Aushadhi usage status. Analysis of these records will help in determining whether the relevant entries are being done on real time basis or not. In addition to this, thorough inspection of the reports will give officer in charge a fair idea about quality and accuracy of the data entered by the sub-stores.
Any problems/gaps identified can be discussed with the sub-stores through regular video conferencing.
Resources
Standard Operating Procedure Manual Procurement & Supply Chain Management, Ministry of Health and Family Welfare, Government of India 2018
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Analysis of Nikshay Aushadhi reports helps in ensuring adequate stocks True False
1
Analysis of the reports enable the Officer in-charge to ensure that adequate stock of supplies for consumption is available at the stores. At the same time, it will highlight the stores that are overstocked, understocked, or have supplies that have a near expiry date.
-
Ph-Ch31:Store Visits
FullscreenStore Visits in NTEP
ContentThis is a type of monitoring method, which is used to review and analyse the real situation. This is not only comprise of matching stock with the reports. It covers all the aspects of supply chain from infrastructure, people,stock,reporting etc. The filed visits are comprises of the following components.
Assessment:
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
NTEP store visit includes the checklist of
Drug Stock register
Reconstitution register
Both Answer 1&2
None of the above
3
Relevant details to be checked at state level & district level during store visit are:
- Space assessment for drug store.
- Infrastructure for drug store.
- Human resources.
- Transportation.
- Physical verification.
- Training and capacity building workshops
- Expired / sub-standard drugs.
- Packaging of second line anti-TB drugs (Second Line anti-TB Drugs) in monthly patient wise boxes (PWBs).
- Documentation
- Recording and reporting formats
- Drug resistant TB (DR-TB) report
- Reconstitutions register
Checklists for Store Visit in NTEP
ContentSignificance of Checklist
- The person who conducts supervisory visits should ensure that the health workers are performing their job adequately. S/he should observe personnel at work, review records and forms for completion and accuracy, and speak to the staff about their job responsibilities, case- finding, treatment outcomes, etc.
- Supervisory visits provide an opportunity to evaluate the training programme and to identify staff who needs to build additional skills, or who have other training needs. Supervision is the opportunity to give on the job training to such staff if feasible and in case there is no progress in performance even after on the job training, there is a need for assessing the quality of training received.
- The supervisor should also interact with community leaders and with patients, to assess their perception of the programme and to discuss with them the means for improving the services and community support.
- A staff member may not be adequately performing his/her job because of lack of skills or knowledge. The person evaluating the performance must determine the specific skill or knowledge in which the person is deficient. S/he should recommend and ensure that the staff member is retrained.
- A questionnaire may be used to evaluate quality of training. These include Pre-Test, Post- Test and Follow-up of the trainees using the tool (questionnaire / interview).
- Transfer of knowledge (gained during the training) into the skills can be assessed after few months up to a year by observing the activities being performed by the personnel on the job/ indicators where applicable and comparing the same with earlier performance of the similar nature.
The Parameter to be considered : -
- Space Assessment
- Infrastructure
- Human Resource
- Physical verification
- Transportation
- Management of SLD
- Recording and Reporting
Resources
1. NTEPTrainingModfdules5to9.pdf
https://tbcindia.gov.in/WriteReadData/NTEPTrainingModules5to9.pdf
2. Central Internal Evaluation Checklist NTEP
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Common observations made in SDS,DDS,TU are:
Stock register
FEFO
Both Stock register & FEFO
Only Stock register
3
Common observations are made in SDS,DDS,TU in both stock register & FEFO
Documenting the store visit
Content- Team may document observations of the visit in supervisory register maintained at PHI level in order to ensure continuity in supervisory efforts (in duplicate).
- One copy may be retained at PHI and one copy may be kept along with team for reference.
- Record important observations of the visit
- Communicate the observations to staff and appropriate authorities
- Keep track of actions taken on the recommendation
- Action taken may be sought within 1 month till district level and 2 months for state and central level supervisory visits.
Resources
- NTEPTrainingModules5to9, Central TB Division, MoHFW, GoI 2020
- Central Internal Evaluation Checklist NTEP
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Documenting store visit includes:
Checking Stock register
Checking
FEFO
Checking Both Stock register & FEFO
Checking Only Stock register
3
Documenting store visit check the Both Stock register & FEFO
-
PHI Pharmacist : PHYSICAL VERIFICATION
FullscreenPhysical Verification of supplies
ContentPhysical verification of stores is the process of actual counting, weighing and measuring all items of stocks, recording the results and to ensure that the materials are according to the nomenclature, description, specification shown in the stock ledgers and to actual balances of such stocks agree with balances appearing in the book and are confirmed and authenticated.
