-
M 01: National TB Elimination Program [NTEP]
Fullscreen-
TS: Tuberculosis
FullscreenTuberculosis
Content
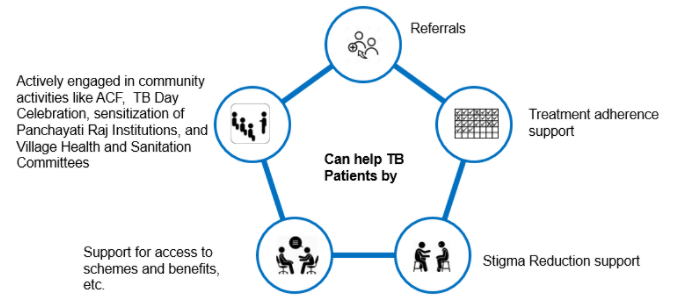
Figure: Causative agent for Tuberculosis is Bacillus: Mycobacterium tuberculosis (M.tb)
-
Tuberculosis (TB) is a communicable disease that is a major cause of ill health.
-
TB is caused by the bacillus Mycobacterium tuberculosis (M.tb)
-
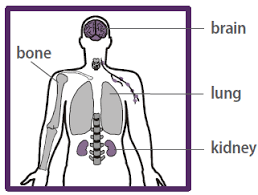
TB disease typically affects the lungs (pulmonary TB) (80%) but can also affect other parts of the body (extra pulmonary TB) (20%)
-
It spreads when people who are sick with TB expel bacteria into the air (for example by coughing, sneezing, shouting or singing)
-
It is one of the top 10 causes of death worldwide and the leading cause of death from a single infectious agent
Resources
- Global Tuberculosis Report, 2020; Geneva: World Health Organization, 2020
- Training Modules (1-4) for Programme Managers and Medical Officers India: Central TB Division, MoHFW, Government of India,July 2020
-
Burden of TB in India
ContentTB is one of the top burdensome infectious diseases in India. It is estimated that, around 1/4th (26%) of the world's TB cases are in India, translating to about 30 Lakhs new TB cases emerging each year (TB incidence). Against this estimated incidence the National TB Elimination program reported around 19 lakh new and relapse cases in the year 2021.
An estimated 5 Lakhs deaths occur due to TB each year in the country, translating to about 1 case of TB death every one-two minutes. Compared to this, there are only about 60 thousand deaths due to HIV and about 77 deaths due to Malaria each year.
TB diagnosis and treatment services although provided free of cost in the public sector, the cost of accessing these services and related loss of wages drive the affected people with poverty (catastrophic costs). TB also has a huge impact on the world's and the country's economy because of loss of workdays (100 million workdays per year).
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test What is the estimated number of incident TB cases that emerge each year in India? 35 Lakh cases 26 Lakh Cases 26% of the Global Burden 19 Lakh Cases 2 The estimated number of new and relapse (incident) cases in India that emerge each year is about 26 Lakh Yes Yes How many cases of deaths are estimated to be caused by TB in India Approximately One death every 2-3 minutes Approximately 5 Lakh deaths 60 Thousand deaths each year 1 and 2 4 In India it is estimated that there is around one death caused due to TB every one to two minutes, translating to about 5Lakh deaths each year in India Yes Yes Resources:
TB Causative organism
Content
Figure Mycobacterium tuberculosis
TB is caused due to the infection by a bacterium called Mycobacterium tuberculosis.

Figure: Extra-Pulmonary Tuberculosis
It often affects the lungs, and in such cases it is called Pulmonary Tuberculosis. But, it can affect almost any part of the body (except the hair and the nails), in which it is known as Extra-Pulmonary Tuberculosis.
Resources:
Determinants of TB Disease
ContentDeterminants are any characteristics that affect the health of a patient.
Biological Determinants Behavioral Determinants Socio Economic Determinants Occupational Determinants - People living with HIV(PL HIV)
- History of contact with a case of TB
- People with underlying medical conditions like Diabetes, Kidney disease, Cancer etc.
- Existing lung disease
- Old age
- Use of tobacco and alcohol
- Malnutrition
- Person in contact with TB infected patient
- Person living in areas with poor ventilation & over crowding
- Poverty and Malnutrition
- Homeless
- Mining work
- Quarry work(Silicosis)
- Construction work
- Migrant worker
- Daily wagers
Vulnerable Population for Tuberculosis
ContentTB can affect anyone but it is more prevalent in some communities which are vulnerable to TB disease due to various factors which are mentioned below:
Increased exposure of TB due to where they live or work
- prisoners
- slum dwellers
- miners
- hospital visitors
- healthcare workers
Limited access to Quality TB services
- Migrant workers
- Women in settings with gender disparity,
- Children
- Physically challenged
- Transgender population
- Tribal and population living in hard to reach areas
- Refugees or internally displaced people
- Illegal miners and undocumented migrants
Increased risk because of biological or behavioural factors that compromise immune functions in people who:
- People who live with HIV
- have diabetes or silicosis
- undergo immunosuppressive therapy
- are undernourished
- use tobacco
- suffer from alcohol use disorders.
- inject drugs
Mode of TB Transmission
ContentTuberculosis is transmitted mainly through the air via droplet nuclei generated when a TB patient coughs or sneezes.
It is estimated that every sputum smear-positive patient spreads the infection to 10 – 15 persons annually, if untreated..

Figure: Transmission of TB bacteria through air via droplet
Resources:
- Technical and Operational Guidelines for TB Control in India 2016
- WHO - Fact sheet details on Tuberculosis
Kindly provide your valuable feedback on the page to the link provided HERE
Symptoms of TB Disease
ContentActive TB disease has 4 major symptoms (the 4 Symptom complex). Presence of any one of these symptoms without any other reason warrants evaluation for TB. These are:

Figure: Signs and Symptoms of TB
People affected with TB may experience other symptoms as well. These may be based on the site that is affected with TB or other more non-specific symptoms of an infection. The physician or doctor would evaluate these symptoms in view of diagnosis of TB.
Resources:
Progression to TB Disease
ContentAfter exposure to infective droplets containing M.TB, only a small proportion gets infected and further progresses to active TB disease.
- Majority of those that get infected persist in a stage of clinical latency known as TB infection (previously known as Latent TB infection). They do not have TB disease and do not show any symptoms of TB and no evidence of any TB related changes on chest X-ray.
- A small proportion of those with prior infection may progress to active TB disease due to various environmental/ agent/ host factors.

Figure: Flow chart for TB disease progression
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
TB Infection
Content-
TB Infection (or previously known as Latent TB infection) is a stage in between uninfected and having active TB. In this stage the person has no symptoms and can only be identified using laboratory tests.
