-
IEC-M1: Basics of Tuberculosis and NTEP
Fullscreen-
IEC-CH 1: TB & TB Epidemiology
FullscreenTuberculosis
Content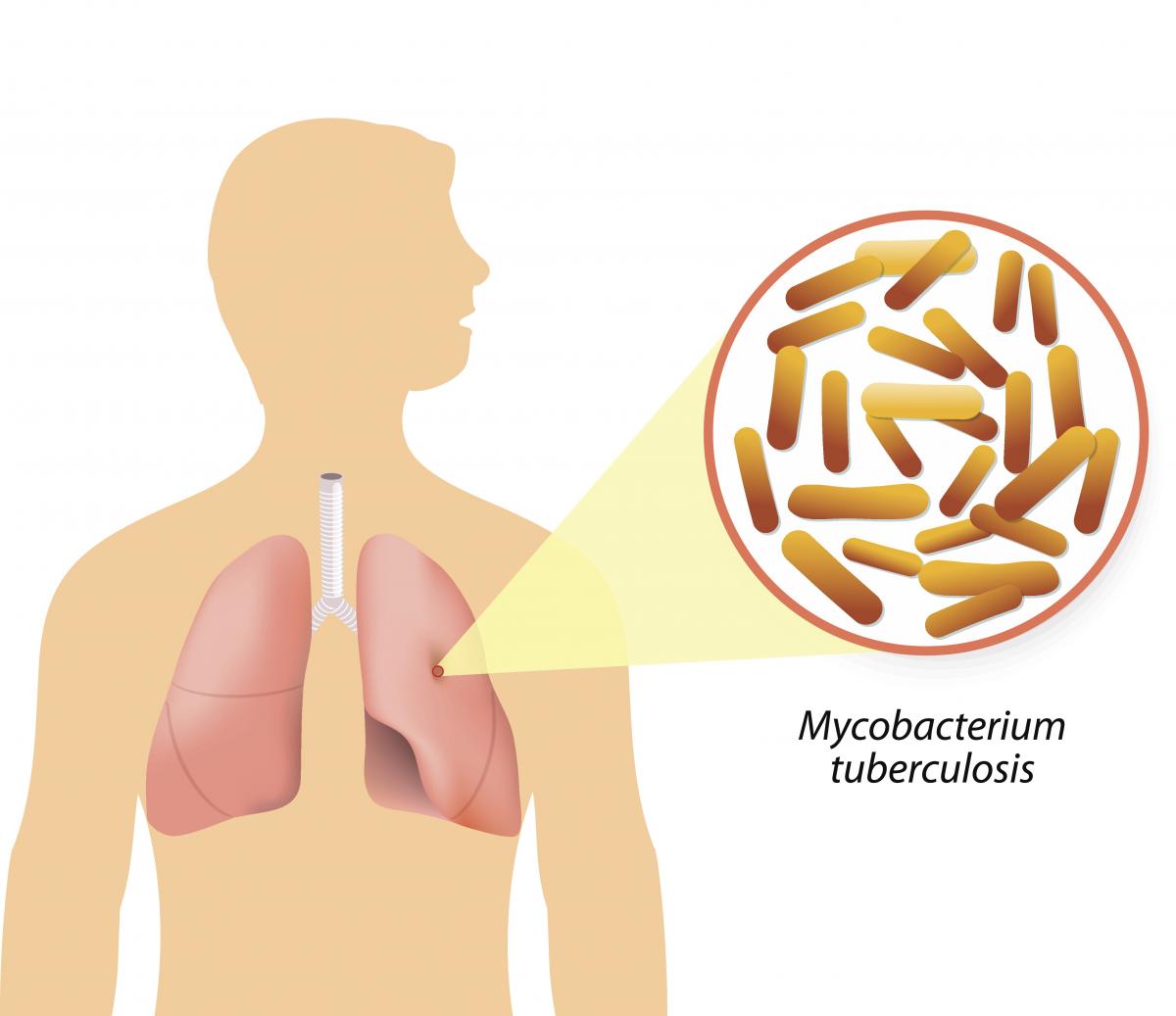
Figure: Causative agent for Tuberculosis is Bacillus: Mycobacterium tuberculosis (M.tb)
-
Tuberculosis (TB) is a communicable disease that is a major cause of ill health.
-
TB is caused by the bacillus Mycobacterium tuberculosis (M.tb)
-
TB disease typically affects the lungs (pulmonary TB) (80%) but can also affect other parts of the body (extra pulmonary TB) (20%)
-
It spreads when people who are sick with TB expel bacteria into the air (for example by coughing, sneezing, shouting or singing)
-
It is one of the top 10 causes of death worldwide and the leading cause of death from a single infectious agent
Resources
- Global Tuberculosis Report, 2020; Geneva: World Health Organization, 2020
- Training Modules (1-4) for Programme Managers and Medical Officers India: Central TB Division, MoHFW, Government of India,July 2020
-
Burden of TB in India
ContentTB is one of the top burdensome infectious diseases in India. It is estimated that, around 1/4th (26%) of the world's TB cases are in India, translating to about 30 Lakhs new TB cases emerging each year (TB incidence). Against this estimated incidence the National TB Elimination program reported around 19 lakh new and relapse cases in the year 2021.
An estimated 5 Lakhs deaths occur due to TB each year in the country, translating to about 1 case of TB death every one-two minutes. Compared to this, there are only about 60 thousand deaths due to HIV and about 77 deaths due to Malaria each year.
TB diagnosis and treatment services although provided free of cost in the public sector, the cost of accessing these services and related loss of wages drive the affected people with poverty (catastrophic costs). TB also has a huge impact on the world's and the country's economy because of loss of workdays (100 million workdays per year).
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test What is the estimated number of incident TB cases that emerge each year in India? 35 Lakh cases 26 Lakh Cases 26% of the Global Burden 19 Lakh Cases 2 The estimated number of new and relapse (incident) cases in India that emerge each year is about 26 Lakh Yes Yes How many cases of deaths are estimated to be caused by TB in India Approximately One death every 2-3 minutes Approximately 5 Lakh deaths 60 Thousand deaths each year 1 and 2 4 In India it is estimated that there is around one death caused due to TB every one to two minutes, translating to about 5Lakh deaths each year in India Yes Yes Resources:
Evolution of TB Elimination Programme in India
ContentThe National Tuberculosis Control Program (NTP) of India was launched in 1962. It relied on BCG, X-ray based diagnosis and Streptomycin and INH based treatment centralized at district level.
Based on a review of the NTP, and WHO recommendations of the DOTS Strategy, Government of India then revised the NTP and launched new program with the title Revised National Tuberculosis Control Program (RNTCP) in 1997. It used Sputum microscopy at DMC(Designated Microscopy Centres) for diagnosis, and multi-drug Short Course Anti-TB Therapy, decentralized to the TU (TB Unit) level.
In recognition of the rising drug resistance problem the DOTS Plus/ PMDT (Programmatic Management of Drug Resistant TB) was launched in 2006 and scaled up to the entire country by 2012.
Further to strengthen the monitoring and supervision system - a case based notification system - Nikshay was introduced in 2012. The same year Tuberculosis was added as a notifiable disease at the point of diagnosis by all health care providers.
Other key milestones from 2012 to 2020 were the availability of the Standards of TB Care in India (STCI) in 2014, introduction of the Daily weight band wise Fixed Dose combination (FDC) in 2016 and new drugs like Bedaquilline and Delaminid were started in 2017 and 2018 respectively.
To emphasise the commitment of the Government of India and to accelerate the efforts towards TB elimination, RNTCP was renamed as "National Tuberculosis Elimination Programme (NTEP)" in 2020.

Figure: Key milestones under NTEP
Resources:
Stages in TB Patient's Lifecycle
ContentThose who are suspected of having TB disease are first screened for symptoms like cough and fever for more than 2 weeks, blood stained sputum and weight-loss. If found positive on screening, then TB patients are referred for testing to the nearest health facility. If diagnosed with TB, then they are subsequently initiated on treatment. The TB patients initiated on treatment are regularly monitored with the help of field staff or digital interventions like 99DOTS and MERM (Medication Event Reminder Monitor) technology. NTEP staff also ensures that the TB patients are regularly followed up on monthly basis till their treatment completion.

Figure: Patient Flow
Kindly provide your valuable feedback on the page to the link provided HERE
TB Causative organism
Content
Figure Mycobacterium tuberculosis
TB is caused due to the infection by a bacterium called Mycobacterium tuberculosis.

Figure: Extra-Pulmonary Tuberculosis
It often affects the lungs, and in such cases it is called Pulmonary Tuberculosis. But, it can affect almost any part of the body (except the hair and the nails), in which it is known as Extra-Pulmonary Tuberculosis.
Resources:
Mode of TB Transmission
ContentTuberculosis is transmitted mainly through the air via droplet nuclei generated when a TB patient coughs or sneezes.
It is estimated that every sputum smear-positive patient spreads the infection to 10 – 15 persons annually, if untreated..

Figure: Transmission of TB bacteria through air via droplet
Resources:
- Technical and Operational Guidelines for TB Control in India 2016
- WHO - Fact sheet details on Tuberculosis
Kindly provide your valuable feedback on the page to the link provided HERE
Symptoms of TB Disease
ContentActive TB disease has 4 major symptoms (the 4 Symptom complex). Presence of any one of these symptoms without any other reason warrants evaluation for TB. These are:

Figure: Signs and Symptoms of TB
People affected with TB may experience other symptoms as well. These may be based on the site that is affected with TB or other more non-specific symptoms of an infection. The physician or doctor would evaluate these symptoms in view of diagnosis of TB.
Resources:
Progression to TB Disease
ContentAfter exposure to infective droplets containing M.TB, only a small proportion gets infected and further progresses to active TB disease.
- Majority of those that get infected persist in a stage of clinical latency known as TB infection (previously known as Latent TB infection). They do not have TB disease and do not show any symptoms of TB and no evidence of any TB related changes on chest X-ray.
- A small proportion of those with prior infection may progress to active TB disease due to various environmental/ agent/ host factors.

Figure: Flow chart for TB disease progression
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
TB Infection Vs Active TB Disease
ContentTB Infection Active TB Disease May not have any signs & symptoms Has sign and symptoms such as cough for more than two weeks, fever, weight loss and blood in sputum Has dormant, contained bacteria is the body Has active, multiplying bacteria in the body Doesn't spread TB bacteria to others May spread TB bacteria to others Chest X-ray usually normal Lesion in Chest X- ray (usually) May advance to active TB. It is estimated that the lifetime risk of an individual with TB infection for progression to active TB is 5–10%. Needs treatment for TB disease Resources:
Risk Factors for TB Disease
ContentFollowing are the risk factors that increase the chances of developing TB disease in an individual:

Figure: Risk factors for developing active TB
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Presumptive TB
ContentPresumptive TB case refers to a patient who presents with symptoms or signs suggestive of TB disease (previously known as a TB suspect) and where further diagnostic workup including bacteriological investigation is required.
Presumptive TB can be categorized into
-
Presumptive Pulmonary TB (P TB) - Symptoms are directly related to lungs (Cough, hemoptysis)
-
Presumptive Extra Pulmonary TB (EP TB) - Symptoms/ signs are specific to an extra pulmonary site (example: Lymph node swelling)
-
Presumptive Pediatric TB - Symptoms of TB in young children are more difficult to identify and can be more general (fever, weight loss)
Resources:
- Technical and Operational Guidelines for TB Control in India 2016
- Definitions and reporting framework for tuberculosis
Kindly provide your valuable feedback on the page to the link provided HERE
-
Prevention of TB
ContentAs TB is an airborne infection, TB bacteria are released into the air when someone with infectious TB coughs or sneezes. The risk of infection can be reduced by taking simple precautions:
Figure: Measures for control and prevention of tuberculosis
TB Preventive Treatment(TPT) also has a very important role in prevention of TB. Presently, household contacts of sputum-positive TB patients are given TPT upon confirmation of TB infection and ruling our active Tuberculosis.
Resources:
-
IEC-CH 2: NTEP
FullscreenEvolution of TB Elimination Programme in India
ContentThe National Tuberculosis Control Program (NTP) of India was launched in 1962. It relied on BCG, X-ray based diagnosis and Streptomycin and INH based treatment centralized at district level.
Based on a review of the NTP, and WHO recommendations of the DOTS Strategy, Government of India then revised the NTP and launched new program with the title Revised National Tuberculosis Control Program (RNTCP) in 1997. It used Sputum microscopy at DMC(Designated Microscopy Centres) for diagnosis, and multi-drug Short Course Anti-TB Therapy, decentralized to the TU (TB Unit) level.
In recognition of the rising drug resistance problem the DOTS Plus/ PMDT (Programmatic Management of Drug Resistant TB) was launched in 2006 and scaled up to the entire country by 2012.
Further to strengthen the monitoring and supervision system - a case based notification system - Nikshay was introduced in 2012. The same year Tuberculosis was added as a notifiable disease at the point of diagnosis by all health care providers.
Other key milestones from 2012 to 2020 were the availability of the Standards of TB Care in India (STCI) in 2014, introduction of the Daily weight band wise Fixed Dose combination (FDC) in 2016 and new drugs like Bedaquilline and Delaminid were started in 2017 and 2018 respectively.
To emphasise the commitment of the Government of India and to accelerate the efforts towards TB elimination, RNTCP was renamed as "National Tuberculosis Elimination Programme (NTEP)" in 2020.
Figure: Key milestones under NTEP
Resources:
India's commitment to End TB
ContentThe Government of India has committed to achieving the Sustainable Development Goals(SDG) targets related to ending TB by 2025 (5 years ahead of the global target). This would mean that in 2025, the 2030 target of achieving 80% reduction in incidence, 90% reduction in deaths due to TB compared to that of 2015, is to be achieved.
Parameter 2015 Value SDG 2030 Target Commitment for 2025 Estimated annual Incidence 217 cases/Lakh 80% reduction 44 cases/lakh Estimated annual Mortality 4.5 lakh 90% reduction 45,000 Table: India's commitment to End TB by 2025.
Resources:
National Strategic Plan [NSP] for TB Elimination 2017-25
ContentThe National Strategic Plan (NSP) for TB elimination 2017–25 is a bold strategic framework to drive the acceleration of progress toward TB Elimination, and achieving the Sustainable Development Goal (SDG) and End TB targets for India. It expects to guide the activities of all stakeholders including the national and state governments, development partners, civil society organizations, international agencies, research institutions, private sector, and many others whose work is relevant to TB elimination in India. It is adopts strategies under four groups DETECT, TREAT, PREVENT, BUILD.
VISION: TB-Free India with zero deaths, disease and poverty due to tuberculosis
GOAL: To achieve a rapid decline in burden of TB, morbidity and mortality while working towards elimination of TB in India by 2025.The results framework of the NSP outlines the various targets (impact and outcomes) to be achieved.
IMPACT INDICATORS 2015
(Baseline)2020 2023 2025 1. To reduce estimated TB Incidence rate (per 100,000) 217
(112-355)142
(76-255)77
(49-185)44
(36-158)2. To reduce estimated TB prevalence rate (per 100,000)
320
(280-380)170
(159-217)90
(81-125)65
(56-93)3. To reduce estimated mortality due to TB (per 100,000)
32 (29-35) 15 (13-16) 6 (5-7) 3 (3-4) 4. To achieve zero catastrophic cost for affected families due to TB 35% 0% 0% 0% Resources
Assessment Questions
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct Answer Explanation Part of pre-test Part of post-test Which are the groups under which strategies for National Strategic Plan (NSP) for TB elimination 2017–25 were developed? DETECT, TREAT, PREVENT DETECT, TREAT, PREVENT, BUILD DETECT, TREAT, PREVENT, REHABILITATE DETECT, TREAT, REHABILITATE DETECT, TREAT, PREVENT, BUILD The National Strategic Plan (NSP) for TB elimination 2017–25 adopts strategies under four groups: DETECT, TREAT, PREVENT, BUILD. Yes Yes Which of the following does the National Strategic Plan (NSP) for TB elimination 2017–25 aim to bring down to 0% by 2025? Incidence rate Prevalence rate Mortality rate Catastrophic cost for affected families Catastrophic cost for affected families The target of the National Strategic Plan (NSP) for TB elimination 2017–25 is to achieve zero catastrophic cost for affected families due to TB Yes Yes NTEP Objectives- in relation to NSP 2017-2025
ContentNSP 2012 - 2017 had the aim of achieving universal access to quality diagnosis and treatment. The NSP 2017-2025 which builds on the success and learnings of the last NSP, and articulates the bold and innovative steps required to move towards TB elimination. In 2020, RNTCP was renamed to "National Tuberculosis Elimination Programme" with the following objectives:

Figure: Objectives of NTEP
Resources:
Organizational Structure of NTEP
ContentNational Tuberculosis Elimination Programme (NTEP) is a centrally sponsored programme being implemented under the aegis of National Health Mission.
National Level: Managed by Central TB Division (CTD), the technical arm of the Ministry of Health and Family Welfare (MOHFW)
State Level: State TB Cell coordinates the overall TB elimination programme in state under the guidance of State Health Society. The training ,supervision, monitoring and evaluation NTEP at state level are looked after by STDC (State TB Training and Demonstration Centre).
District TB Centre (DTC) is the nodal point for all TB elimination activities in the district under the guidance of the District Health Society.
Tuberculosis Unit (TU) Level: NTEP activities at block/sub-district level are implemented through TU which comprises Designated Medical Officer (MO) supported by two full-time NTEP staff - STS (Senior Treatment Supervisor) & STLS (Senior TB Lab Supervisor).
PHI (Peripheral Health Institute): PHI is a health facility manned by a Medical Officer (MO). Some of the PHIs are also the Tuberculosis Diagnostic Centres, which are the most peripheral level laboratories in the NTEP structure. All the Private Health Facilities like Private Practitioners / Private Hospitals / Clinics / Nursing Homes are also PHI.

Figure: Organisational structure of NTEP
Resources:
The State TB Cell
ContentThe State TB Cell or STC is the state-level implementing structure of the National TB Elimination Program (NTEP). It is the leading institution for management of NTEP activities at the state level.
The STC is a State Government entity that acts as the bridge between the Central and State Governments for implementing the NTEP. It works under the guidance of the Central TB Division (CTD), and it oversees the program implementation at the districts.
- The State TB Cell is supported by the State TB Training and Demonstration Centre (STDC) for its technical functionalities. STDC mainly supports training, supervision and monitoring.
- The nodal laboratory for the State is the Intermediate Reference Laboratory (IRL). This supports quality assurance of the smear microscopy network and laboratory services in the state.
- The STC has a fully operational State Drug Store (SDS) which is responsible for the effective management and uninterrupted supply of good-quality of medicines and other logistics.
Human Resources at the State TB Cell are:
- State Tuberculosis Officer (STO). A dedicated official from the state health system, at the rank of a Joint Director is designated as the STO and heads the implementation of the NTEP at state level.
- Medical Officer STC (MO-STC): A medical officer from the state health system assists the STO in overseeing various activities.
- State DRTB Coordinator: Assist the STO in DRTB activities monitoring across the districts
- TB - HIV Coordinator: Assist the STO in overseeing TB comorbidities across the district.
- State PPM Coordinator: Looks at the private sector engagement
- State IEC Officer/ACSM Officer: Oversees the implementation of advocacy, communication and social mobilisation activities across different districts.
- STC - Epidemiologist: Assist the STO and STDC Directors by analyzing state-level data and preparing review materials
- Other support staff at the STC include
- Accounts Officer
- Technical Officer-PSM
- Secretarial Assistant
- Data entry operators/Nikshay operator
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Training Modules (5-9) for Programme Managers and Medical Officers, 2020.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following statements are true about the State TB Cell (STC)? STC is a state government entity. It is the leading institution for the management of NTEP activities at the state level. It is supported by the STDC. All of the above 4 The STC is a state government entity that is the leading institution for the management of NTEP activities at the state level and is supported by the STDC. Yes Yes State TB Training and Demonstration Centre [STDC]
ContentThe State Tuberculosis (TB) Cell (STC) is supported by the State TB Training and Demonstration Centre (STDC) in many states through its three units – Training Unit, Supervision and Monitoring Unit and an Intermediate Reference Laboratory (IRL). This relationship is shown in the figure below.
- Training Unit: It is involved in estimating the training load, organizing state level training (Induction and Refresher) and evaluating the performance of those who undergo training.
- Supervision and Monitoring Unit: It consists of a team which is dedicated to the supervision of TB elimination activities through supervisory visits, periodic desk review of Nikshay and Nikshay Aushadhi data, and plans state internal evaluations apart from assisting in other supervision and monitoring activities of National Reference Laboratories, Central TB Division and other national/international monitoring missions.
- Intermediate Reference Laboratory: This supports an effective quality assurance system of the sputum smear microscopy network and laboratory services for the programmatic management of drug-resistant TB (molecular drug resistance and culture and drug susceptibility testing) in the state.
The STDC is also involved in operational research.
Human Resources in the STDC
- The STDC functions under the leadership of STDC Director.
Training and Supervision & Monitoring Units:
- 1 Epidemiologist
- 1/more Medical Officer
- 1 Nikshay Operator
- 1 Secretarial Assistant
Intermediate Reference Laboratory (IRL):
- 1 Microbiologist
- 1 Microbiologist- External Quality Assistance (EQA)
- 1 Senior Laboratory Technician- EQA
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Training Modules (5-9) for Programme Managers and Medical Officers, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
District TB Centre [DTC]
ContentThe key level for the management of public health services is the district level. The District Tuberculosis Centre (DTC) is the nodal point for tuberculosis (TB) control activities in the district.
Functions of the DTC
The primary role of the DTC is a managerial one. The DTC is the central program management unit of the district responsible for all activities related to National TB Elimination Programme (NTEP) implementation such as:
- Advocacy
- Active case finding
- Diagnosis, treatment (both for drug-susceptible and drug-resistant TB cases) and follow up
- Managing comorbidities
- Service delivery
- Maintaining diagnostic and treatment infrastructure
- Setting up Drug-resistant TB (DR-TB) centres
- Ensuring community engagement and TB forums
- Multi-sectorial involvement for drug management, and supervision and monitoring
- Financial management
- Drugs, logistics and supply chain management.
Components of the DTC
- District Drug Store (DDS)
- Nucleic Acid Amplification Test machine (Cartridge Based NAAT or TrueNAT)
- Designated Microscopic Center (DMC)
- Treatment Support Center
- Drug Resistant TB (DR-TB) Center
- X-Ray Unit
With expansion of TB services and ongoing collaboration with various national programs, the structure of DTC is highly integrated as part of general health system and some components may cater to non-TB patients as well e.g., the DMC may be a part of general laboratory, and X-ray unit can be functional for all departments and not just chest/TB section.
Human Resources Deployed at the DTC
The Chief District Health Officer (CDHO) / Chief District Medical Officer (CDMO) / Civil Surgeon or an equivalent functionary in the district is responsible for all medical and public health activities including control of TB.
A full-time District TB Officer (DTO), trained at the national level and based at the DTC, is responsible for planning, training, supervising and monitoring the programme in the district. The DTO is assisted by other technical and secretarial staff:
- Medical Officer- District TB Center
- District DR-TB-HIV Coordinator
- District Public Private Mix Coordinator
- District Program Coordinator
- District Drug Store Pharmacist
- District Data Entry Operator-Nikshay
- District Accountant
- Senior TB laboratory Supervisor
- Senior Treatment Supervisor
- Laboratory Technicians for DMC and NAAT site
- Counsellor for District DR-TB center
- TB Health Visitors
While the National TB Elimination Program (NTEP) approves the above positions through National Health Mission NTEP Project Implementation Plan, the district always has the flexibility for additional resource deployment based on the need and existing epidemic. The DTO and his/her team are supported by various other program officers/staff and non-governmental organizations working in the field for Tuberculosis and Health.
Resources
- NTEP Training Modules 1-4 for Programme Managers & Medical Officers, 2020.
- NTEP Training Modules 5-9 for Programme Managers & Medical Officers, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Tuberculosis Unit [TU]
ContentTuberculosis (TB) unit (TU) is the sub-district level supervisory unit of National TB Elimination Program with the following organogram:
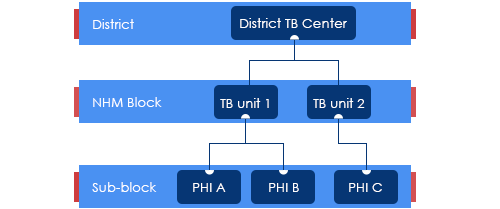
Figure: Organogram of a TB Unit
(PHI: Peripheral Health Institution)
TUs are based mainly on National Health Mission (NHM) health blocks with the aim of aligning with the NHM Block Programme Management Unit (BPMU) for optimum resource utilization and appropriate monitoring.
The TUs have been created based on a population of 1 per 2,00,000 (range 1.5 – 2.5 lakh) for rural and urban populations and 1 per 1,00,000 (0.75 – 1.25 lakh) population in hilly/tribal/difficult areas.
The TU consists of a designated Medical Officer-Tuberculosis Control (MO-TC), as well as one full-time supervisory staff - Senior Treatment Supervisor (STS). However, one Senior TB Laboratory Supervisor (STLS) will be there in every 5 lakh population (one per 2.5 lakh population for tribal/hilly/difficult areas), mostly covering 2-3 TUs.
TB Unit manages the provision of TB services (Diagnosis, Treatment, Prevention, etc.) and programme management in the assigned geographical area.
Resources
Peripheral Health Institutions [PHI] and Health Facilities
ContentUnder the National Tuberculosis Elimination Programme (NTEP), a Peripheral Health Institute (PHI) is a health facility that is manned by at least a Medical Officer (MO), where diagnosis and management of Tuberculosis (TB) are done.
At this level, there are dispensaries, Primary Health Centres (PHCs), Community Health Centres (CHCs), referral hospitals, major hospitals, speciality clinics or hospitals (including other health facilities), TB hospitals, Anti-retroviral Treatment (ART) centres and medical colleges within the respective district.
All health facilities in the private and Non-government Organisation (NGO) sectors participating in NTEP are also considered PHIs. Some of these PHIs also function as Designated Microscopy Centres (DMCs).
Role of PHIs in Program Management for TB Elimination
- PHIs undertake tuberculosis case-finding and treatment activities as a part of the general health services.
- In situations where more than one MO is posted in any of the PHC, one of them may be identified and entrusted with the responsibilities of the NTEP.
- Additionally, NTEP provides 1 TB Health Visitor (TBHV) per one lakh urban population to support the urban TB control activities in urban settings/ medical colleges.
Resources
DR-TB Centres and Network
ContentDrug-resistant Tuberculosis Centres (DR-TBCs) are specialized centres for the clinical management of Drug-resistant TB (DR-TB).
Each DR-TBC needs to have established a DR-TB committee to carry out the clinical management of DR-TB patients.
DR-TBCs can be established in the public sector where appropriate facilities are available.
- The DR-TBC can also be established in the private sector on mutually agreeable terms and conditions based on the Guidance Document on Partnerships, 2019.
District level: There are District Drug-resistant TB Centres (DDR-TBCs) to manage DR-TB cases. These centres will function under the guidance of Nodal Drug-resistant TB Centres (NDR-TBCs). Almost every district has a mandate to establish a DDR-TBC in India. There are around 620 DDR-TBCs established in the country.
State/ Regional level: At the state/ regional/ division level, there are NDR-TBCs to manage seriously ill DR-TB cases. There are 173 NDR-TBCs established in India.
Decentralized DR-TB services through an expanded network of DR-TB centres has helped the National TB Elimination Program in improving access to DR-TB services and has also resulted in improved DR-TB treatment linkage and better management of DR-TB patients.
Resources
Standards of TB Care in India
ContentThe Standards for TB Care in India (STCI), which is a locally customized version of the International Standards of Tuberculosis Care, mentions 26 standards that every citizen of India should receive irrespective of the sector of treatment.
STCI were developed based on a series of discussions involving various stakeholders including clinicians, public health specialists, community workers and patient advocates.
STCI represent what is expected for quality TB care from the Indian healthcare system including both public and private systems.
It was first published in 2014 and outlines standards across the four themes of TB diagnosis, TB treatment, public health action and social inclusion.
Following are the list of the 26 Standards:

Table 1: Categorisation of the Standards for TB Care in India, Source: Standards for TB Care in India, World Health Organisation, pp. 13-23
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test How many standards in TB care are described in the Standards of TB Care in India (STCI) 2014? 4 15 26 32 3 There are 26 standards for TB care under four major categories: diagnosis, treatment, public health actions and social inclusion. Yes Yes Stages in TB Patient's Lifecycle
ContentThose who are suspected of having TB disease are first screened for symptoms like cough and fever for more than 2 weeks, blood stained sputum and weight-loss. If found positive on screening, then TB patients are referred for testing to the nearest health facility. If diagnosed with TB, then they are subsequently initiated on treatment. The TB patients initiated on treatment are regularly monitored with the help of field staff or digital interventions like 99DOTS and MERM (Medication Event Reminder Monitor) technology. NTEP staff also ensures that the TB patients are regularly followed up on monthly basis till their treatment completion.
Figure: Patient Flow
Kindly provide your valuable feedback on the page to the link provided HERE
-
IEC-CH3: Diagnostic Technologies
FullscreenScreening For Tuberculosis Disease
ContentScreening for active tuberculosis (TB) a process to filter out people who are less likely to have TB, from a group. Screened positive people are likely to have TB and are confirmed subsequently using a TB diagnostic test. This will allow finite diagnostic testing resources to be used on the remaining.
Screening in TB may be performed using simple field tools (4 Symptom complex) and tests such as Chest X-ray, or a combination of both. Combination of both is the most effective, but is often not applied due to the practical difficulties in making a chest X-ray conveniently available.
Screening is an integral part of any general case finding effort. It is also applied systematically in specific situations.
- At health care facilities (intensified case finding): Here those visiting are screened using the 4 symptom complex, often at the point of entry to the facility. Those screened positive may be fast-tracked to TB Diagnostic testing.
- In vulnerable populations in active case finding efforts: Here the entire population identified for active case finding are screened using the pre-decided protocols by going door to door.
Resources
Approaches to TB Case Finding
ContentPeople who have been exposed to patients with infectious TB are known as TB contacts; they constitute a high-risk group for TB. Case finding investigation contributes to the early detection of TB cases, and results in identifying a significant number of additional patients.
Figure: Approaches to Tuberculosis Case Finding
Active case-finding requires systematic screening and clinical evaluation of populations who are at high risk of developing TB, such as people living in slums, tribal areas, congregate settings, persons who are household contacts of TB cases
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Active Case Finding
ContentSystematic screening of all individuals of a defined population is known as active case finding. It is applied outside of health facilities at the community level by the health system.
Objective of ACF is to:
- identify cases early, initiate prompt treatment, reduce risk of poor treatment outcomes and reduce risk of further transmission of TB
- to provide access to diagnosis services to populations that would have been otherwise unreached
It is effort intensive and is recommended only in population groups where there is estimated high case load. In NTEP, ACF is recommended only to be performed in Key / vulnerable population.
ACF can also be clubbed with suitable ACSM campaigns to create awareness about the signs and symptoms and about TB in the target population/ community. It can also be combined with other health activities/ campaigns (such as Pulse Polio/ Leprosy screening/ population based screening for NCDs) for increased efficiency.
Resources
- Training Modules for Programme Managers and Medical Officers.
- Active TB Case Finding, Guidance Document.
- WHO recommendations for Systematic Screening for Active Tuberculosis
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following is not a primary objective of ACF? Increase TB notification Early identification of cases. Reduce the risk of transmission of TB. Reduce the risk of poor treatment outcomes. 1 Notification is not a primary objective of ACF. Yes Yes Classification of TB on the basis of Drug Resistance
ContentResistant Sensitive Unknown / Sensitive Types of Drug Resistance TB (DR TB) Resistant to Isoniazid (H) Rifampicin (R) Fluroquinolones (FQ) =
Ofloxacin, Levofloxacin,
MoxifloxacinGroup A Drugs =
Bedaquiline/ LinezolidH Mono / Poly Drug Resistance Resistant Sensitive Unknown/ Sensitive Unknown/ Sensitive Rifampicin Resistance (RR) Unknown/ Sensitive Resistant Unknown/ Sensitive Unknown/ Sensitive Multi Drug Resistance TB (MDR TB Resistant Resistant Unknown/ Sensitive Unknown/ Sensitive Pre-Extensive Drug Resistance (Pre -XDR) Resistant Resistant Resistant Unknown/ Sensitive Extensive Drug Resistance (XDR) Resistant
Resistant Resistant Resistant Resources:
-
IEC-CH4: TB Case Finding in NTEP
FullscreenClassification of TB cases based on history of Previous TB treatment
Content- New case - A TB patient who has never had treatment for TB or has taken anti-TB drugs for less than one month is considered as a new case.
- Previously treated patients have received 1 month or more of anti-TB drugs in the past. They could be further classified as:
- Recurrent TB case - A TB patient previously declared as successfully treated(cured/treatment completed) and is subsequently found to be microbiologically confirmed TB case is a recurrent TB case.
- Treatment After failure patients are those who have previously been treated for TB and whose treatment failed at the end of their most recent course of treatment.
- Treatment after loss to follow-up A TB patient previously treated for TB for 1 month or more and was declared lost to follow-up in their most recent course of treatment and subsequently found microbiologically confirmed TB case
- Other previously treated patients are those who have previously been treated for TB but whose outcome after their most recent course of treatment is unknown or undocumented.
- Transferred In: A TB patient who is received for treatment in a Tuberculosis Unit, after registered for treatment in another TB unit is considered as a case of transfer in.
- Transferred Out : A patient who has been transferred to another recording and reporting unit and whose treatment outcome is unknown.
Classification of TB on the basis of diagnosis
ContentOn the basis of diagnosis, Tuberculosis (TB) can be classified into 2 main types:
- Microbiologically confirmed TB
- Clinically diagnosed TB
Microbiologically Confirmed TB
- Microbiologically confirmed TB refers to a presumptive TB case from which a biological specimen is positive for acid-fast bacilli/ Mycobacterium tuberculosis on smear microscopy, culture, or on a rapid diagnostic molecular test (such as Cartridge-based Nucleic Acid Amplification Test (CBNAAT)/ Truenat).
- All such diagnosed cases should be notified at the source, regardless of whether TB treatment has started.
Clinically Diagnosed TB
- Clinically diagnosed TB refers to a presumptive TB case that is not microbiologically confirmed but has been diagnosed with active TB by a clinician who has decided to give the patient a full course of anti-TB treatment.
- This definition includes cases diagnosed on the basis of X-ray abnormalities or suggestive histology or extrapulmonary cases without laboratory confirmation.
- Clinically diagnosed cases subsequently found to be microbiologically positive (before or after starting treatment) should be reclassified as microbiologically confirmed.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Definitions and Reporting Framework for Tuberculosis, WHO, 2013.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test TB is classified on the basis of diagnosis into which of the following? Microbiologically confirmed TB and clinically diagnosed TB Mono-resistant TB and poly-resistant TB Recurrent cases and previously treated cases None of the above 1 TB can be classified on the basis of diagnosis into 2 main types: Microbiologically confirmed TB and Clinically diagnosed TB.
-
-
IEC-M2: Treatment Support and Monitoring of TB patient
Fullscreen-
IEC-CH6: DSTB Treatment and Care
FullscreenDS-TB Treatment – Patient Flow
ContentCommunity Health Volunteers(CHVs) have to refer the presumptive cases identified based on the r symptom screening to the nearest NTEP health facility for further investigation. Once Diagnosed with TB, the TB patients are initiated on the first-line TB treatment. Patients are also offered NAAT within a maximum of 15 days to rule out any drug resistance. If no drug resistance is detected, then the patient continues on the first-line TB treatment. TB patients are then clinically evaluated every month to check the progress of TB treatment.
The treatment duration of TB is divided into two phases - The Intensive Phase(IP) and the Continuation Phase(CP). Post-treatment completion, patients are then evaluated at intervals of 6,12,18 and 24 Months to ensure a relapse-free TB cure for the patient.
Figure: DSTB Treatment Flow
Adverse Drug Reactions(ADRs) to First Line Treatment
ContentSymptoms
Drug Responsible
Action to be taken by Community Health Volunteers
Gastrointestinal Symptoms
Any Oral Medications
-
Reassure patient.
-
Give TB Drugs with less water at a longer interval.
-
If symptom persists, refer to the nearest health facility
Itching/Rashes
Isoniazid
-
Reassure patient.
-
In case of severe itching, refer the patient to the nearest health facility
Tingling/ burning/ numbness in the hands & feet
Isoniazid
-
Refer the patient to the nearest health facility
Joint Pains
Pyrazinamide
-
Reassure patient.
-
Increase intake of liquids.
-
If severe, refer the patient to the nearest health facility
Impaired Vision
Ethambutol
-
Refer the patient to the nearest health facility
Ringing in the ears, Loss of hearing, Dizziness and loss of balance
Isoniazid, Rifampicin or Pyrazinamide
-
Refer the patient to the nearest health facility
Hepatitis: Anorexia/ nausea/ vomiting/ jaundice
Isoniazid, Ethambutol, Rifampicin or Pyrazinamide
-
If patient detected with signs of jaundice, refer the patient to the nearest health facility
-
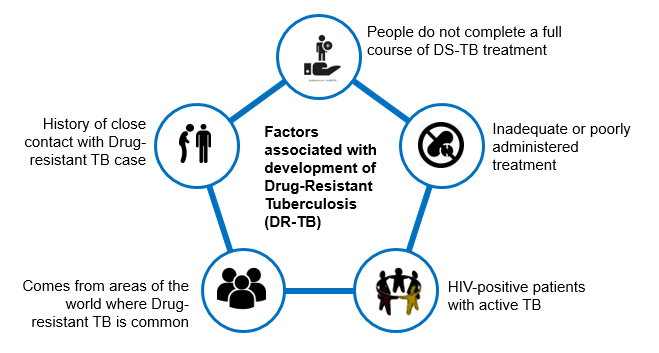
Drug-Resistant Tuberculosis(DR-TB)
ContentWhat is Drug-Resistant Tuberculosis?
-
Drug-Resistant TB occurs when bacteria become resistant to the drugs used to treat TB. This means that the drug can no longer kill the TB bacteria.
-
Multidrug-resistant TB (MDR TB) is a type of DR-TB where TB bacteria is resistant to both Isoniazid and Rifampicin, the two most potent anti-TB drugs.
Figure: High Risk for Drug-Resistant Tuberculosis (DRTB)
Resources:
-
DR-TB Treatment – Patient Flow
ContentAfter getting diagnosed with Drug-Resistant TB(DR-TB), the patient is referred to District DRTB Centre(DDR-TBC) for initiation of treatment. Few clinically complicated cases are referred to the Nodal DRTB Centre(NDR TBC). Since the drugs used for the treatment of DR-TB have significant adverse effects and to rule out any underlying comorbid conditions or radiological or ECG, or biochemical derangements, a Pre-treatment evaluation is done to check eligibility of patients for DR-TB regimen and to identify those patients requiring special attention and regimen modifications before initiating patients on TB treatment.
After initiation of treatment, patients are monitored every month. If the sputum test is positive during the follow-up, then the sputum sample is sent for further testing, and if needed, the regimen is changed. And if the sputum sample turns out to be negative during follow up sputum test, then the same treatment regimen is continued till treatment completion.
Post-treatment completion, patients are evaluated at the interval of 6, 12, 18 and 24 months, screened for any clinical signs and symptoms, and, if found suspected, then referred for sputum microscopy and /or culture test.
Figure: TB patient flow after being diagnosed with Multi Drug Resistance TB(MDR/RR TB)
-
IEC-CH7: Treatment Adherence
FullscreenTB Treatment Adherence
ContentTuberculosis(TB) is curable if patients are treated with effective, uninterrupted anti-tuberculous treatment. Treatment adherence is critical for curing individual patients, controlling the spread of infection in the community, and minimizing the development of drug resistance.
Adherence to treatment means that a patient follows the recommended course of treatment by taking all the prescribed medications for the entire length of time, as necessary. In other words, “right dose for the right duration”.
In Drug Sensitive Tuberculosis(DSTB), a TB patient completes 168 doses of TB treatment and adheres to TB treatment.
Importance of Treatment adherence
ContentAdherence to tuberculosis(TB) treatment is important for promoting individual and public health. Poor adherence to TB treatment results in:
- More individual suffering and death,
- Costly treatment as treatment regimens lengthen and
- Increases the risk for Drug Resistant Tuberculosis
Proper treatment of all forms of TB is critical to reducing individual morbidity and mortality and to interrupting transmission among family and community members.
Recording and Monitoring Adherence
ContentRecording of Treatment Adherence can be done as
- Manually by DOT/Health Care Provider in TB Treatment Card of a patient.
- Self-reported by Patient using digital tools for reporting adherence using 99 DOTS and MERM technologies.
Monitoring Treatment Adherence:
All TB patients should be monitored to assess their response to TB treatment. Nikshay Adherence calendar has a colour legend for various doses taken by a patient
Figure: Sample Nikshay Adherence Calendar in web and Mobile App
COLOUR LEGEND DOSE DESCRIPTION Treatment Start /End Denotes Treatment start and End Date Digitally Reported Dose Denotes that the patient has successfully called the Toll Free Number displayed on the envelope Manually Reported Dose Indicates that the staff has marked manually confirmed dose for the day Unreported Dose Indicates that there was no call event received on Nikshay for that day Manually Reported Missed Dose Indicates that the staff has marked a manually confirmed missed dose for the day Digitally Reported(From Shared Phone Number) Indicates that the patient has been calling from a shaed number(A mobile number that is common for more than one patient) Image
Figure: DSTB Treatment Card (Paper)
Digital Adherence Monitoring Technologies
Content99DOTS is a low-cost digital adherence technology built-in Nikshay that uses inexpensive packaging(envelopes or stickers) with medication that enables people taking medication to engage with their treatment daily. This packaging, distributed to TB patients taking medications, has a hidden number behind perforated flaps on the external envelope; in some cases, the number may be fixed outside the medication blister or pill bottle. This number can be a toll-free number that can be called to register daily adherence or a code sent by SMS, USSD, or other communication channels. Calling or messaging the number is free!
Figure: 99 DOTS Envelope
MERM: The Medication Event Reminder Monitor(MERM) is a digital pillbox that provides daily pill-taking reminders and facilitates remote monitoring of medication adherence. This system provides visual and audible reminders for both daily dosing and refill,.transmits this data to a server so that healthcare providers can remotely visualize patients’ dosing histories to support enhanced adherence counselling.
Figure: MERM Box
-
IEC-CH8: TB infection and TPT
FullscreenTB Infection
Content-
TB Infection (or previously known as Latent TB infection) is a stage in between uninfected and having active TB. In this stage the person has no symptoms and can only be identified using laboratory tests.
-
The vast majority of infected people may never develop TB disease. However, to achieve TB elimination, it is important to treat TB infection in people at risk of developing active TB disease.
-
It is a state of persistent immune response to stimulation by Mycobacterium tuberculosis antigens with no evidence of clinically manifested active TB.
-
There is no single acceptable/reliable test for direct identification of Mycobacterium tuberculosis infection in humans. Tuberculin Skin Test (TST) and Interferon-gamma release assay (IGRA) are commonly used tests for identifying TB infection.
Resources:
-
Testing for TB Infection
ContentFor TB infection, there are two recommended tests which can be used to identify such patients.
Tuberculin Skin Test (TST)
The skin test is done by injecting a small amount (0.5 ml) of TB antigens into the top layer of skin on your inner forearm. If one has ever been exposed to TB bacteria (Mycobacterium tuberculosis), there will be a reaction indicated by the development of a firm red bump (induration) >= 10 mm at the site within 2 days.
Image
Figure: Tuberculin Skin Test
Interferon-gamma release assay (IGRA)
IGRA is a Blood test. If one has been exposed to TB bacteria, the white blood cell in the blood will release a substance called gamma interferon when the cells are exposed to specific TB antigens.
Image
Figure: Interferon-gamma release assay (IGRA)
Resources:
- Latent Tuberculosis Infection Guideline
- Guideline for Programmatic Management of Tuberculosis Preventive Treatment in India
Kindly provide your valuable feedback on the page to the link provided HERE
TB Preventive Therapy
ContentTPT treatment options recommended under NTEP include:
- 3-month weekly Isoniazid and Rifapentine (3HP)
- 6-months daily isoniazid (6H)