If any, the excess or shortage brought to notice on such verification is properly investigated, accounted for and reconciled.
Why is physical verification important?
- It is an audit requirement that physical verification of all stocks are carried out at least once a year.
- Essential, as it checks the accuracy of store records and brings about an overhaul of the store section, especially its physical condition.
- Useful as it discloses any weakness or defects in the system for the custody and control of stocks, besides bringing the stock accounts up-to –date.
- Reveals the possibility of frauds, thefts or loss and suggests the adoption of additional preventive measures to stop them.
- Reveals losses due to wrong issues, negligence, misappropriations, misuse or leakage, pilferage, theft etc. and suggests measurement to stimulate better control.
- Helps in clearing up surplus and obsolete items, thus avoiding locking up resources.
- Ensures that the stores are well preserved against any damage or deterioration due to improper storage or other hazards.
- Valuable as it greatly assists in training the staff and measuring the more conversant with store keeping methods and techniques.
Physical verification of the inventory of anti-TB drugs and reconciliation thereof with store records shall be carried out under the supervision of the concerned officer-in-charge at the State Drug Store (SDS), District TB Centre (DTC), Tuberculosis Unit (TU) & Peripheral Health Institution (PHI) drug stores at the following times:
- Regularly at the end of each month
- Surprise / spot verification by the Director or his nominee
- At the year-end
Resources
- Procedure of Physical verification of stores; Council of Scientific & Industrial Research (CSIR), 2004.
2. Standard Operating Procedure Manual Procurement & Supply Chain Management; RNTCP, MoHFW, GoI, 2018.
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Physical verification of supplies are carried out
End of each month
Surprise checks during the year
At the year-end
All of the above
4
Physical Verification of supplies carried out
1. End of each month
2. Surprise checks during the year
3. At the year-end
Steps for Physical verification of supplies in different stores
ContentPhysical verification and reconciliation of anti-TB drug stocks are done at the drug stores, and immediate next steps are taken to deal with discrepancies determined, if any.

Figure 1: Flow chart of process of physical verification
Table 1: Format for Physical Verification Sheet (PVS) -Reporting Unit: State Drug Stores (SDS)/ District TB Centre (DTC)/ Tuberculosis Unit (TU)
S.No
Drug
UOM
Qty &DOE as per stock register
Qty &DOE as per physical count
Discrepancy between stock register and physical count
Nature of discrepancy
How discrepancy was dealt with
Remarks
(a)
(b)
(c)
(d)
(e)
(f=d-e)
(g)
(h)
(i)
UOM: Unit of Measurement, QTY: Quantity, SR: Stock Register
Resources
- Standard Operating Procedure Manual Procurement & Supply Chain Management; Central TB Division, MoHFW, GoI 2018.
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of these are included in the steps for Physical Verification of supplies in different stores?
UOM
Qty & DOE as per stock register
Qty & DOE as per physical count
Discrepancy between stock register and physical count
All of the above
Steps for Physical Verification of supplies in different stores include:
- UOM
- Qty & DOE as per stock register
- Qty & DOE as per physical count
- Discrepancy between stock register and physical count
Recording of Physical Verification in Ni-kshay Aushadhi
ContentPhysical Verification of stock is a two-step process:
- Physical Verification of Supplies
- Recording the Change in Ni-kshay Aushadhi
Image
- Fill the details as per Ni-kshay Aushadhi as well as the physical stock in the PSV excel format.
- It might be a change in quantity of stock or addition of new batch of the specific drug
- Get the format signed by the Medical Officer
- Each store will have one PSV sheet format filled, verified and signed by the MO
For example, if a TBU has 5 PHIs, then there will 6 PSV sheets (one for the TBU store and one each for the 5 PHIs)
Image
- Open ‘Physical Stock Verification’ form. and click on ‘GO’ button.
- In ‘To be verified drug details’ the system is showing already existing drugs and batches present in the inventory.
- Select the drug, with the batch number and enter the quantity into the ‘Counted Qty’ column, which is physically available at the store.
- To remove a batch or a drug, enter ‘0’ into the ‘Counted Qty’ column.
- Click on ‘Final Save’ button.
- If no further changes are required, follow the ‘Second Step’ of Physical Stock Verification to update the stock.
Image
In case of New Batch - enter the details of the new batch or new drug to add, and enter the ‘Remarks’ and click on ‘Add’ button
Image
- Click on ‘GO’ button again
- System will show 4 options, ‘M’ to modify the record, ‘C’ to cancel the record, ‘V’ to view the record’ and ‘S’ to final upload the stock.
- Click on ‘S’ to upload the stock.
- The system will generate the voucher,
- The changes will be updated in drug inventory of the store.
-
Fullscreen