-
The vast majority of infected people may never develop TB disease. However, to achieve TB elimination, it is important to treat TB infection in people at risk of developing active TB disease.
-
It is a state of persistent immune response to stimulation by Mycobacterium tuberculosis antigens with no evidence of clinically manifested active TB.
-
There is no single acceptable/reliable test for direct identification of Mycobacterium tuberculosis infection in humans. Tuberculin Skin Test (TST) and Interferon-gamma release assay (IGRA) are commonly used tests for identifying TB infection.
Resources:
-
TB Infection Vs Active TB Disease
ContentTB Infection Active TB Disease May not have any signs & symptoms Has sign and symptoms such as cough for more than two weeks, fever, weight loss and blood in sputum Has dormant, contained bacteria is the body Has active, multiplying bacteria in the body Doesn't spread TB bacteria to others May spread TB bacteria to others Chest X-ray usually normal Lesion in Chest X- ray (usually) May advance to active TB. It is estimated that the lifetime risk of an individual with TB infection for progression to active TB is 5–10%. Needs treatment for TB disease Resources:
-
TS: NTEP
FullscreenNational TB Elimination Program [NTEP]
Content- The National Tuberculosis Elimination Program (NTEP) is the public health initiative of the Government of India that organizes the country’s Tuberculosis Elimination efforts.
- NTEP is a centrally sponsored scheme being implemented under the aegis of the National Health Mission with resources sharing between the State Governments and the Central Government.
- The program provides various free of cost, quality tuberculosis diagnosis and treatment services across the country.
Image
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers; New Delhi, India: Central TB Division, MoHFW, Government of India, July 2020
- India TB Report 2021
Kindly provide your valuable feedback on the page to the link provided HERE
Tuberculosis Unit [TU]
ContentTuberculosis (TB) unit (TU) is the sub-district level supervisory unit of National TB Elimination Program with the following organogram:
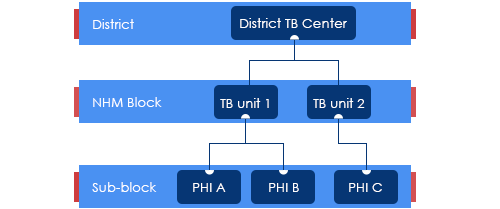
Figure: Organogram of a TB Unit
(PHI: Peripheral Health Institution)
TUs are based mainly on National Health Mission (NHM) health blocks with the aim of aligning with the NHM Block Programme Management Unit (BPMU) for optimum resource utilization and appropriate monitoring.
The TUs have been created based on a population of 1 per 2,00,000 (range 1.5 – 2.5 lakh) for rural and urban populations and 1 per 1,00,000 (0.75 – 1.25 lakh) population in hilly/tribal/difficult areas.
The TU consists of a designated Medical Officer-Tuberculosis Control (MO-TC), as well as one full-time supervisory staff - Senior Treatment Supervisor (STS). However, one Senior TB Laboratory Supervisor (STLS) will be there in every 5 lakh population (one per 2.5 lakh population for tribal/hilly/difficult areas), mostly covering 2-3 TUs.
TB Unit manages the provision of TB services (Diagnosis, Treatment, Prevention, etc.) and programme management in the assigned geographical area.
Resources
Stages in TB Patient's Lifecycle
ContentThose who are suspected of having TB disease are first screened for symptoms like cough and fever for more than 2 weeks, blood stained sputum and weight-loss. If found positive on screening, then TB patients are referred for testing to the nearest health facility. If diagnosed with TB, then they are subsequently initiated on treatment. The TB patients initiated on treatment are regularly monitored with the help of field staff or digital interventions like 99DOTS and MERM (Medication Event Reminder Monitor) technology. NTEP staff also ensures that the TB patients are regularly followed up on monthly basis till their treatment completion.

Figure: Patient Flow
Kindly provide your valuable feedback on the page to the link provided HERE
Categorization of TB Treatment Regimen
ContentDaily Regimen is prescribed for TB patients, where patients need to consume the medicine daily.
Daily Regimen comprises of the first line Anti TB drugs, based on
- Age: Adult/Paediatric
- Weight of the patient: Weight Bands
Age: Based on the age, patients are categorized into
- Adults: Patient's age should be 19 years or more.
- Paediatrics: Patient's age up to 18 years and weight less than 39 Kgs
Weight Bands:
- Treatment dosage is based on the TB patient’s weight.
- A weight band category is defined for Adult and Paediatric patients separately and medicines are issued based on that weight category.
TB Case classification in NTEP
ContentTB cases are generally classified on the basis of previous history of TB treatment into New and previously treated cases.
New case - A TB patient who has never had treatment for TB or has taken anti-TB drugs for less than one month is considered as a new case.
Previously treated patients have received 1 month or more of anti-TB drugs in the past. They could be further classified as:
- Recurrent TB case - A TB patient previously declared as successfully treated (cured/treatment completed) and is subsequently found to be microbiologically confirmed TB case is a recurrent TB case.
- Treatment After failure patients are those who have previously been treated for TB and whose treatment failed at the end of their most recent course of treatment.
- Treatment after loss to follow-up - A TB patient previously treated for TB for 1 month or more and was declared lost to follow-up in their most recent course of treatment and subsequently found microbiologically confirmed TB case
- Other previously treated patients are those who have previously been treated for TB but whose outcome after their most recent course of treatment is unknown or undocumented.
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Patient interaction with TB Care Ecosystem
ContentHealth Volunteers/ Treatment Supporters are often the regular point of contact for a TB patient in the community. They support the TB patient during the entire episode of TB and ensure complete diagnosis and treatment. The next points of contact are with the MPHWs who periodically visit the patients to ensure specific delivery of services.
The Peripheral HeaIth Institution (PHI) is the nearest accessible health facility where the patient can access a physician/ doctor for diagnosis and treatment services. These are often in the form of a Primary Health Centre, but can also be higher level institutions such as medical colleges and private health facilities that are most accessible to/ preferred by the patient. The PHI may also host a drug store/ pharmacy from where the patient's medicines would be dispensed.
Other health facilities with diagnostic services such as DMCs, NAAT Sites and C&DST Labs may be accessed by the patient or by their biological specimen being collected and transported to the corresponding laboratory. Other higher order health institutions such as DRTB Centres may also be accessed by the patient on referral.
The District TB Centre, TB Unit and its staff provide programmatic support and supervision indirectly through the PHI. At times the National Call Centre may contact the patient for providing specific information, or for collecting feedback on quality of service delivery.