Table 1: TPT Options for Target Population; Source: (Guidelines for Programmatic Management of Tuberculosis Preventive Treatment)

Table 2: TPT dosage based on age and weight band recommended by NTEP; Source: Guidelines for Programmatic Management of Tuberculosis Preventive Treatment
Resources
- Guidelines for Programmatic Management of Tuberculosis Preventive Treatment
- National Strategic Plan for TB Elimination
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test TPT options recommended under NTEP include which of the following? 3-month weekly Isoniazid and Rifapentine (3HP) Rifampicin 6-months daily isoniazid (6H) 1 and 3 4 TPT options recommended under NTEP include 3-month weekly Isoniazid and Rifapentine (3HP) and 6-months daily isoniazid (6H). Yes Yes
-
IEC-CH9: TB Comorbidity
FullscreenComorbidity & special situation with TB
ContentSeveral medical conditions are risk factors for TB and poor TB treatment outcomes. Similarly, TB can complicate the course of some diseases. Therefore, it is important to identify these comorbidities in people diagnosed with TB to ensure early diagnosis and improved outcomes. When these conditions are highly prevalent in the general population, they can significantly contribute to the TB burden. Consequently, reducing the prevalence of these conditions can help prevent TB.
TB shares underlying social determinants with many of these conditions. Addressing the social determinants of health is a shared responsibility across disease programmes and other stakeholders within and beyond the health sector.
Figure: Various comorbid and special situation related with tuberculosis
HIV in TB Patients
ContentThe primary impact of HIV on TB is that the risk of developing TB becomes higher in patients with HIV. Overall, HIV-infected persons have an approximately 8-times greater risk of TB than persons without HIV infection.
Screen TB PLHIV patients for symptoms of TB and HIV
Figure: Screening steps for TB - HIV patients
Treatment for TB HIV Patients
- All TB patients who have been diagnosed and registered under NTEP should be referred for screening for HIV.
- Referral of TB patients for screening for HIV and its recording & reporting is the responsibility of the Peripheral Health Institutions(PHI) where TB treatment is initiated.
- TB patients diagnosed with HIV will receive the same duration of TB treatment with daily regimen as non-HIV TB patients.
- TB patients must be referred to the nearest ART(Anti - Retroviral Treatment) centre for management of HIV.
Diabetes in TB Patients
ContentAs a consequence of urbanization as well as social and economic development, there has been a rapidly growing epidemic of Diabetes Mellitus(DM). India has the second largest number of diabetic people in the world.
Screen TB patients for symptoms of diabetes
Figure: Screening steps for TB - Diabetic Patients
Treatment for TB Diabetes Patients
- All TB patients who have been diagnosed and registered under NTEP will be referred for screening for Diabetes.
- Referral of TB patients for screening for DM and its recording & reporting is the responsibility of the Peripheral Health Institutions(PHI) where TB treatment is initiated.
- TB patients diagnosed with diabetes will receive the same duration of TB treatment with daily regimen as non-diabetic TB patients.
- TB patients must be referred to the nearest healthcare facility for management of DM.
- Regular monitoring of blood sugar levels is advised.
Malnutrition in TB Patients
ContentMalnutrition refers to deficiencies, excesses or imbalances in a person’s intake of energy and/or nutrients. The term malnutrition covers 2 broad groups of conditions.
- One is ‘undernutrition’—which includes stunting(low height for age), wasting(low weight for height), underweight(low weight for age) and micronutrient deficiencies or insufficiencies(a lack of important vitamins and minerals).
- The other is overweight, obesity and diet-related non communicable diseases (such as heart disease, stroke, diabetes, and cancer).
Screen TB Malnutrition patients for nutritional needs
Figure: Screening Steps for TB - Malnutrition patients
Treatment for TB Malnutrition Patients
Cases of TB with SAM and moderate undernutrition should be referred to the nearest health facility of NTEP for further management. Special focus should be given to the following categories:
- Children below five years
- School-age children and adolescents(Up to age 18 years)
- Adults, including pregnant and lactating women, with active TB and SAM
Alcoholism in TB Patients
ContentAbout 10% TB deaths globally have been attributed to alcohol as a risk factor(WHO, Global TB Report 2017). Alcohol abuse is associated with threefold increase in risk of contracting tuberculosis.
Side effects of anti TB drugs in this situation might get aggravated.
Figure: Impact of Alcoholism on TB patients
Treatment for Alcoholic TB Patients:
- Patients with TB and a history of alcohol use should be referred to the nearest health facility of NTEP to manage TB and alcoholism.
- While registering as a TB case, the status of alcohol use should be recorded in the patient records. If the TB patient is an alcohol user, he/she should be counselled to quit it. If the patient doesn't quit alcohol, s/he may be referred to the nearest alcohol de-addiction facility.
- The patient should be assessed at every follow-up visit for TB and the status of use of alcohol.
- At the end of treatment, his/her status of alcohol use should be recorded on the treatment card. If the patient has not quit alcohol, he/she should be referred to the nearest alcohol de-addiction facility and Alcohol Anonymous wherever available.
Tobacco in TB Patients
ContentAlmost 38% of TB deaths are associated with the use of tobacco. The prevalence of TB is three times higher among ever-smokers as compared to that of never-smokers. Mortality from TB is three to four times higher among ever-smokers as compared to never-smokers. Smoking contributes to 50% of male deaths in the 25-69 age group from TB in India.
Figure: Impact of Tobacco on TB patients
Treatment for TB - Tobacco Patients:
- While registering as a TB case, the status of tobacco use is recorded on the TB treatment card.
- If the TB patient is a smoker or tobacco user, he/she is counselled to quit tobacco use. The patient is assessed at every visit for follow up for TB and the status of tobacco use.
- At the end of treatment, his/her status of tobacco use is recorded in the treatment card. If the patient has not quit tobacco use, he/she will be referred to the nearest Tobacco Cessation Clinic(TCC) or Quit Line or M-Cessation Initiative.
Pregnancy and Lactation in TB Patients
ContentThe presence of tuberculosis disease during pregnancy, delivery, and postpartum is known to result in unfavourable outcomes for both pregnant women and their infants. These outcomes include a roughly two-fold increased risk of preterm birth, low birth weight, intrauterine growth restriction, and a six-fold increase in perinatal death.
Screen TB patients in Pregnancy & Lactating Patients
Figure: Screening Steps in special situation - Pregnancy and Lactating TB Patients
Treatment for TB - Pregnant & Lactating Patients
- Cases of pregnant/lactating women with active TB should be referred to the nearest health facility of NTEP for further management.
- They should be continued on iron and folic acid and other vitamins and minerals to complement their maternal micronutrient needs.
- In situations when calcium intake is low, calcium supplementation is recommended as part of antenatal care.
COVID-19 in TB patients
ContentTuberculosis and COVID-19 are infectious diseases which primarily attack the lungs. They present with similar symptoms of cough, fever and difficulty in breathing, although TB disease has a longer incubation period and a slower onset of disease.
Screen patients for symptoms of TB and COVID-19
Figure: Screening steps for TB - COVID 19 Patients
Management of TB & COVID-19 Patients
People with TB are likely to be at increased risk of COVID-19 infection, illness and death. So, TB patients should take precautions as advised by health authorities to be protected from COVID-19 and continue their TB treatment as prescribed.
Prevention: While both TB and COVID-19 are spread by close contact between people, the exact mode of transmission differs. Thus, the patient should be explained the following measures to control disease spread.
- Apart from that keeping rooms well ventilated, avoiding crowds and Respiratory precautions are thus important in the control of COVID-19 and TB Disease
-
-
IEC-M3: Patient Support
Fullscreen-
IEC-CH10: Counselling
FullscreenTB Awareness Generation in Community
ContentAwareness should be generated in the community for promoting various health programmes, health seeking behaviours, screening of TB cases etc. by involving and sensitizing community influencers including PRI members and treatment support groups.
Figure: Activities for awareness generation in community
Counselling of TB Patients
ContentConfidential dialogue between a health care provider and a patient that helps a patient to define his/her feelings, cope with stress, and to make informed decisions regarding treatment.
The patient should be counselled at all the three phases i.e.,
Pre-treatment counselling`
- About TB disease and treatment
- Air borne infection control
- Need for adherence
- Public Health Actions
- Identification of adverse events
- Tobacco /Alcohol cessations
- Identification of comorbidities
During Treatment Counselling
- Importance of Adherence
- Identification of adverse events
- Importance of timely follow ups
- Public Health Actions
- Tobacco /Alcohol cessations
- Management of comorbidities
Post treatment Counselling
- Testing at the end of treatment.
- Long term follow up
- Tobacco /Alcohol cessations
Objectives of TB Counselling:
- Prevention of TB transmission.
- Provision of emotional support to TB patients.
- Motivation of TB clients to complete treatment.
- Helping patients make their own informed decisions about their behaviour and supporting them in carrying out their decisions.
Figure: Characteristics of effective counselling
Do's & Don'ts for Patient Communication
ContentDo’s
- Active listening, emphatic gestures and expressions
- Ensure the confidentiality of the conversation done with the patient
- Ensure Minimum interruption during the conversation with patient
- Ensuring availability of IEC materials such as posters, videos, pamphlets etc. to dispel myths and misconceptions.
Don'ts
- Do not use any negative stereotypes
- Do not have any physical wall or glass between patient and yourself
- Do not breach the trust and confidentiality of the TB patient
- Do not make threats or use coercive language
- Do not exaggerate dangers or risk of TB
- Do not blame or shame TB patients
Nutritional Counselling
ContentNutritional Counselling begins with the nutritional assessment of TB patients by
-
Nutritional Status: Assessing the height, weight and BMI of the TB patient
-
Diet and Preference food for TB patients
-
Current appetite and food intake of TB patients
Based on the nutritional assessment, following information can be conveyed to TB Patients
-
Patients with TB should be encouraged to have frequent food intake in the form of three meals and three snacks.
-
Attempts should be made to increase the energy and protein content in the meals and snacks without increasing its volume.
-
The addition of oil, butter or ghee to the chapati or rice can increase the energy content of the diet.
-
Pulses in other forms, e.g. sprouts, roasted Chana, groundnuts, can be taken as snacks in either fried or in roasted form. Milk and eggs to be included in the diet.
-
The use of easily available nutritious foods based on vegetarian/non-vegetarian preferences of the patients must be emphasized.
-
Information about NFSA (National Food Security Act) and Poshan abhiyan should be given.
Figure: Healthy diet for TB Patients
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
-
-
IEC-CH11: Social Inclusion and Wellness activity
FullscreenDeterminants of TB Disease
ContentDeterminants are any characteristics that affect the health of a patient.
Biological Determinants Behavioral Determinants Socio Economic Determinants Occupational Determinants - People living with HIV(PL HIV)
- History of contact with a case of TB
- People with underlying medical conditions like Diabetes, Kidney disease, Cancer etc.
- Existing lung disease
- Old age
- Use of tobacco and alcohol
- Malnutrition
- Person in contact with TB infected patient
- Person living in areas with poor ventilation & over crowding
- Poverty and Malnutrition
- Homeless
- Mining work
- Quarry work(Silicosis)
- Construction work
- Migrant worker
- Daily wagers
Socio-Economic Determinants for Tuberculosis
ContentSocioeconomic determinants of health include the conditions in which people are born, grow, live, work, and age. These determinants play an important role in increasing the risk of acquiring TB infection, its progression into active TB disease and further transmission to contacts.
Socio-economic factors affect health-seeking behaviour and access to TB services
Figure: Socioeconomic factors that are affecting the health of TB patients
There may be difficulties in transportation to health facilities and lack of social support to seek care when they fall sick. This delays the contact with health systems for appropriate diagnosis and initiation of treatment.
Socio economic factors affecting TB patients
ContentSocio-economic factors affecting TB patients are:
1. General socioeconomic conditions of the society, culture and environment. This includes:
-
Gross Domestic Product (GDP)
-
Immigration
-
Urbanisation
-
Incidence of TB in the country
-
Labour policy
-
Access to healthcare
2. Socioeconomic position of the individual. This includes:
-
Income
-
Education
-
Occupation
-
Social class/ caste
-
Indigenous/ tribal population
-
Gender
3. Living and working conditions. This includes:
-
Housing conditions (overcrowding and poor ventilation especially in night shelters, de-addiction centres, old age homes, prisons)
-
Employment conditions - Occupation with risk of developing TB (mines, coal industry, sand blasting industries, weaving & glass industries, stone-crushers, cotton mill workers, tea garden workers, rice mill workers, etc.,)
-
Homelessness
-
Hard to reach areas
-
Urban slums
3. Psychosocial risk factors, such as:
-
Social exclusion
-
Depression
4. Individual lifestyle risk factors, such as:
-
Smoking
-
Alcohol abuse
-
Tobbaco use
-
Drug abuse
-
Nutrition (malnutrition)
-
Co-morbidities like diabetes mellitus, malignancies, patients on dialysis and on long term immunosuppressant therapy HIV, past history of TB
Resources
- NTEP Training Modules (1 to 4) for Programme Managers & Medical Officers, CTD, 2020.
- Social Determinants of Tuberculosis Context Framework and the Way Forward to Ending TB in India, IPH, India, 2020.
Assessment
Question
Answer
1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Socio-economic factors affecting TB patients are:
-
Housing
-
Income
-
Access to healthcare
-
Alcohol abuse
1,2
2,3,4
1,2,3,4
1,2,4
3
TB is one of the few diseases which reflects and expresses social inequalities. Living conditions, economic conditions, lifestyle, and access, affordability, and availability of healthcare are factors which affect TB patients.
-
Vulnerable Population for Tuberculosis
ContentTB can affect anyone but it is more prevalent in some communities which are vulnerable to TB disease due to various factors which are mentioned below:
Increased exposure of TB due to where they live or work
- prisoners
- slum dwellers
- miners
- hospital visitors
- healthcare workers
Limited access to Quality TB services
- Migrant workers
- Women in settings with gender disparity,
- Children
- Physically challenged
- Transgender population
- Tribal and population living in hard to reach areas
- Refugees or internally displaced people
- Illegal miners and undocumented migrants
Increased risk because of biological or behavioural factors that compromise immune functions in people who:
- People who live with HIV
- have diabetes or silicosis
- undergo immunosuppressive therapy
- are undernourished
- use tobacco
- suffer from alcohol use disorders.
- inject drugs
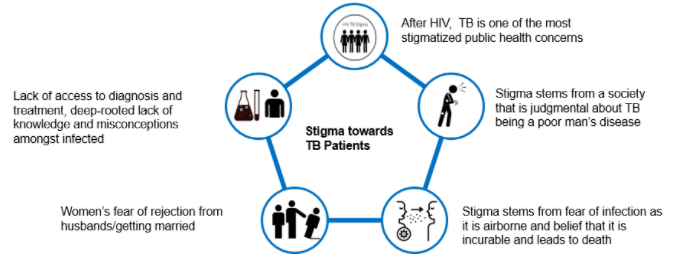
Stigma and Discrimination towards TB Patient
ContentStigma is when someone sees you in a negative way.
Discrimination is when someone treats you in a negative way.
TB patients face various forms of stigma and discrimination in the community
Figure: Stigma towards TB Patients in the community
Effects of Stigma on TB Patients
ContentAt Individual Level
- Lack of self-esteem and confidence
- Increased sense of emotional isolation, feeling of guilt and anxiety
- Physical as well as financial debilitation
- People, more often women, are forced to leave their homes
- Concealing symptoms and hesitancy in seeking medical care making disease management more difficult
- Delayed diagnosis, interrupted treatment that can lead to further transmission and DRTB
- Vulnerability increases, can lead to suicidal thoughts due to isolation and shame
At Family and Community Levels
- Loss of household earnings
- Exposure of caregivers to the risk of infection that lowers productivity and cycle of poverty further gets perpetuated
- Isolation and stigmatization of infected persons often by people of their community
- Deep-rooted lack of knowledge and misconceptions among the affected and infected within their cultural and religious environment
- Loss of status and negative impact on those with the disease, their caregivers, family, friends and communities
- Perceived and internalized stigma of the community due to socio-cultural values that TB is punishment for sins or transgression
Gender Aspects of TB
ContentAlthough more men are affected by TB, women and transgender persons experience the disease differently. Gender differences and inequalities play a significant role in how people of all gender access and receive healthcare services.
Gender difference in Men Women Incidence of TB - Higher proportion of men(approximately- 2:1) are diagnosed with TB than women
- More likely to have microbiologically confirmed Pulmonary TB
- More likely to have Clinically diagnosed pulmonary TB and extra – pulmonary forms of TB
- Prevalence of HIV-TB co-infection is higher among women who live in overcrowded houses and consume alcohol
- High Risk for developing TB – Pregnant women and women in the postpartum period
Exposure, Risk & Vulnerability - Smoking and alcohol consumption among men
- High risk for developing TB - employment in mining, quarrying, metals and construction industries
Undernutrition, their role as caretakers and the use of solid fuel for cooking puts women at risk for TB Health Seeking & Health system factors - Fear of loss of income and the consequences of absence from work hinder care seeking.
- Women face difficulties due to perceived stigma, prioritization of household chores, lack of money or financial dependence
Treatment Outcomes - Pressure to get back to work and lifestyle habits such as smoking or consumption of alcohol influence discontinuation of treatment in men
- Migrant workers, mostly men, often face difficulties in adherence to treatment in the face of extreme poverty and issues of daily survival
- Women tend to have better adherence and treatment outcome as compared to men
- Stigma and discrimination are major impediments to treatment adherence, mainly among unmarried women, newly married women and the elderly
Transgender population often has low literacy, low education levels and are poor. A high proportion of transgender persons are known to smoke, consume alcohol and use drugs. All these factors make them vulnerable to TB.
Addressing Gender Inequalities
ContentBroad principles to address gender inequalities in TB care
- Confidentiality of patient needs to be maintained
- Non-discrimination and non-stigmatising behaviour to be promoted
- Respect for all to be ensured
- Informed consent and informed treatment
- Accountability to be fixed for actions and inactions
- Access for all health services
- Rights-based approach
- Empowered communities - Ensure representation of women, men and transgender persons in all forums
- Work in partnership - Strengthen linkages between program, private sector and communities
Wellness Activity for TB Patients
ContentYoga
- Yoga aims at holistic functioning of the mind and body. It consists of various exercises and specific body positions and movements(yoga asana) which can be learnt and performed under the supervision of a yoga teacher.
- Yoga will help to clean the upper respiratory tract and the sinuses. The breathing exercise or pranayama induce relaxation and help to reduce the stress levels of the patients considerably.
Meditation
- Meditation is a practice where an individual uses a technique – such as mindfulness, or focusing the mind on a particular object, thought, or activity – to train attention and awareness, and achieve a mentally clear and emotionally calm and stable state.
Exercise
- Exercise is being recognized as an important modality for gaining good health and recovering from illness and disease.