Figure: Stakeholders interacting with HVs
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Role of Health Volunteers
ContentHealth Volunteers
- are members of the communities where they work,
- are supported by the health system but not necessarily a part of its organization,
- and have shorter training than professional workers”

Figure: Role of Health Volunteers
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
-
Ch 03: TB Diagnosis and Case Finding
FullscreenPresumptive TB
ContentPresumptive TB case refers to a patient who presents with symptoms or signs suggestive of TB disease (previously known as a TB suspect) and where further diagnostic workup including bacteriological investigation is required.
Presumptive TB can be categorized into
-
Presumptive Pulmonary TB (P TB) - Symptoms are directly related to lungs (Cough, hemoptysis)
-
Presumptive Extra Pulmonary TB (EP TB) - Symptoms/ signs are specific to an extra pulmonary site (example: Lymph node swelling)
-
Presumptive Pediatric TB - Symptoms of TB in young children are more difficult to identify and can be more general (fever, weight loss)
Resources:
- Technical and Operational Guidelines for TB Control in India 2016
- Definitions and reporting framework for tuberculosis
Kindly provide your valuable feedback on the page to the link provided HERE
-
Presumptive Pulmonary TB
ContentPulmonary TB(PTB) is primarily involves lungs. Screening should be done for the following symptoms:
Figure: Signs and Symptoms of active TB
Regular screening of Presumptive TB cases with unexplained cough of any duration should be done and checked for:
- History of close contact with known active TB case
- Whether the patient has developed Presumptive/confirmed extrapulmonary TB(EPTB)
- High-risk groups: PL HIV, Diabetics, Malnourished, Cancer patients, patients on immunosuppressive therapy or steroids
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Testing for TB diagnosis
ContentNational Tuberculosis Elimination Programme (NTEP) strives for all presumptive TB patients to be microbiologically confirmed. Under NTEP, the acceptable methods for microbiological diagnosis of TB are:
Sputum Smear Microscopy (for Acid Fast Bacilli - AFB): Sputum Smear microscopy is the primary tool which is reliable, inexpensive, easily accessible and rapid method of diagnosing PTB, where in the bacilli are demonstrated in the sputum. Two types:
-
Ziehl-Neelsen Staining
-
Fluorescence staining
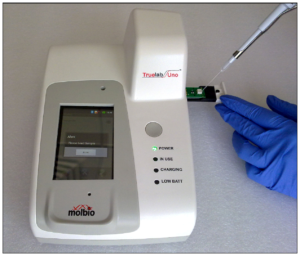
Rapid diagnostic molecular test: Rapid molecular tests that use techniques like NAAT are very specific. They amplify the genomic material in the patient sample and hence enhances detection
-
Nucleic Acid Amplification Test (NAAT) e.g., GeneXpert, TrueNat
Figure: Genxpert Machine for CBNAAT
Figure: Truenat Machine
- Line Probe Assay
Culture and DST: A culture test involves studying bacteria by growing the bacteria on different substances. This is to find out if particular bacteria are present. In the case of the TB culture test, the test is to see if the TB bacteria Mycobacterium tuberculosis, are present.
Two types:
-
Solid (Lowenstein Jensen) media
-
Liquid media (Middlebrook) e.g., Bactec MGIT etc.
-
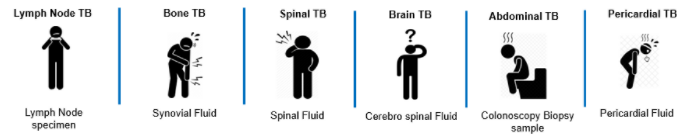
Biological Specimen for Diagnosis of TB
ContentFor laboratory diagnosis of TB, different biological specimens are used.
Pulmonary TB: Sputum sample is used. Sputum is a thick fluid produced in the lungs and in the adjacent airways. Normally, a spot sample and a fresh morning sample is preferred for the bacteriological examination of sputum.
Extra Pulmonary TB:
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Sputum Collection Process
ContentPresumptive TB patients attending the TB Diagnostic centre (TDC) will be referred for sputum examination at the same facility. The patients are given the sputum container with laboratory serial number written on its side. The patient is:
Figure: Sputum Collection Process
- Provided with the labelled sputum cups and demonstrated how to open and close the container.
- Given a labelled container with instructions to cough out sputum into the container early in the morning after rinsing the mouth with water. This is the early morning specimen. This is labelled as Specimen ‘b’.
- Ensure collection of sputum samples in an open, well-ventilated area designated for this purpose.
- Given a sputum container with instructions to collect an early morning specimen and go with the sputum specimen to the TDC(if the health facility is not a TDC) where the spot specimen can be collected. If the patient cannot travel to the TDC, then the spot specimen could be collected at the nearest health facility or sputum collection centre and transported to the TDC.
Video fileVideo: Process of sputum collection
Resources:
Role of Health Volunteers in TB Case Finding
Content- Community Health Volunteers play a significant role in increasing awareness regarding the burden of TB and the importance of preventing it and regularly screening the population.
- Community Health Volunteers should use the various platforms in the communities, such as the PRI meetings, school meetings etc., for spreading the information on TB. Using such media, the Community Health Volunteers should focus on building community awareness to improve the patients' health-seeking behaviour.
- Community Health Volunteers should screen the vulnerable population for Tuberculosis during the Active Case Finding Campaign. Positive TB suspects identified should then be referred for testing, post which, if diagnosed with TB, should be initiated on treatment.
- Community Health Volunteers should also ensure that those TB patients initiated on treatment adhere to the treatment.
- Community Health Volunteers should also record the population screened; sputum examined cases, diagnosed cases and patients initiated on treatment.
- Community Health Volunteers should also confirm the patient's address in their respective locality for correct patient identification.
Kindly provide your valuable feedback on the page to the link provided HERE
Prevention of TB
ContentAs TB is an airborne infection, TB bacteria are released into the air when someone with infectious TB coughs or sneezes. The risk of infection can be reduced by taking simple precautions:
Figure: Measures for control and prevention of tuberculosis
TB Preventive Treatment(TPT) also has a very important role in prevention of TB. Presently, household contacts of sputum-positive TB patients are given TPT upon confirmation of TB infection and ruling our active Tuberculosis.
Resources:
-
Ch 04: Nikshay & Treatment Supporter
FullscreenNikshay
ContentNikshay is an Integrated ICT system for TB patient management and care in India. Nikshay was launched in 2012 and since then, various improvements have been made in the system.
Nikshay provides-
- A Unified interface for public and private sector health care providers
- Different types of Logins such as State, District, TU, PHI, Staff logins, Private providers, Chemist, Labs and PPSA/JEET Logins
- Integration of all adherence technologies such as 99DOTS and MERM
- Unified DSTB and DRTB data entry forms
- Mobile friendly website with mobile app
Nikshay is accessible either via web browser(https://Nikshay.in ) or mobile App called ‘Nikshay’ that can be downloaded from Google Play Store(Android).
Figure: Nikshay Login Pages
Nikshay interfaces- Web and Mobile application
ContentFigure: Nikshay Home Page
After login in Nikshay, using the login credential shared by NTEP Health Staff, Treatment Supporter will be able to access the following button:
- New Enrolment: Allows to enrol new cases in Nikshay
- Search Patient: Allows to search for patients that are mapped to him /her, using Patient Name, Nikshay ID and Old Nikshay ID
- Add Patient Test: Allows to add tests for all the patients.
- Diagnosis Pending: View the list of the patients that are pending for diagnosis
- Not on Treatment: View the list of the patients that are diagnosed but pending to be initiated on treatment
- On Treatment Patients: Gives the list of on treatment patients
- Outcome assigned: Gives the list of the patients that have completed their treatment
- Training Material; Access the training content available on Nikshay
- Patient Summary: Gives a brief overview on the Presumptive cases registered, Diagnosed and patients that are initiated on treatment
- Task List: Allows to view the list of pending activities pertaining to adherence, Treatment Outcome and Bank details missing for mapped patient
- Latest Updates: New updates of features that are released on Nikshay
TB Aarogya Sathi
ContentTB Aarogya Sathi empowers Citizens(including TB Patients under NTEP) and to serve as a Direct interface with the healthcare system. The App is aimed at augmenting the initiatives of the Central TB Division, Government of India in proactively increasing awareness among the citizens and ensuring availability of free and quality assured drugs and diagnostics to all citizens in the country.
Citizens using the TB Aarogya Sathi App will have access to common FAQs regarding TB, Information on the symptoms of TB and Side effects of Anti TB drugs. Using the app, any user will be able to find the closest health facilities that can assist in diagnosis of TB.
Patients registered with Nikshay will have access to the Adherence, Treatment Progress and DBT Details.
Citizen:
- Informative Content available for all Citizens using the App(no login required to access this content)
- Information on TB
- Symptoms of TB
- Side Effects of TB
- Health Facility Search
- BMI Assessment
- Nikshay Sampark Helpline
- Motivational Videos
- Nutritional Advice
Patient:
- Patients registered in Nikshay get access to additional information(after login)
- Adherence Details
- Treatment Progress Details
- DBT Details
TB Aarogya Sathi App is available in Google play store and can be download using this QR Code
Figure: TB Aarogya Sathi Application snapshot
- Informative Content available for all Citizens using the App(no login required to access this content)
-
-
M 02: Treatment Support and Monitoring of TB Patient
Fullscreen-
Ch 05: TB Treatment and Care
FullscreenDrug-Sensitive Tuberculosis(DS-TB)
ContentWhat is Drug-Sensitive Tuberculosis (DS-TB)?
-
DSTB is a case where a person is infected with TB bacteria that are susceptible to all first line anti-TB drugs. It means that all of the first line TB drugs will be effective as long as they are taken properly and regularly.
-
This type of TB has the best prognosis and the shortest treatment duration.
-
Patients diagnosed with TB are considered to be DS-TB case, till such time s/he detected with resistance to any anti-TB drugs.
Kindly provide your valuable feedback on the page to the link provided HERE
-
DSTB Treatment Phases
ContentDSTB Treatment duration is of 6–9-month course of antibiotics. The duration and drug dosage used may vary according to a patient’s age, type of TB infection, and whether s/he has been treated before.
The standard 6-month course of treatment consists of two phases.
Intensive Phase(IP)
Continuation Phase(CP)
- The first phase lasts 2 months.
- 4 drug regimen(HRZE) is given as part of IP.
- The second phase lasts 4 months
- 3 drug regimen(HRE) is given as part of CP.
*Extension of CP: Depending upon response to treatment or type of disease, physician may decide to extend the treatment by 3 months.
Treatment Regimen for DSTB – Adult
ContentIntensive Phase(IP): Consists of eight weeks (56 doses) of HRZE in daily dosages as per weight of patient.
Continuation Phase(CP): Consists of 16 weeks (112 doses) of HRE in daily dosages as per weight of patient.
For adults, there are five weight bands, as shown in the table below. The table also indicates the number of FDC tablets that have to be consumed in each weight band
Weight band category
Intensive phase(IP)
(HRZE - 75/150/400/275)
Continuation phase(CP)
(HRE - 75/150/275)
25–34 kgs
2
2
35–49 kgs
3
3
50–64 kgs
4
4
65–75 kgs
5
5
>=75 kgs
6
6
Regular monthly follow up of the patient needs to be done and if patient loses or gains approx. 5 kg weight and if weight band changes during the treatment, then the dose of the patient needs to be recalculated.
Fixed Dose Combinations [FDC]s
ContentFixed-dose combinations (FDCs) are drug formulations where two or more drugs are combined physically into one formulation such as a tablet or pill.
This is more convenient to the patients taking medicines and it also simplifies the supply chain.

Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
FDCs used in NTEP
ContentImage
Adverse Drug Reactions(ADRs) to First Line Treatment
ContentSymptoms
Drug Responsible
Action to be taken by Community Health Volunteers
Gastrointestinal Symptoms
Any Oral Medications
-
Reassure patient.
-
Give TB Drugs with less water at a longer interval.
-
If symptom persists, refer to the nearest health facility
Itching/Rashes
Isoniazid
-
Reassure patient.
-
In case of severe itching, refer the patient to the nearest health facility
Tingling/ burning/ numbness in the hands & feet
Isoniazid
-
Refer the patient to the nearest health facility
Joint Pains
Pyrazinamide
-
Reassure patient.
-
Increase intake of liquids.
-
If severe, refer the patient to the nearest health facility
Impaired Vision
Ethambutol
-
Refer the patient to the nearest health facility
Ringing in the ears, Loss of hearing, Dizziness and loss of balance
Isoniazid, Rifampicin or Pyrazinamide
-
Refer the patient to the nearest health facility
Hepatitis: Anorexia/ nausea/ vomiting/ jaundice
Isoniazid, Ethambutol, Rifampicin or Pyrazinamide
-
If patient detected with signs of jaundice, refer the patient to the nearest health facility
-
Follow-up of TB patient
ContentTo know the TB treatment response and to determine that if patient is cured, TB patients are clinically evaluated at the end of every four weeks of treatment, and they are also followed up by performing sputum test at end of each treatment phase (i.e. Intensive phase and Continuation phase)
TB patients during clinical evaluations are assessed to
- Identify possible adverse reactions to medications;
- Check for any comorbid conditions;
- Weight change;
- monitor adherence; and determine treatment efficacy by observing their symptoms
Although each patient responds to treatment at a different pace, all TB symptoms should gradually improve and eventually go away.