- Exercise like cycling and walking are great ways to make sure that the TB infection that was once in your system has been completely eradicated. Once recovered, it is a good idea to keep up the exercise, as this is a factor in stopping the TB from returning at a later date.
-
Rehabilitation Service to TB Patients
- Emotional support must be provided to patients with TB and their families during illness. Receiving TB diagnosis is often regarded by patients as a real stigma that isolates them from their family and society. Psychologists can support patients to help reduce misconceptions and socially integrate former patients.
- TB is a contagious disease that induces fear and social isolation and needs a long period of drug administration, sometimes with adverse effects. Therefore, therapeutic education is very important, which serves the purpose of explaining to patients and their families about the condition of the disease, the risks of contagiousness, the stages of treatment and prognosis.
- Exercise may be light initially, followed by assisted and active exercise. Once the patient’s condition is stable, a 6-minute walk test may be done in the room or corridor. The intensity should be progressively increased, depending on the patient’s tolerance.
- Nutrition: Weight loss is associated with fatigue and decreased exercise capacity. There is a risk for the patient not recovering body weight at the end of drug therapy, despite receiving correct TB treatment. Nutritional supplementation may play a positive role in the recovery of these patients.
- Tuberculosis Drug side effects: A proactive clinical approach is required to replace/stop the use of the concerned drugs.
- Providing Assistive devices Hearing aids, cochlear implants, tinnitus-masking devices, mobility aids, and prosthetic/orthotic devices improve the quality of life of patients.
- Corrective Surgery: May be required in TB of the bones, spine etc.
- Community and home-based care: This becomes important in severe neuromuscular deficits and movement disabilities.
- Physiotherapy: A trained physiotherapist may help through:
- Sputum clearance technique for reduced sputum quantity, better ventilation and relief of symptoms
- Cough education involving body positioning during coughing, control of breathing in coughing to achieve mobilization and secretions
- Counselling: Psychological support is required for facing long-term/permanent disabilities like loss of vision and hearing loss as side effects of the drugs, paralysis in TB meningitis, infertility in genital TB etc.
- Livelihood options: NGOs and support groups can create such options and/or facilitate treated patients to find various livelihood options
Psychosocial Support to TB Patients
ContentWho can provide Psychosocial support?
Family Members, Peer groups, treatment support groups, TB Champions, Community Health Volunteers(CHVs) and NGOs can provide psychosocial support to TB patients and their families by:
- Building a strong sense of community
- Helping the patients to contact a health worker or visit a health facility
- Providing treatment support to take their drugs and finish their treatment. Family members, community-based volunteers and workers can be trained as treatment supporters by NGOs
- Facilitating patients to access DBT for nutritional support under NPY
- Helping TB patients with comorbidities to visit the referral facility for treatment
- Treatment adherence support through peer support and education and individual follow up
- Home-based palliative care for TB
- Awareness generation, providing right information, behaviour change communication and community mobilisation for reducing stigma and discrimination
- Facilitating patients to join yoga/meditation/exercise groups once the active phase is over
- Facilitating and arranging rehabilitative services for problems/disabilities in TB patients
- Social and livelihood support
- Food supplementation
- Income-generation activities(NGO can start or facilitate patients to join activities like candle making, making festival-related goods)
- Sensitising PRIs to engage TB patients(who can work) through the Mahatma Gandhi National Rural Employment Guarantee Scheme(MGNREGS)
Rehabilitation service to TB patients
ContentThe holistic management of Tuberculosis (TB) patients can improve their life expectancy. The importance of addressing malnutrition, adverse drug reactions, psycho-social well-being, and catastrophic expenses correctly and in a timely fashion is essential in reducing morbidity and mortality.
Table: Rehabilitation services for TB patients Rehabilitation Services for TB Patients Care Providers Key Components Nutritional Rehabilitation 1. Senior Treatment Supervisor
2. TB Health Visitors
3. Accredited Social Health Activists (ASHAs)
4. Auxiliary Nurse Midwife (ANM)
5. TB treatment supporter
6. Medical officers at Peripheral Health Centre (PHC), Community Health Centre (CHC) level
-
Supporting nutritional needs of TB patients through Ni-kshay Poshan Yojana
-
Management of undernutrition in nutrition rehabilitation centres (NRCs)
-
Linkages for extra nutritional support for TB patients like the public distribution system (PDS) or food security act.
Pulmonary Rehabilitation
1.Physiotherapists (preferable one male and one female)
2. Nurses
3. Attendant
Management of physical and psychological impairment due to the disease to lower the handicap. Physical Rehabilitation -
therapists (preferable one male and one female)
-
Nurse Doctors
-
Surgeons
-
Physio
-
Attendant
-
Management of post-treatment sequelae by early identification and periodic assessment.
-
Comorbidity management
Social Rehabilitation 1. TB Health Visitors
2. Accredited Social
3. Health Activists (ASHAs)
4. Auxiliary Nurse Midwife (ANM)
5. TB treatment supporter
6. Medical officers at PHC, CHC level
7. Ni-kshay Mitra
-
Linkage for vocational rehabilitation e.g., Skill India
-
Synergy between social welfare support systems like:
-
Rashtriya Swasthya Bima Yojana (RSBY)
-
TB pension schemes
-
National rural employment guarantee scheme
-
National Health Protection Scheme (NHPS) for palliative care and rehabilitation
Mental Rehabilitation 1. Psychiatrist
2. Psychologists / Counsellors
3. TB Health Visitors
4. Accredited Social
5. Health Activists (ASHAs)
6. Auxiliary Nurse Midwife (ANM)
7. TB treatment supporter
8. Medical officers at PHC, CHC level
-
Psychological counselling to the patient and caregivers.
-
Assisting patients in the planning of decisions related to the end-of-life stage.
Patient rehabilitation is ensured by:
-
1. IT-based monitoring via Ni-kshay platform
-
2. Community-based monitoring
-
3. Surveillance: A comprehensive surveillance system for TB patients and their providers built into eNikshay. This is supported by a call centre for user-friendly private reporting and patient monitoring.
Resource
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Rehabilitation services to TB patients comprise Nutritional, Physical, Pulmonary, Social and Mental Rehabilitation.
False
True
2
The holistic management of tuberculosis (TB) patients can improve life expectancy. The importance of addressing malnutrition, adverse drug reactions, psycho-social well-being, and catastrophic expenses correctly and in a timely fashion is essential in reducing morbidity and mortality.
-
Palliative Care in TB patients
ContentPalliative care is specialised medical care for people living with a serious illness.
- This type of care is focused on providing relief from the symptoms and stress of the illness.
- The goal is to improve the quality of life for both the patient and the family.
- Palliative care is based on the needs of the patient, not on the patient’s prognosis.
Need for Palliative Care for TB Patients
TB is, and should be, a curable disease; however, each year an increasing number of patients acquire or develop drug-resistant TB (DR-TB), which has a much lower cure rate.
While the expectations are to have increasing numbers of treatment success rates, DR-TB remains a life-threatening condition with high mortality.
The life-threatening nature of DR-TB and the burden of disease management in terms of symptoms, adverse treatment effects, adherence, stigma and subsequent discrimination and social isolation, clearly show the need for care that addresses physical, social and emotional suffering by patients.
Thus, the need for palliative care is being increasingly recognised as an important part of the continuum of care for DR-TB patients.
Challenges in Palliative Care
At present, there is a scarcity of trained health workers and local community-based palliative care resources in the settings that are most in need. Although clinical expertise in palliative care for patients who die in respiratory distress has developed considerably, individuals with DR-TB are yet to see the benefits.
Services under Palliative Care for TB
- Addressing pain and symptom control (including respiratory insufficiency)
- Nutritional support
- Medical intervention after treatment cessation
- Ensuring the appropriate place of care, preventive care, infection control and end-of-life care
Supportive Measures in Palliative Care
Image
Resources
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Palliative care is based on a patient’s prognosis.
True
False
2
Palliative care is based on the needs of the patient, not on the patient’s prognosis.
YES
YES
Patients' charter for TB care
ContentThe Patients’ Charter for Tuberculosis Care (the Charter) outlines the rights and responsibilities of people with TB. It empowers people affected by TB and their communities through this knowledge. Initiated and developed by persons affected by TB from around the world, the Charter makes the relationship with healthcare providers a mutually beneficial one.
The Charter sets out ways in which people affected by TB, the community, health providers (both private and public), and governments can work as partners in a positive and open relationship with a view to improve TB care and enhance the effectiveness of the healthcare process.
It allows for all parties to be held more accountable to each other, fostering mutual interaction and a positive partnership.
Principles of the Patients’ Charter for TB Care
- The charter practices the principle of Greater Involvement of People with TB (GIPT).
- This affirms that the empowerment of people with the disease is the catalyst for effective collaboration with health providers and authorities and is essential to victory in the fight to end TB.
Parts of the Patients’ Charter for TB Care
There are two main parts in the patients’ charter for TB care which cover:
- Patients’ rights
- Patients’ responsibilities
These parts are further delineated in Tables 1 and 2 below.
Table 1: Patient's Rights According to the Patient's Charter for TB Care Rights Explanation of rights: You, as the patient, have the right to: Care - Free and equitable TB quality care meeting the International Standards of Tuberculosis Care (ISTC)
- Benefit from community-care programmes
Dignity - Be treated with respect and dignity
- Social support of the family, community and national programmes
Information - Information about available care services — be informed about condition and treatment, know drug names, dosage and side-effects
- Access your medical records in the local language
- Have peer support and voluntary counselling
Choice - A second medical opinion, with access to medical records
- Refuse surgery if drug treatment is at all possible
- Refuse to participate in research studies
Confidence - Have your privacy, culture and religious beliefs respected
- Keep your health conditions confidential
- Care in facilities that practice effective infection control
Justice - File a complaint about care, and have a response
- Appeal unjust decisions to a higher authority
- Vote for accountable local and national patient representatives
Organization - Join or organise peer support groups, clubs and Non-governmental Organisations (NGOs)
- Participate in policy-making in TB programmes
Security - Job security, from diagnosis through to cure
- Food coupons or supplements, if required
- Access to quality-assured drugs and diagnostics
Table 2: Patients' Responsibilities According to the Patients' Charter for TB Care Responsibilities Explanation of responsibilities: You, the patient, have the responsibility to: Share information - Inform healthcare staff all about your condition
- Tell staff about your contacts with family, friends, etc.
- Inform family and friends and share your TB knowledge
Contribute to community health - Encourage others to be tested for TB if they show symptoms
- Be considerate of care providers and other patients
- Assist family and neighbours to complete treatment
Follow treatment - Follow the prescribed plan of treatment
- Tell staff of any difficulties with treatment
Solidarity - Show solidarity with all other patients
- Empower yourself and your community
- Join the fight against TB in your country
Resources
- The Patients’ Charter for Tuberculosis Care, The Global Plan to Stop TB 2006-2015.
- Capacity-building of Affected Communities for Accelerated Response to Drug-resistant Tuberculosis in the South-east Asia Region, WHO, 2019.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test According to the Patients' Charter for TB Care, it is not the patient’s responsibility to support other patients. True False 2 According to the Patients' Charter for TB Care, patients have a responsibility to support other patients, show solidarity and empower their communities. Yes Yes
-
IEC-CH12: Linkages to Social Support Schemes
FullscreenDirect Benefit Transfer(DBT) under NTEP
ContentDirect Benefit Transfer (DBT) is a major initiative of Government of India (GoI) whereby any government subsidy or benefit is to be transferred directly into the beneficiary's bank accounts. Intermediary government agencies only manage the process of payments, without handling actutal money.
NTEP is one of the first health programmes in India to use a fully adopt DBT. It uses an end to end electronic system, to digitise beneficiary information and transfer monetary benefits. In NTEP to process benefits, two electronic systems are used, Ni-kshay (operated by NTEP) and PFMS (Public Finance Management System, operated by the Ministry of Finance). Ni-kshay enables Direct Benefit Transfer by digitizing the beneficiaries(bank account details of patients, treatment supporters and providers) and calculates of incentives/ benefits (eligible payment) and processes them for payment through PFMS under various schemes. The various schemes operational under NTEP are:
- Nikshay Poshan Yojana(NPY)
- Tribal Support Scheme
- Treatment supporter’s Honorarium
- Incentive for Notification and Outcome
DBT Schemes in Nikshay
Other Local DBT Schemes
ContentThere may be other Central or State government schemes and programmes that beneficiaries related to the TB program are eligible for, over and above the 4 schemes provided by the central government through NTEP. Some examples are:
- State Illness Relief Fund (can serve seriously ill TB patients)
- Chief Minister’s Farmers Security Scheme
- Nutritional Support to DR-TB Patients
- Sanjay Gandhi Niradhar Yojana
- Surakhaya Yojana
- Pridhar Parasar Yojana
- Scheme for treatment of critical disease for schedule caste/schedule Tribe and people below poverty line (BPL).
- Rastriya Swasthiya Bhima Yogana (RSBY) reimbursement for those TB patients who required hospitalisation
- Sudurvarti Sahayaks from CM's Sudurvarti Gram Yojana involved TB services
These schemes are paid through their respective payment processing channels and not through Ni-kshay.
Criteria for availing DBT Scheme benefits under NPY
Content- All TB patients notified on or continues treatment after 1st April 2018 including all existing TB patients under treatment are eligible to receive incentives.
- For availing DBT scheme benefits under NTEP Programme, TB patients have to provide their bank details to the nearest NTEP Health facility.
- The patient must be registered\notified on the NIKSHAY portal.
- Each beneficiary can be linked to unique savings bank account belonging to him/her. Beneficiaries without bank accounts need to be facilitated to open bank accounts in any bank as convenient.
- If a Beneficiary does not have a bank account and is unable to open a new bank account, his/her relative’s bank account may be used(immediate family member such as parents, spouse, siblings).
- If a relative’s bank account is used, written consent should be taken from beneficiary.
- If a bank account has already been used for another beneficiary, it cannot be re-used for another beneficiary. If a new Bank account needs to be opened, it’s easy to open a zero-balance account with Indian Post Payments Bank.
-
-
IEC-M4: Advocacy, Communication & Social Mobilization (ACSM)
Fullscreen-
IEC-CH13: Concepts in ACSM
FullscreenWhat is A in ACSM
ContentIn ACSM, "A" stands for Advocacy. "Advocacy" is an activity by an individual or a group that aims to influence the decisions within political, economic and social institutions.
Advocacy focuses on influencing policy-makers, funders and international decision-making bodies through a variety of channels:
- Conferences, summits and symposia
- Celebrity spokespeople, press conferences, news coverage
- Meetings between various levels of government and civil society organizations
- Official Memoranda of Understanding (MoU), parliamentary debates and other political events
- Partnership meetings, patients’ organizations, private physicians, radio and television talk shows, and service providers.
Types of advocacy
- Policy advocacy: Mainly targets policy-setting, influencing policymakers to incorporate the latest evidence and informs senior politicians and administrators how an issue will affect the country, and outlines actions to take for improving the laws and policies.
- Programme advocacy: Targets opinion leaders at the community level on the need for local action.
- Media advocacy: Validates the relevance of a subject, puts issues on the public agenda and encourages the media to cover TB-related topics regularly and in a responsible manner so as to raise awareness of possible solutions and problems.
Resources
- Advocacy, Communication & Social Mobilization (ACSM) for Tuberculosis Control - A Handbook for Country Programmes, WHO, 2007.
- Operational Handbook on Advocacy, Communication & Social Mobilization for RNTCP, Central TB Division, MoHFW, GoI, 2014.
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
News reports on World TB day celebrations are an example of which of the following types of advocacy?
Policy advocacy
Programme advocacy
Media advocacy
None of the above
3
Media advocacy encourages the media to cover TB-related topics regularly and in a responsible manner so as to raise awareness of possible solutions and problems.
Yes Yes What is C in ACSM
ContentCommunication aims to favourably change knowledge, attitudes and practices among various groups of people.
Types of communication in healthcare are:
- Oral/verbal communication- by word of mouth (speech/talk)
- Written communication- exchange of facts, ideas and opinions through the use of written materials
- Non verbal communication- through gestures, body language or posture, facial expressions, and eye contact
- Visual communication- exchange of ideas through visuals
Health communication aims to influence and empower individuals, populations and communities to make healthier choices. It frequently informs the public of the services that exist for diagnosis and treatment and relays a series of messages about the disease. It aims to inculcate behaviour change for healthy life choices.
E.g.: “Seek treatment if you have a cough for more than two weeks”, “TB hurts your lungs” or “TB is curable”.
Approaches to health communication
1. Informative communication
Provides information about a new idea and makes it familiar to people.
2.Educative communication
A new idea on health behaviour is explained, including its strengths and weaknesses.
3.Persuasive communication
Usually in the form of a message that promotes a positive change in behaviour and attitudes, and which encourages that audience to accept the new idea. This approach to message development involves finding out what most appeals to a particular audience. Persuasive approaches are more effective than coercive approaches in achieving behaviour change.
4.Prompting communication
Messages are designed so that they are not easily ignored or forgotten they can be used to remind the audience about something that reinforces earlier messages.
Behaviour Change Communication (BCC)
- Behaviour Change Communication (BCC) is an interactive process of any intervention with individuals, groups or communities to develop communication strategies to promote positive health behaviours which are appropriate to the current social conditions and thereby help the society to solve their pressing health problems.
- BCC creates an environment through which the affected communities can discuss, debate, organize and communicate their own perspectives on TB.
- It aims to change behaviour – such as persuading people with symptoms to seek treatment – and to foster social change, supporting processes in the community or elsewhere to spark a debate that may shift social mores and/or eliminate barriers to new behaviour.