Patients whose symptoms do not improve during the first 2 months of treatment, or whose symptoms worsen after improving initially, should be re-evaluated for adherence issues and development of drug resistance.
Long Term Post-treatment follow up of TB patients
ContentAfter completion of TB treatment, all patients should be followed up at the end of
- 6 months,
- 12 months,
- 18 months &
- 24 months
TB patients at the follow up should be screened for any clinical symptoms and/or cough. If found positive on screening, then sputum microscopy and/or culture should be considered. This is important in detecting the recurrence of TB at the earliest.
After completion of TB treatment, if the patient has not developed any clinical symptoms and/or cough and also if the microscopy remains negative during their follow up, then the patient is considered as “Relapse Free Cure from TB.”
Drug-Resistant Tuberculosis(DR-TB)
ContentWhat is Drug-Resistant Tuberculosis?
-
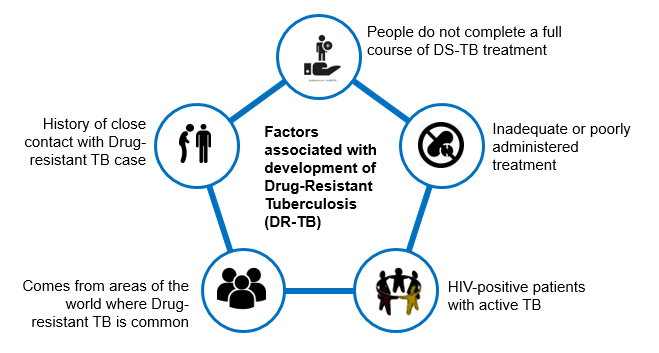
Drug-Resistant TB occurs when bacteria become resistant to the drugs used to treat TB. This means that the drug can no longer kill the TB bacteria.
-
Multidrug-resistant TB (MDR TB) is a type of DR-TB where TB bacteria is resistant to both Isoniazid and Rifampicin, the two most potent anti-TB drugs.
Figure: High Risk for Drug-Resistant Tuberculosis (DRTB)
Resources:
-
Adverse Drug Reactions(ADRs) to Second Line Treatment
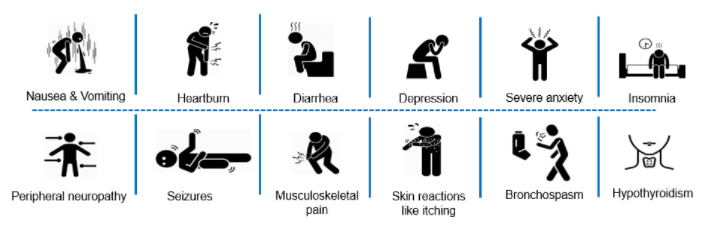
ContentCommon Adverse events to second line treatment are as below
Figure: Adverse Drug Reaction to Second line drugs
Adverse events should be identified, monitored and be referred to
- Nearest treating doctor for minor symptoms or
- District DR-TB Centres for major symptoms
If required, hospitalization can be done at the District DR-TB Centers where inpatient facility is available or referred to a Nodal DRTB Centre for admission
TB Infection
Content-
TB Infection (or previously known as Latent TB infection) is a stage in between uninfected and having active TB. In this stage the person has no symptoms and can only be identified using laboratory tests.
-
The vast majority of infected people may never develop TB disease. However, to achieve TB elimination, it is important to treat TB infection in people at risk of developing active TB disease.
-
It is a state of persistent immune response to stimulation by Mycobacterium tuberculosis antigens with no evidence of clinically manifested active TB.
-
There is no single acceptable/reliable test for direct identification of Mycobacterium tuberculosis infection in humans. Tuberculin Skin Test (TST) and Interferon-gamma release assay (IGRA) are commonly used tests for identifying TB infection.
Resources:
-
Regimen for TPT
ContentThe following TPT treatment options are recommended under NTEP once active TB has been ruled out:
6H
3HP
Medicines
Isoniazid
Isoniazid + rifapentine
Duration (months)
6
3
Interval
Daily
Weekly
Doses
182
12
Pregnant women
Safe for use
Not Known
Post-treatment TPT for PLHIV: In patients previously treated for TB, post-treatment TPT has been considered in view of the 5-7 times higher risk of recurrence of TB among PLHIV and nearly 90% of these due to re-infection. Thus, all CLHIV/PLHIV who had successfully completed treatment for TB disease earlier should receive a course of TPT after completing treatment of TB.
Resources
-
Guideline for Programmatic Management of Tuberculosis Preventive Treatment in India
-
Latent TB Infection : Updated and Consolidated Guidelines for Programmatic Management, WHO, 2018
Kindly provide your valuable feedback on the page to the link provided HERE
-
-
Ch 06: Treatment Adherence
FullscreenTB Treatment Adherence
ContentTuberculosis(TB) is curable if patients are treated with effective, uninterrupted anti-tuberculous treatment. Treatment adherence is critical for curing individual patients, controlling the spread of infection in the community, and minimizing the development of drug resistance.
Adherence to treatment means that a patient follows the recommended course of treatment by taking all the prescribed medications for the entire length of time, as necessary. In other words, “right dose for the right duration”.
In Drug Sensitive Tuberculosis(DSTB), a TB patient completes 168 doses of TB treatment and adheres to TB treatment.
Importance of Treatment adherence
ContentAdherence to tuberculosis(TB) treatment is important for promoting individual and public health. Poor adherence to TB treatment results in:
- More individual suffering and death,
- Costly treatment as treatment regimens lengthen and
- Increases the risk for Drug Resistant Tuberculosis
Proper treatment of all forms of TB is critical to reducing individual morbidity and mortality and to interrupting transmission among family and community members.
Recording and Monitoring Adherence
ContentRecording of Treatment Adherence can be done as
- Manually by DOT/Health Care Provider in TB Treatment Card of a patient.
- Self-reported by Patient using digital tools for reporting adherence using 99 DOTS and MERM technologies.
Monitoring Treatment Adherence:
All TB patients should be monitored to assess their response to TB treatment. Nikshay Adherence calendar has a colour legend for various doses taken by a patient
Figure: Sample Nikshay Adherence Calendar in web and Mobile App
COLOUR LEGEND DOSE DESCRIPTION Treatment Start /End Denotes Treatment start and End Date Digitally Reported Dose Denotes that the patient has successfully called the Toll Free Number displayed on the envelope Manually Reported Dose Indicates that the staff has marked manually confirmed dose for the day Unreported Dose Indicates that there was no call event received on Nikshay for that day Manually Reported Missed Dose Indicates that the staff has marked a manually confirmed missed dose for the day Digitally Reported(From Shared Phone Number) Indicates that the patient has been calling from a shaed number(A mobile number that is common for more than one patient) Image
Figure: DSTB Treatment Card (Paper)
Digital Adherence Monitoring Technologies
Content99DOTS is a low-cost digital adherence technology built-in Nikshay that uses inexpensive packaging(envelopes or stickers) with medication that enables people taking medication to engage with their treatment daily. This packaging, distributed to TB patients taking medications, has a hidden number behind perforated flaps on the external envelope; in some cases, the number may be fixed outside the medication blister or pill bottle. This number can be a toll-free number that can be called to register daily adherence or a code sent by SMS, USSD, or other communication channels. Calling or messaging the number is free!
Figure: 99 DOTS Envelope
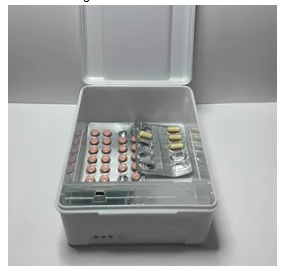
MERM: The Medication Event Reminder Monitor(MERM) is a digital pillbox that provides daily pill-taking reminders and facilitates remote monitoring of medication adherence. This system provides visual and audible reminders for both daily dosing and refill,.transmits this data to a server so that healthcare providers can remotely visualize patients’ dosing histories to support enhanced adherence counselling.
Figure: MERM Box
Recording manual doses in Nikshay
ContentManual recording of Adherence in Nikshay:
in Nikshay, Adherence can only be recorded only if there is corresponding dispensation being issued to a Patient
Figure: Steps to record manual dose in Nikshay
Recording in Patient Treatment Card:
Figure: Filled Treatment card for TB Patient
Recording missed doses in Nikshay
ContentMissed Dose recording in Nikshay:
For recording missed doses in Nikshay, following steps should be followed:
Role of Health Volunteers in TB Treatment and care
ContentAdministration of drugs and adherence to therapy
Community Health Volunteers should ensure supply and regular consumption of TB drugs by a patient, so that TB patients adhere to their treatment.
Monitoring of Adverse Drug Reactions
Community Health Volunteers should be able to do an early identification and referral for Adverse Drug Reactions(ADRs) to the nearest health facility of NTEP Programme.
Referral for Clinical & Lab Follow up of Patient as per TB Treatment schedule
Community Health Volunteers should ensure that the patient adheres to the regular monthly follow up and sputum test at the end of each treatment phase as per the TB Treatment guideline.
Community Health Volunteers should also help in recording of TB recurrence in a patient on Nikshay platform(i.e., old details with new episodes)
Maintaining records of TB patients and linkages with health systems
Community Health Volunteers should ensure that the necessary TB patient records are maintained at the nearest health facility, which in turn should be linked with the health systems.
Kindly provide your valuable feedback on the page to the link provided HERE
-
-
M 03: Patient Support
Fullscreen-
Ch 07: Public Health Action
FullscreenPublic Health Actions
ContentPublic Health Action is conducted under the NTEP programme to support and prevent further health complications among TB patients after diagnosis.
Figure: Various activities under Public Health Action
Contact Tracing and Investigation
ContentContact tracing is a process to identify people who are at a high risk of developing TB due to their contact with a known TB case.
The aim of contact tracing is to find other people with TB disease and those infected with TB
All close contacts, especially household contacts of a Pulmonary TB patient, should be screened for TB.
In paediatric TB patients, reverse contact tracing for the search of any active TB case in the child's household must be undertaken.
Particular attention should be paid to contacts with the highest susceptibility to TB infection.
Figure: Contacts to be Prioritized for contact TB screening
Home visit to TB Patients
ContentInteraction with the patients and their families is crucial to gauge a patient's understanding of the disease he/she is suffering from and the course of treatment to be followed.
Aspects to be considered during a Home visit:
- First home visit should be completed within 7 days of the patient's diagnosis.
- Patients who have Adverse Drug Reaction(i.e. ADR) / interrupted treatment /Loss to follow up /Repeat episode, interrupted the treatment should be given preference and would be preferable if the In-charge of the health facility accompany the team during home visit.
Figure: Precautionary measures to be advised to patient during home visit
Treatment supporter to TB Patient
ContentA Treatment Supporter can be any person such as a Medical Officer, MPWs, community volunteers working with the program etc. Even a patient’s relative or family member can be a Treatment Supporter.
As per NTEP guidelines, salaried NTEP/General Health System staff may also be assigned as treatment supporters for a patient. However, they will not be eligible for any honorarium.
A patient can only be linked to one treatment supporter at a time in Nikshay.
Task performed by Health Volunteers on Home Visit to TB Patient
Content- Screening for four symptom complex for TB and refer for testing
- Support for treatment adherence
- By self-monitoring
- Patient /family counselling
- Peer group support meetings
- Counselling of TB Patients
- To report Adverse Drug Reaction(ADR), if any
- Adhere to the treatment and ensure treatment completion
- Regular monthly follows up during treatment
- Nutritional support
- Supporting the patients in getting linked with existing nutritional supplementation schemes
- Socio economic support
- Profiling of patients to determine eligibility for the scheme
- Support to file application for socio-economic schemes
- Collaboration with non-governmental sources
- Community engagement
- Promotion of other Health programmes.
-
STS: TB Arogya Sathi App
FullscreenTB Aarogya Sathi
ContentTB Aarogya Sathi empowers Citizens(including TB Patients under NTEP) and to serve as a Direct interface with the healthcare system. The App is aimed at augmenting the initiatives of the Central TB Division, Government of India in proactively increasing awareness among the citizens and ensuring availability of free and quality assured drugs and diagnostics to all citizens in the country.
Citizens using the TB Aarogya Sathi App will have access to common FAQs regarding TB, Information on the symptoms of TB and Side effects of Anti TB drugs. Using the app, any user will be able to find the closest health facilities that can assist in diagnosis of TB.
Patients registered with Nikshay will have access to the Adherence, Treatment Progress and DBT Details.