Figure: Behaviour Change Communication
Resources
- Advocacy, Communication & Social Mobilisation (ACSM) for Tuberculosis Control - A Handbook for Country Programmes, WHO, 2007.
- Operational Handbook on Advocacy, Communication & Social Mobilisation for RNTCP, Central TB Division, MoHFW, GoI, 2014.
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What does the environment created by behaviour change communication encourage the TB-affected communities to do?
Discuss, debate, organize, communicate
Discuss, organize, implement, communicate
Organize, enforce, communicate
None of the above
1
Behaviour change communication creates an environment through which the affected communities can discuss, debate, organize and communicate their own perspectives on TB.
What is SM in ACSM
ContentSocial Mobilisation (SM) is the process of bringing together different stakeholders and building partnerships to prevent, detect and cure TB. It generates dialogue, negotiation and consensus among a range of players that includes decision-makers, the media, Non-government Organisations (NGOs), opinion leaders, policy-makers, the private sector, professional associations, TB-patient networks and religious groups.
At the heart of social mobilisation is the need to involve people who are either living with active TB or have suffered from it at some time in the past.
Aims of Social Mobilisation
• Increase awareness of the disease (TB) and the demand for diagnosis and treatment services
• Expand service delivery through community-based approaches
• Enhance sustainability, accountability and community ownership of TB services
Activities for Social Mobilisation
- Group and community meetings - Engaging yuva/ mahila mandals, village health sanitation and nutrition committees under the National Rural Health Mission (NRHM), sensitization of local and religious leaders on TB and related stigma in the community. Regular meetings at the village level to address myths and misconceptions and help people with TB symptoms seek timely and appropriate care or referrals.
- School activities - Conducting TB awareness campaigns in schools by addressing the school assembly/ class, painting competitions, rallies, road shows, essay competitions, drawing competitions, exhibitions, dramas, pictorial presentations, quizzes, puzzles, puppet shows, leaflet distributions etc.
- Traditional media group performances - Performing entertainment-centred folk performances, street plays with scripts centred around TB awareness messages.
- Rallies and road shows - Spreading TB related messages on World TB day.
- Home visits - Encouraging interpersonal communication and empowering former TB patients and TB champions to become Directly Observed Treatment, Short-course (DOTS) providers.
Here, inter-personal communication and group communication are the main channels of communication for disseminating TB-related key messages.
In the National TB Elimination Programme (NTEP), partner NGOs play an important role in social/ community mobilisation. It generates dialogue, negotiation and consensus, engaging a range of players in interrelated and complementary efforts while taking into account people’s needs.
Resources
- Advocacy,Communication & Social Mobilisation (ACSM) for Tuberculosis Control - A Handbook for Country Programmes, WHO, 2007.
- Operational Handbook on Advocacy, Communication & Social Mobilisation for RNTCP, Central TB Division, MoHFW, GoI, 2014.
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
A roadshow was conducted by local PHC in a village on World TB day with message to End TB. This is an example of:
Policy making
Social mobilisation
Institutional strengthening
Diagnostics
2
Roadshow is one of the activities of social mobilisation strategy which aims at increasing awareness about the disease, involving major stakeholders.
-
IEC-CH14: Guidelines & protocols for ACSM Activities
FullscreenOrganising Community meetings
ContentCommunity meetings are organised by the Senior Treatment Supervisor (STS) or the partner Non-Government Organisation (NGO) under the supervision of the Medical Officer.
- These meetings are conducted to create awareness about TB among the general population, community leaders, people’s representatives, Self-help Groups (SHGs), community volunteers, traditional healers, etc.
- These meetings are organised in a community centre or any other suitable place at the village and slum level.
- To maximise the output, the community meetings should be planned appropriately.
Following are the steps involved in planning a community meeting:
Image
Resources
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Who supervises the conduct of community meetings? DTO STO MO STLS 3 Community meetings are organised by the STS or the partner NGO under the supervision of the Medical Officer. YES YES Peer group interventions
ContentCommunity or peer-led measures penetrate better into the intricate layers of key population and facilitate Intensive Case Finding (ICF). Peer group support helps patients deal with challenges that they face during the treatment period. Several Tuberculosis (TB) patients find their treatment period stressful and having a peer to talk to, who has undergone similar challenges, and a doctor or counsellor to answer their questions, helps build confidence and realization that they are not alone in this journey.
Image
Figure 1: Characteristics of a Peer Group
Image
Figure 2: Peer group interventions has an influence on the knowledge, attitude, and quality of life of the pulmonary tuberculosis patients
-
Peer group intervention is human centered approach as it involves perspectives from the patients and their care givers encouraging them to openly discuss their concerns. Peer group intervention builds collective strength and solidarity among patients attending the group meeting and improve their treatment experience by learning from experience of peers. Talking to others in support groups reduces anxiety, improves self-esteem, and helps members' sense of well-being overall.
-
Peers are an underused resource for strengthening TB control among socially excluded populations. There is a need for further research into the contribution of peers to TB control, including analyses of economic effectiveness.
Peer group interventions for TB patients are:
-
Conducting patient support group meetings where patients and care givers can discuss their concerns and invite other patients who have addressed similar issues in their treatment. Social support from family and friends, helps in patient’s adherence to treatment. Treatment adherence is a key to the completion of TB treatment. The support is part of an external stimulus which can develop a particular behavior in human.
-
Peer group members can facilitate linkages to nutrition and other forms of support for TB patients – Patients or caregivers can be linked to support services like counselling, nutrition and social entitlements, either from the NTEP or through other public schemes or community structures.
-
Peer group members can help each other by sharing their knowledge to create linkages with the medical support systems – TB patients who develop side effects due to medication, should be linked for medical support during the meetings. Medical Doctor/STS/TBHV/CHO shall provide counselling to patients regarding side effects of the TB treatment and how to address the issues. Members act as role models for each other. Seeing others who are contending with the same adversity and making progress in their lives is inspiring and encouraging.
-
Peer group members can facilitate interactions of family members with Medical officer (M.O.)/National TB Elimination Programme (NTEP) staff – Peer group meetings can be used to counsel the caregivers on how to take care of the patient at home. A support group is a safe place for someone who needs to talk about intensely personal issues, experiences, struggles, and thoughts.
Resources
Guidance document on community engagement under NTEP Central TB Division, MoHFW, GoI September 2021
NTEP Training Modules 5 to 9, Central TB Division, MoHFW, GoI 2020
Assessment
Question
Answer
1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Peers are an underused resource for strengthening TB control among socially excluded populations. There is a need for further research into the contribution of peers to TB control, including analyses of economic effectiveness.
True
False
1
Community or peer-led measures penetrate better into the intricate layers of key population and facilitate Intensive Case Finding (ICF).
-
ACSM activities in schools
ContentIn order to create awareness and mobilise young students to fight against TB, the National TB Elimination Programme (NTEP) encourages TB awareness campaigns in schools.
Common school activities undertaken to create awareness about TB among children include the following:
- Addressing the school assembly/ classes
- Holding painting competitions
- Holding rallies and road shows
- Holding essay competitions
- Holding slogan competitions
- Reading TB leaflets during prayers
- Organising quizzes
- Puzzle games
- Pictorial presentations (presenting TB-related information in the form of pictures)
- Organising exhibitions (posters, models etc.)
- Katputli shows
- Distributing leaflets containing information about TB
Steps for Organising School Activities
School activities could prove very effective, provided they are well planned. Following are the steps for effective organisation of school activities:
Image
Resources
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Training school teachers is a part of the ACSM activities in schools. True False
1
Training of school teachers, who will in turn conduct school activities in a planned manner is a part of ACSM activities in schools. YES
YES
Community mobilization strategies-Tribal areas
ContentTribal people (10.4 Cr, 8.6% of total population) have higher prevalence (703 per 100,000) of TB compared to national average (256 per 100,000).10.4% of all TB notified patients are from tribal communities. The National TB program has prioritized this subgroup of population through Tribal Action Plans since 2005.
As a part of the Multisectoral collaboration with various Ministries, a guidance note on the joint action plan was developed by Ministry of Health and Family Welfare (MoHFW) and Ministry of Tribal Affairs in October 2020 and shared with the Secretaries of all States/ UTs for field level implementation. Tribal TB initiative, a unique partnership between the Ministry of Health and Family Welfare and Ministry of Tribal Affairs was initiated to improve the cascade of TB care and support services among Tribal Populations in India. The technical assistance for this initiate will be provided by USAID.
Challenges in communities in tribal areas:
Access, availability, and utilization of TB care services of these communities are hindered by:
- Geographical barriers
- Poor state of social determinants
- High impact of malnutrition, insufficient community involvement
- Health system constraints including lack of trained human resources
- Cultural and communication gaps between the care provider and the community, etc.
- The COVID-19 pandemic has probably further worsened the situation.
Community mobilization strategies in tribal areas:
Image
Various departments which play a role in community mobilization in Tribal areas:
- National Program Management Unit (NPMU) provides technical assistance in monitoring and implementation of the Tribal TB Initiative.
- Coordination among National Tuberculosis Elimination Programme (NTEP), National Health Mission (NHM), Ministry of Development of Northeastern Region, Ministry of Tribal affairs at National, state and district levels through national level Technical Support Unit.
Image
- Coordination with ‘Centre of Excellence’ within the Ministry of Tribal Affairs, with a key focus on TB.
- Partnering with private sector players for leveraging resources for TB elimination in Tribal communities.
- Documenting best practices, and commission tribal health research studies in collaborations with identified government institutions.
- Various departments collaborate for improving the operational excellence of existing demand-side interventions such as Village Health Sanitation and Nutrition Days (and committees), Jan Arogya Samiti platforms, Jan Andolan initiatives, engaging TB-Champions, and training of faith healers and other community influencers.
Resource
Assessment
Question Answer
1
Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Community mobilization strategies in tribal areas include home visits. True False 1 Community mobilization is about seeking cooperation and support from different stakeholders in general and the community in specific.
Home visits will improve awareness on various government schemes, provisions, facilities available for TB patients and to improve treatment literacy and adherence among TB patients in tribal areas.
Community mobilization strategies-Rural areas
ContentRural populations have more limited access to primary care physicians than residents of urban areas, and are older, sicker, and poorer than urban counterparts. Travel to reach a primary care provider may be costly and burdensome for patients living in remote rural areas, with subspecialty care often being even farther away. These patients may substitute local primary care providers for sub specialists, or they may decide to postpone or forego care. Many social determinants act as barriers for rural communities to access health services.
Challenges faced by communities in rural areas are:
- Higher poverty rates, which can make it difficult for participants to pay for services or programs
- Cultural and social norms surrounding health behaviors
- Low health literacy levels and incomplete perceptions of health
- Linguistic and educational disparities
- Limited affordable, reliable, or public transportation options
- Unpredictable work hours or unemployment
- Poor primary healthcare and infrastructure in rural areas
- Lack of access to tuberculosis testing and treatment centers in remote unreached areas
- Unregulated indigenous system of medicine
- Poor airborne infection control
- Poor nutrition and Malnourishment
Community mobilization strategies in rural areas include:
Image
Various committees which play a role in community mobilization in rural areas:
Image
- Village Health Sanitation and Nutrition Committees (VHSNCs) - In each Gram Panchayat, Village Health Sanitation and Nutrition Committees (VHSNCs) have been formed at the village level under National Health Mission (NHM). These committees are entrusted with community-level planning and implementation of health and sanitation, and have representation from the local government, local health centre, and the local community.
- Panchayat Raj Institution (PRI) - Members of PRI refers to local self-government at the village level. The village pradhan (head) and members of the Panchayat are elected members of the Gram Panchayat. They are the key people who can, after sensitization, mobilize the community for TB care and control and make allocations for TB patients’ nutrition and travel requirements.
- Yuva mandal/Mahila mandals (Youth/women’s clubs) - Community-level federations of young boys/girls/women, sometimes even comprising several women SHGs.
- Self-help groups (SHG) - An SHG is a group of individuals with a homogenous social and economic background, who voluntarily come together to regularly save small amounts of money and contribute to a local fund to meet the members’ emergency needs on a mutual help basis. These groups collectively manage their payments and ensure proper use of credits. Many NGOs currently engaged in the project are involved in formation/registration of these SHGs. It would be advisable to involve these NGOs for ease of implementation.
- Community-based organizations (CBO) - A CBO is a small group of people from a community, who come together for a particular purpose. It may be a local association of people mobilized around water conservation, mother and childcare, sustainable agriculture, education, or adolescent health; a group of social service persons; or any other such active group in a village.
Resource:
Assessment:
Question
Answer
1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Community mobilization strategies in rural areas includes empowering key decision-makers, people affected by TB, and marginalized and vulnerable populations.
True
False
1
This leads to raising awareness of services available and general health literacy surrounding TB.
More people accessing public health services will lead to better utilization of services.
- Higher poverty rates, which can make it difficult for participants to pay for services or programs
Community mobilization strategies-Urban areas
ContentIndia has historically been called a rural economy but has witnessed fast-paced urbanisation in the last few decades. Currently, one-third of our population is urban. It is projected that by 2030, 46% of our population will be living in cities. Urban areas are characterised by high economic activity, diversity of livelihood opportunities and infrastructural development. Migrants are drawn to urban areas for employment opportunities and to establish a better life for themselves and their families.
Challenges faced by communities in urban areas: Most individuals and families living in urban areas face multiple and overlapping vulnerabilities. The vulnerabilities faced by urban people come from:
-
-
1. Residential vulnerability: Slum or slum-like habitations face the insecurity of tenure and are unserved or under-served with basic public services like sanitation, clean drinking water and drainage.
-
2. Occupational vulnerability: Urban residents working in the informal sector, daily wage labourers, factory workers working without adequate safety equipment, sanitation workers without adequate protective equipment and bonded labour are occupationally vulnerable.
-
3. Social vulnerability: Hinders access to resources such as health services, education and access to government schemes/ programmes because of societal discrimination. Widows, transgenders, the elderly, the disabled and those belonging to scheduled castes and tribes face discrimination because of their disadvantaged social status.
Social and systemic barriers to accessing public healthcare services in urban areas:
-
-
1. Limited availability of government primary healthcare services: Primary healthcare facilities in urban areas are limited in number. Urban residents have access to ‘larger’ or secondary/ tertiary hospitals (even for minor ailments) and private sector providers, paying heavily out of their pockets.
-
2. Overcrowding in public hospitals: Patients are forced to procure products and diagnostic services from other private providers due to lengthy waiting times.
-
3. Inconvenient timings: As most public health services open in the morning hours, consulting a doctor may mean the loss of a day’s wage for the poor. The alternative is to go to private doctors during evening hours.
Community mobilisation strategies for urban areas: Key strategies for community mobilisation in urban areas to facilitate improved case-finding, testing and treatment are given below.
-
-
1. Peer outreach at TB testing and treatment sites: Peer educators will be linked with TB service providers. These can be peers from a targeted intervention or HIV care and support programmes. Community or peer-led measures will penetrate better and facilitate Intensified Case Finding (ICF).
-
2. Mobile unit with the display of Information, Education and Communication (IEC) materials along with a facility for sputum collection and transportation.
-
3. Safe virtual or physical spaces (for example telephone hotlines, or drop-in centres) to seek information and referrals for care and support for TB treatment. Weekly/ fortnightly awareness sessions, testing days and follow-up testing days for TB can be organised in coordination with District TB Officers (DTOs).
-
4. Involvement of Community-based Organisations (CBOs)/ civil societies
Various departments/programs which play a role in community mobilisation in urban areas:

Resources
Assessment
Question
Answer
1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Collaboration of National TB Elimination Programme (NTEP) and National Urban Health Mission (NUHM) is to develop strategies to address urban TB.
False
True
2
National Urban Health Mission integrates vertical health programs in its services. It makes special efforts to make its services accessible by the urban marginalized population through its location, service delivery, outreach and making its service providers sensitive to the needs of its target population.
-
IEC material for general public
ContentInformation, Education and Communication (IEC) material for the Public has been made available on the Central TB Division official website. In the home page of https://tbcindia.gov.in under the ACSM/IEC option IEC materials like launch video on World TB Day, Posters on TB Arogya Sathi, Ni-kshay Poshan Yojana, Ni-kshay Patrika, Documentaries, Radio Spots, TV Spots/TVC’s, Script for Nukkad Natak’s and Exhibition Panels are available in the public domain.
Image
Figure 1: IEC Material available in Public Domain: Source: tbcindia.gov.in
Information, Education and Communication (IEC) materials for the general public include:
- Mid-Media
- Banners
- Flip charts
- Wall writings
- Hoardings
- Posters
- Pamphlets
- Mobile vans and videos on wheels
- Folk performances
- Kiosks individuals - Face-to-face communication along with audio-visual communication for better message retention. Useful in dispelling myths and practices.
Image
Figure 2: Poster for TB Arogya Sathi App: Source: tbcindia.gov.in
Image
Figure 3: Poster for Nikshay Poshan Yojana: Source: tbcindia.gov.in
- Mass media
- Newspapers
- Television
- Radio
- Magazines
Image
Figure 4: Snapshots from a TVC’s: Source: tbcindia.gov.in
- Social Media
- Blogs
- YouTube
Image
Figure 5: Ni-kshay e-patrika: Source: tbcindia.gov.in
- Interpersonal Communication (IPC)
- Counselling
- Home-visits
- Community Dialogue
- Public meetings and gatherings
Image
Figure 6: Script for Nukkad Natak available on Central TB Division website: Source: tbcindia.gov.in
Resources
Assessment
Question Answer
1
Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Counselling and home visits are not part of the IEC materials/ tools available to the public. False True 1 Counselling and home visits are part of the interpersonal communication of the IEC strategy. IEC Strategies for Government & Private Medical Practitioners
ContentInformation, Education and Communication (IEC) is defined as a comprehensive approach that spans across mass media, digital campaigns, strategic partnerships and inter-personal ground level activities.
Standardised training of practitioners
- All practitioners, government and private must receive up-to-date training as and when the programme launches newer updates to the TB treatment and guidelines.
- The trainings shall be conducted through the use of standardised materials utilising the Swasth e-Gurukul Platform.
- The IEC material developed for the practitioners must not only include TB symptoms but also focus on free diagnostics, free treatment, financial support available under the National TB Elimination Programme (NTEP).
- Only NTEP approved IEC materials in the form of print media (pamphlets, posters) or digital media (videos, audios) shall be provided to the private practitioners in the area by the District TB Officers (DTOs), for display in the health care establishments as well as for patient communication.
- All practitioners must be trained on the identification of Latent TB infection and importance of initiating TB preventive treatment.
Capacity building
- Use of Nikshay Sampark (Toll free number: 1800- 11-6666) for feedback/concerns should be promoted from providers as well as patients.
- The training should also be provided to all the practitioners in order to be able to use the Ni-kshay digital application for TB notification and reporting all other related aspects.
- System should be set up to enable all practitioners to receive the government’s demi official (DO) letters as and when circulated.
- All government practitioners should be educated on how to build capacities of Mahila Arogya Samiti (MAS) and Accredited Social Health Activists (ASHA) in TB control at the community level.
- Capacities of District Programme Supervisors , District programme Co-ordinators, Senior Treatment Supervisors should be built under the leadership of the DTO to be able to extend support to the government medical practitioners in day to day TB control activities.
- Professional medical associations must be sensitized to conduct regular Continued Medical Education (CMEs) programmes in TB care and elimination for the private sector providers
Involvement of Patient Provider Support Agencies (PPSAs) and Non-Governmental Organisations (NGO’s)
- A list of contact details of local public health staff/officers and PPSA (where present) should be made available to all private providers.
- Wherever possible PPSAs must be utilised to help the private sector establishments provide patient centric support by facilitating implementation of a single window for diagnostic and treatment services, notification, patient linkage with social welfare, contact investigation, TB preventive treatment and treatment adherence support.
- DTOs should ensure coordination with PPSA for DR-TB services.
- NGOs functioning in the area may also be involved to support the practitioners in conducting IEC campaigns in the communities.
- Advocacy and policy support groups may be formed with the practitioners and medical associations to strengthen the TB control activities in the private sector.
Resource:
Training Modules (5-9) For Programme Managers & Medical Officers, CTD, MoHFW, India,2020.
National Strategic Plan For Tuberculosis Elimination 2017–2025, MoHFW, India, 2017
Guidance Document on STEPS (System for TB Elimination in Private Sector) in Kerala.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Information, Education and Communication (IEC) strategies for government & private medical practitioners includes only interpersonal communication.
True
False
1
Information, Education and Communication (IEC) strategies for government & private medical practitioners includes mass strategies as well as interpersonal communication
Yes
Yes
- All practitioners, government and private must receive up-to-date training as and when the programme launches newer updates to the TB treatment and guidelines.
IEC strategies for CHVs
ContentInformation, Education & Communication (IEC) strategies for community health volunteers (CHVs) are:
Standardised TB training
- Training for all CHVs should be conducted through standardised training material approved and published under the Central TB Division (CTD)
- E – modules available on Swasth e-Gurukul platforms should be used in order to maintain uniformity of the training processes as well as for conducting pre and post training assessments
- Regular capacity building workshops for CHVs may be conducted along with CTD and partner organizations as per the need of the localities identified.
Dissemination of simplified IEC tools to all the CHVs
- NTEP’s IEC material must be simplified, translated to local language and must be provided to all CHVs through the programme.
- Program / medical jargon (e.g.: District Microscopy centre (DMC)/ rapid molecular tests) must be avoided for ease of understanding.
- All CHVs must be equipped with necessary permissions and facilities required to display these IEC materials across common access areas, public walls, canteens, factories entry/exit points etc.
TB related events and community engagement activities
- Under the supervision of District TB Officers (DTOs), the CHVs must be guided and supported for organising events on the occasion of World TB Day, Village Health and Nutrition Day etc., with a focus to increase understanding of the prevailing TB scenario and also their commitment towards TB elimination.
- Community engagement activities must be conducted by the CHVs and should involve role plays, street plays (Nukkad Naatak on TB), video vans, group meetings, outdoor communications especially in the high-risk areas/vulnerable populations.
Training on NTEP’s digital initiatives for TB elimination
- All CHVs must be trained on the functioning of TB Arogya Saathi - a citizen and patient application launched by the Ministry of Health & Family Welfare, India that connects patients to TB health care services.
- Ni-kshay Sampark the TB helpline (Toll free number: 1800- 11-6666) must be made accessible to all CHVs across various states through which they can seek reliable information.
- CHVs must be well-informed about the Nikshay Poshan Yojana and other financial support schemes (travel support, tribal patient support etc.) available for TB patients under NTEP’s direct beneficiary transfer (DBT)
Resources:
National Strategic Plan for Tuberculosis Elimination 2017–2025, CTD, 2017
Assessment:
Question
Answer
1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Training through standardised training material available on CTD website and E – modules available on Swasth e-gurukul is an IEC strategy for Community Health Volunteers.
False
True
2
The community health volunteers can take the course and get certified, which can further aid them in managing TB patients.
+
-
-
IEC-M5: Program Management
Fullscreen-
IEC-CH15: Planning & Budgeting
FullscreenACSM planning based on needs assessment
ContentThe preparation of a research and evidence-based Programme Implementation Plan (PIP) is vital for conducting effective Advocacy, Communication and Social Mobilisation (ACSM) activities under the National TB Elimination Programme (NTEP). The plan for ACSM activities should be made based on the needs of the community.
Needs Assessment through Situation Analysis
Situation analysis should start at the TB Unit (TU) level. The Senior Treatment Supervisor (STS) should take the initiative under the guidance and supervision of the District TB Officer (DTO).
STEP 1: Identify the priority population/ geographic area
- Prepare a performance matrix for all TUs and Designated Microscopy Centres (DMCs) in the district on the basis of presumptive TB examination rate, case detection, case adherence, treatment success rate and private notification.
Table 1: Example of performance matrix (district X in state Y)
Tuberculosis Unit (TU) Presumptive TB Examination Rate % Case
notification
%
Case
adherence
%
Treatment Success Rate % Private
notification
%
TU 1 TU 2 TU 3 TU 4 - Identify the TUs/DMCs with lower performance indicators and prioritize them for ACSM activities with targeted solutions to existing challenges. Work out the likely budget and time constraints for ACSM intervention in the current financial year and in the next two years or so, in these.
- Sustain ACSM activities in other DMCs
STEP 2: Identifying key program challenges
Ascertain the main program issues in the low-performing DMCs that have been identified as priority areas by asking the following guiding questions to Medical Officer - Tuberculosis Control (MO-TC), Senior TB Laboratory Supervisor (STLS), and other concerned health staff like Accredited Social Health Activist (ASHA).
a. What are the reasons for low case detections?
i. Lack of awareness about TB
ii. High stigma and discrimination
iii. Poor access to services
b. What are the reasons for low case adherence?
i. Economic hardship
ii. Lack of care and support
iii. Lack of awareness about the importance of completing treatment
c. What are the reasons for low private notification?
i. Lack of information about the need for TB notification
ii. Lack of knowledge about TB, its diagnosis, and treatment
iii. Lack of motivation and fear of patient loss
Responses to these questions will help in identifying the various program challenges and in planning appropriate ACSM activities.
Step 3: Identify the barriers for utilisation of services
The Cough to Cure Pathway barrier analysis is a useful tool to discuss key barriers at every level in the journey from symptom to treatment. This approach is suitable to differentiate the barriers at the individual, group, and system levels.