Citizen:
- Informative Content available for all Citizens using the App(no login required to access this content)
- Information on TB
- Symptoms of TB
- Side Effects of TB
- Health Facility Search
- BMI Assessment
- Nikshay Sampark Helpline
- Motivational Videos
- Nutritional Advice
Patient:
- Patients registered in Nikshay get access to additional information(after login)
- Adherence Details
- Treatment Progress Details
- DBT Details
TB Aarogya Sathi App is available in Google play store and can be download using this QR Code
Figure: TB Aarogya Sathi Application snapshot
- Informative Content available for all Citizens using the App(no login required to access this content)
Download the Tb Arogya Sathi App and Steps to Login
ContentVideo fileVideo: Download the Tb Arogya Sathi App and Steps to Login
Health Facilities
ContentVideo fileVideo: Health Facilities
Summary and Treatment Progress View
ContentVideo fileVideo: Summary and Treatment Progress View
View Adherence Details
ContentVideo fileVideo: Adherence Details and DBT Details View
View DBT Details
ContentVideo fileVideo: DBT Details View
Adding bank details in the Arogya Sathi App
ContentVideo fileVideo: Adding bank details in the Arogya Sath App
Symptom Checker-Overview
ContentVideo fileVideo: Symptom Checker-Overview
Screening for Self and Others
ContentVideo fileVideo: Screening for Self and Others
Post enrolment follow-up cycle in Nikshay
ContentVideo fileVideo: Post enrolment follow-up cycle in Nikshay
-
Ch 08: Counselling
FullscreenTB Awareness Generation in Community
ContentAwareness should be generated in the community for promoting various health programmes, health seeking behaviours, screening of TB cases etc. by involving and sensitizing community influencers including PRI members and treatment support groups.
Figure: Activities for awareness generation in community
Counselling of TB Patients
ContentConfidential dialogue between a health care provider and a patient that helps a patient to define his/her feelings, cope with stress, and to make informed decisions regarding treatment.
The patient should be counselled at all the three phases i.e.,
Pre-treatment counselling`
- About TB disease and treatment
- Air borne infection control
- Need for adherence
- Public Health Actions
- Identification of adverse events
- Tobacco /Alcohol cessations
- Identification of comorbidities
During Treatment Counselling
- Importance of Adherence
- Identification of adverse events
- Importance of timely follow ups
- Public Health Actions
- Tobacco /Alcohol cessations
- Management of comorbidities
Post treatment Counselling
- Testing at the end of treatment.
- Long term follow up
- Tobacco /Alcohol cessations
Objectives of TB Counselling:
- Prevention of TB transmission.
- Provision of emotional support to TB patients.
- Motivation of TB clients to complete treatment.
- Helping patients make their own informed decisions about their behaviour and supporting them in carrying out their decisions.
Figure: Characteristics of effective counselling
Do's & Don'ts for Patient Communication
ContentDo’s
- Active listening, emphatic gestures and expressions
- Ensure the confidentiality of the conversation done with the patient
- Ensure Minimum interruption during the conversation with patient
- Ensuring availability of IEC materials such as posters, videos, pamphlets etc. to dispel myths and misconceptions.
Don'ts
- Do not use any negative stereotypes
- Do not have any physical wall or glass between patient and yourself
- Do not breach the trust and confidentiality of the TB patient
- Do not make threats or use coercive language
- Do not exaggerate dangers or risk of TB
- Do not blame or shame TB patients
Nutritional Counselling for TB Patients
ContentNutritional Counselling begins with the nutritional assessment of TB patients by
- Nutritional Status: Assessing the height, weight and BMI of the TB patient
- Diet and Preference food for TB patients
- Current appetite and food intake of TB patients
Based on the nutritional assessment, the following information can be conveyed to TB Patients
- Patients with TB should be encouraged to have frequent food intake in the form of three meals and three snacks.
- Attempts should be made to increase the energy and protein content in the meals and snacks without increasing its volume.
- The addition of oil, butter or ghee to the chapati or rice can increase the energy content of the diet.
- Pulses in other forms, e.g. sprouts, roasted Chana, groundnuts, can be taken as snacks in either fried or in roasted form. Milk and eggs to be included in the diet.
- The use of easily available nutritious foods based on vegetarian/non-vegetarian preferences of the patients must be emphasized.
- Information about NFSA(National Food Security Act) and Poshan abhiyan should be given.
Figure: Healthy diet for TB Patients
-
Ch 09: Social Inclusion and Wellness Activity
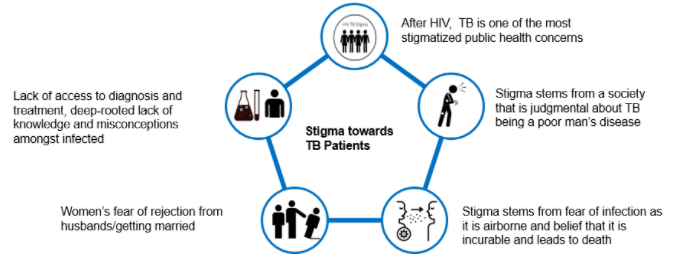
FullscreenStigma and Discrimination towards TB Patient
ContentStigma is when someone sees you in a negative way.
Discrimination is when someone treats you in a negative way.
TB patients face various forms of stigma and discrimination in the community
Figure: Stigma towards TB Patients in the community
Effects of Stigma on TB Patients
ContentAt Individual Level
- Lack of self-esteem and confidence
- Increased sense of emotional isolation, feeling of guilt and anxiety
- Physical as well as financial debilitation
- People, more often women, are forced to leave their homes
- Concealing symptoms and hesitancy in seeking medical care making disease management more difficult
- Delayed diagnosis, interrupted treatment that can lead to further transmission and DRTB
- Vulnerability increases, can lead to suicidal thoughts due to isolation and shame
At Family and Community Levels
- Loss of household earnings
- Exposure of caregivers to the risk of infection that lowers productivity and cycle of poverty further gets perpetuated
- Isolation and stigmatization of infected persons often by people of their community
- Deep-rooted lack of knowledge and misconceptions among the affected and infected within their cultural and religious environment
- Loss of status and negative impact on those with the disease, their caregivers, family, friends and communities
- Perceived and internalized stigma of the community due to socio-cultural values that TB is punishment for sins or transgression
Treatment Supporter Honorarium Eligibility
ContentTreatment supporters are eligible for Honorarium at the end of TB patients treatment, only if the patient's treatment outcome has been declared either as "Cured “or "Treatment Complete".
The eligible amount of honorarium is
- Rs. 1,000 for DSTB Patients and for
- Rs. 5,000 for DRTB patients.
These benefit amount are processed through Nikshay and below are the prerequisite conditions that needs to be met in Nikshay, for generating incentive
- Treatment supporter should be registered and enabled for receiving honorarium from Nikshay.
- Bank details of Treatment supporter should be submitted to the nearest NTEP health facility staff.
- In Nikshay, this is the only scheme where benefits are generated manually by TU users - STS
- Nikshay will allow NTEP TU users to generate benefits, only if
- Treatment Outcome has been declared as "Cured “or "Treatment Complete"
- Patient duplication status should be Unique i.e. Nikshay marks the patient duplicate based on Gender and Mobile Number
- For DSTB patient, one benefit of maximum amount of Rs. 1,000 can be created if outcome is updated as “Cured” or “Treatment Completed
- For DR TB patients two benefits can be generated in Nikshay:
- First benefit of maximum amount Rs. 2,000 can be created at end IP - Intensive Phase (i.e. Initiation Date + 6 months)
- Second benefit of maximum amount Rs. 3,000 can be created if Outcome is updated as “Cured” or “Treatment Completed”
-
CH 10: Community Engagement
FullscreenCommunity Engagement
ContentCommunity engagement is a process of developing relationships that enable stakeholders to work together to address health-related issues and promote well-being to achieve positive health impact and outcomes.
Mobilize communities to engage them in TB care and to increase ownership of the Programme by communities.
Why Community Engagement?
Figure: Importance of Community Engagement
Importance of Community Engagement in TB
ContentCommunity-based TB activities are conducted outside the premises of formal health facilities (e.g. hospitals and clinics) in community-based structures (e.g. schools and places of worship) and homesteads. Community health workers and community volunteers carry out community-based TB activities. Both can be supported by nongovernmental organizations and/or the government.
Community Engagement is a cost effective intervention to improve health service coverage and deliver accessible and people-centered integrated care.
Figure: Importance of Community Engagement
TB Champion
ContentA TB Champion is a person who has been affected by TB and successfully completed the treatment.
TB Champions, in their capacity as survivors, are role models and can provide valuable support to those with TB and their families.
Figure: Roles of TB Champion
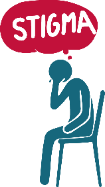
Community Health Volunteers should identify TB Champions and engage them to provide their support to the patient in activities like:
Figure: Help to TB Patients by Community Health Volunteers
Role of Health Volunteers in Community Engagement
ContentInvolve TB Champions: Community Health Volunteers should play a key role in the following aspects
- Identification from TB survivors in the community
- Training in various aspects of TB and role of TB Champions in NTEP activities
- Mentoring and grooming for providing support to TB patients as peer counsellors
- Supporting the formation & functioning of survivor-led networks at various levels
- Recognition and facilitation for good work on occasions like “International TB Day Celebration.”
Engaging community structures at village level: Community Health Volunteers should engage the community for the following:
- Active Case Finding
- TB awareness generation
- Stigma reduction
- Support for TB patients
Psychosocial Support to TB Patients:
- Offer words of encouragement, alleviate anxiety and create awareness.
- Promote kindness, solidarity, compassion; offer to talk to family & community members.
- Connect TB patients to TB community network, TB survivors.
- Have a gender-sensitive approach and ensure gender equality.
- Provide guidance on supportive interventions(e.g., refer to mental health helplines, share information on videos/resources available on MoHFW’s website).
- Choose words carefully while referring to those affected; form treatment support groups.
- Avoid using words like cases, victims, transmitters and suspects.
- Share key messages to prevent stigma; conduct stigma reduction interventions.
-
Ch 11: Linkages to Social Support Schemes
FullscreenDirect Benefit Transfer(DBT) under NTEP
ContentDirect Benefit Transfer (DBT) is a major initiative of Government of India (GoI) whereby any government subsidy or benefit is to be transferred directly into the beneficiary's bank accounts. Intermediary government agencies only manage the process of payments, without handling actutal money.
NTEP is one of the first health programmes in India to use a fully adopt DBT. It uses an end to end electronic system, to digitise beneficiary information and transfer monetary benefits. In NTEP to process benefits, two electronic systems are used, Ni-kshay (operated by NTEP) and PFMS (Public Finance Management System, operated by the Ministry of Finance). Ni-kshay enables Direct Benefit Transfer by digitizing the beneficiaries(bank account details of patients, treatment supporters and providers) and calculates of incentives/ benefits (eligible payment) and processes them for payment through PFMS under various schemes. The various schemes operational under NTEP are:
- Nikshay Poshan Yojana(NPY)
- Tribal Support Scheme
- Treatment supporter’s Honorarium
- Incentive for Notification and Outcome
DBT Schemes in NTEP
ContentSchemes Beneficiary Benefit Amount Nikshay Poshan Yojana(NPY) - All Notified TB Patients in Nikshay from the point of diagnosis
Rs. 1000 at the time of Notification and Rs 500 per treatment month there after paid in advance as installments. Tribal Support Scheme Confirmed TB Patients residing in Tribal TU Rs 750(one time) at the time of notification Treatment supporter’s Honorarium Treatment supporters of patients who have achieved outcome of treatment success - Rs 1,000 in the case of DS TB patients and Rs 5,000 in the case of patients, paid at the time of treatment completion.
Incentive for informants, Notification and Outcomes Private Health Facilities: including Practitioner /Clinic etc.(Single), Hospital/Clinic/Nursing Home etc.(Multi), Laboratories and Chemists
Any citizen reporting TB patients to public health facility or a self-reporting by patient may also be incentivized as an informant
- Rs 500 for Notification or informant
- Rs. 500 for Outcome declaration to health facilities.
Criteria for availing DBT Scheme benefits under NPY
Content- All TB patients notified on or continues treatment after 1st April 2018 including all existing TB patients under treatment are eligible to receive incentives.
- For availing DBT scheme benefits under NTEP Programme, TB patients have to provide their bank details to the nearest NTEP Health facility.
- The patient must be registered\notified on the NIKSHAY portal.
- Each beneficiary can be linked to unique savings bank account belonging to him/her. Beneficiaries without bank accounts need to be facilitated to open bank accounts in any bank as convenient.
- If a Beneficiary does not have a bank account and is unable to open a new bank account, his/her relative’s bank account may be used(immediate family member such as parents, spouse, siblings).
- If a relative’s bank account is used, written consent should be taken from beneficiary.
- If a bank account has already been used for another beneficiary, it cannot be re-used for another beneficiary. If a new Bank account needs to be opened, it’s easy to open a zero-balance account with Indian Post Payments Bank.
-
Fullscreen