Figure: The Cough to Cure Pathway Barrier Analysis Tool; Source: Advocacy, Communication & Social Mobilisation (ACSM) for Tuberculosis Control - A Handbook for Country Programmes, WHO, 2007.
STEP 4: Identifying and defining the target audience
The target audience for advocacy . communication and social mobilisation activities need to be decided based on the requirement
Resources
- Advocacy, Communication & Social Mobilization (ACSM) for Tuberculosis Control - A Handbook for Country Programmes, WHO, 2007.
- Operational Handbook on Advocacy, Communication & Social Mobilisation for RNTCP, Central TB Division, MoHFW, GoI, 2014.
Assessment:
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Cough to cure pathway tool helps in identifying: The audience for ACSM activities Barriers to ideal behaviours Communication strategy None of the above 2 The Cough to Cure Pathway barrier analysis is a useful tool to discuss key barriers at every level in the journey from symptom to treatment. This approach is suitable to differentiate the barriers at the individual, group, and system levels.
Yes Yes Overview of PIP
ContentThe State Programme Implementation Plan (PIPs) for health and family welfare services under National Health Mission (NHM) funding spell out the strategies to be deployed, budgetary requirements and aimed health outcomes.
PIPs are the most crucial documents in NHM through which the states/ Union Territories (UTs), identify and quantify the targets required for programme implementation for the proposed year.
PIPs are prepared by states annually as a document which is then finalised in the National Programme Coordination Committee (NPCC) meeting for administrative approval.
On finalisation of the budget in the NPCC meeting, it becomes an official document available in the Ministry's site for general viewing.
Importance of PIP
- Its a plan according to which the different activities are carried out and performance of each activity can be monitored against it.
- Approval of PIP implies that states/districts can carry out the activities mentioned in the plan.
- It is the indicator of the total budget requirement of the state for carrying out the programme activities
PIP Preparation Process under NHM
A bottom-up approach is followed for preparing the State PIP wherein the inputs are taken from blocks, cities, Community Health Centre (CHC)/ Peripheral Health Centre (PHC), and village level to prepare a DHAP. These DHAPs are then consolidated to prepare a State PIP.
Budget Heads
A total of 18 different budget heads comprises the PIP. These include:
1. Service Delivery – Facility-based
10. Review, Research, Surveillance & Surveys
2. Service Delivery – Community-based
11. Information, Education. Communication (IEC)/ Behaviour Change Communication (BCC)
3. Community Interventions
12. Printing
4. Untied Funds
13. Quality Assurance
5. Infrastructure
14. Drug Warehousing & Logistics
6. Procurement
15. Public Private Partnership (PPP)
7. Referral Transport
16. Programme Management
8. Service Delivery – Human Resource
17. IT Initiatives for strengthening service delivery
9. Training & Capacity Building
18. Innovations
Each budget annexure is linked to the budget summary sheet and the corresponding budget abstracts.
National Tuberculosis Elimination Programme (NTEP) is one of the many National Health Programmes that have come under the umbrella of the NHM. NTEP is now a flagship component of NHM and provides technical and managerial leadership to anti-tuberculosis activities in the country. NHM, in turn, is responsible for making funds available to carry NTEP related activities. The budget heads of NTEP may differ from other programmes. Hence, after the activities to achieve TB-elimination based on the Detect-Treat-Prevent Build strategies under National Strategic Plan (NSP) for TB Elimination 2017-2025 are planned, they have been aligned with the Financial Management Report (FMR) codes of NHM. This facilitates district, state, and central NHM to consolidate the individual PIPs for necessary approvals.
Resources
- E-Training Module on Budget/ PIP Preparation. National Health Mission. Ministry of Health and Family Welfare, Government of India.
- PIP Guidance Note 2018-19. National Health Mission, Ministry of Health and Family Welfare, Government of India.
- Training Modules (5-9) for Programme managers & medical officers, Central TB Division, Ministry of Health and Family Welfare, Government of India.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Budget heads of NTEP and other programmes under NHM are same.
True
False
2
The budget heads of NTEP may differ from other programmes.
Yes
Yes
NTEP Budget Heads
ContentThe National TB Elimination Programme (NTEP) expenditures are organised under 19 heads. These are:
1. Civil works - Initial establishment/ refurbishment costs and maintenance of civil works costs for Designated Microscopy Centres (DMC), Tuberculosis Units (TU), District TB Centres (DTC), Drug-resistant TB (DR-TB) centres and State Drug Stores (SDS).
2. Laboratory materials - Lab consumables for DMCs, Nucleic Acid Amplification Testing (NAAT), Culture and Drug Susceptibility Testing (C& DST) labs, State TB Training and Demonstration Centres (STDCs), National Reference Laboratories (NRLs) and Intermediate Reference Laboratories (IRLs).
3. Honorarium/ Counselling charges - Honorarium for community volunteers facilitating TB patient counselling and treatment.
4. Advocacy, Communication, Social Mobilisation (ACSM) - Various Information, Education and Communication (IEC) activities, patient-provider meetings, Active Case Finding (ACF)/ Intensive Case Finding (ICF) campaigning, etc. are budgeted under this head.
5. Equipment Maintenance - Maintenance and up-gradation costs for laboratory and office equipment.
6. Training - Training of State TB Officers (STOs), District TB Officers (DTOs), STDC faculty and all other cadres of NTEP staff (hiring of venue, organisation charges, honorarium for trainers, travel & dearness allowance, course material charges, refreshments, any other activities of training).
7. Vehicle Operation (POL and Maintenance)- Maintenance costs for all vehicles used for supervisory visits under NTEP. However, vehicle operation costs will not be available for hired vehicles. This will be applicable only for the department vehicles used under NTEP.
8. Vehicle Hiring - Vehicle hiring costs for supervisory visits by NTEP staff.
9. Public Private Mix (Patient-provider (PP) & Non-government Organisation (NGO) Support) - Payments of NGO/ PP schemes grant-in-aid, state and district level Public Private Mix (PPM) coordinators, TB health visitors, cost of pilots/ innovations for improving TB control.
10. Medical Colleges - Funds for referral, treatment, operational research, sensitization and advocacy among staff, faculty and medical students through state/ district health - TB control societies, funding for national, zonal and state task forces in medical colleges, their supervisory visits, etc.
11. Office Operation (Miscellaneous) - Funds for miscellaneous activities like electricity, janitorial expenses, internet cost, stationery, furniture, recruitment/ procurement advertisements, etc.
12. Contractual Services - For recruitment of various contractural staff under NTEP.
13. Printing - Printing of treatment cards, patient identity cards, TB register, lab form, referral form, notification form, health establishment registration form, research reports, action plans, training modules, other reporting formats, etc.
14. Research Studies and Consultancy - Proposals for research studies in specific domains, capacity building programs, consultancy charges for procurement of consumables, web-based reporting system development, etc.
15. Procurement of Drugs - Drugs for TB treatment.
16. Procurement of Vehicles - For purchase and replacement of four-wheelers and two-wheelers for field activities.
17. Procurement of Equipment - For procurement of various laboratory and office equipment.
18. Patient Support and Transportation Charges - Travel costs to patients from tribal/ hilly/ difficult areas, charges for sputum collection and transportation, multidrug-resistant TB suspect travel to District TB Centre (DTC) or collection centre for culture and drug sensitivity testing, etc.
19. Supervision and Monitoring - All activities for supervision, monitoring, evaluations, appraisals, and review meetings.
All activities a district could plan to achieve TB elimination based on the Detect-Treat-Prevent Build strategies under the National Strategic Plan for TB Elimination (2017-2025) can be described and budgeted under one of these heads.
Resources
- NTEP Training modules (5-9) for Programme Managers & Medical Officers, Central TB Division, Ministry of Health & Family Welfare, GoI, 2020.
- Financial Norms of RNTCP, Central TB Division, MoHFW, GoI.
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
ACSM activities have a separate budget head under NTEP.
True
False
1
ACSM activities have a separate budget head under NTEP. ACSM Annual action plan is an integral part of the annual district action plan for NTEP.
Yes
Yes
Principles of Preparing a realistic ACSM budget
ContentIt is important to create a realistic Advocacy, Communication and Social Mobilisation (ACSM) budget.
General principles which would be helpful in creating a realistic budget are:
- Enlist the goals intended to be achieved in the given time period
- Include pre-planning and intended activities
- Include break down of steps involved in each activity along with the resources required
- Partners should understand the overall budget for the activities as well as the budget for the respective components in which they are involved.
- Prioritise programme activities in case funding is reduced
- Follow the ACSM financial guidelines which are issued by the Central TB Division (CTD)
Make sure adequate funds are allocated for:
- Meeting and work space
- Formative research
- Material and product development (including pre-testing) and production
- Material distribution and storage
- Staff and consultants (specify the amount of time needed)
- Revisions to materials and activities, based on feedback from implementers
- Process and outcome evaluation
- Payment of external technical or creative experts as needed
- Miscellaneous costs of the partner organizations such as transportation, telephone and postage.
- Partner organizations can augment existing resources in various ways. For example, some partners might be able to contribute by photocopying materials while others may be able to donate office space for meetings. When planning ACSM activities, draw up a checklist of activities, products and other resources that might be needed. If the National TB Elimination Programme (NTEP) does not already have some of these services or items, identify potential organizations that might be willing to donate them.
- Both ACSM financial guidelines and the previous year’s budget utilisation should be kept in view as only 10–15 percent increase in budget allocation is the general norm. Bigger increases are uncommon and have to be explained with full justification. Hence, it is important to prioritise ACSM activities and prepare a realistic plan and budget estimation.
Table: Example of an Implementation Plan Format

The reason/ purpose for undertaking the ACSM activities is recorded in the last column of the Performance Improvement Plan (PIP) format.
Resources
- Advocacy, Communication & Social Mobilisation (ACSM) for Tuberculosis Control - A Handbook for Country Programmes, WHO, 2007.
- Operational Handbook on Advocacy, Communication & Social Mobilisation for RNTCP, Central TB Division, MoHFW, GoI, 2014.
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
A realistic ACSM budget includes allotment for process and outcome evaluation.
True
False
1
A realistic ACSM budget includes allotment for process and outcome evaluation.
Yes
Yes
ACSM planning format
ContentComponents of Advocacy, Communication and Social Mobilisation (ACSM) Planning Format
- Activity - The number of planned activities is mentioned against the timeline (for every quarter). Common activities listed in the format include community meetings, patient-provider meetings, school activities and outreach activities.
- Timeline - Timelines are divided into four quarters, but one must ensure that activities are spread across all the quarters and not aggregated in the last quarter of January–March.
- Budget - Budgeting for ACSM activities should cover materials, events, training, monitoring, evaluation, etc.
- Justification - The reason/ purpose for undertaking the ACSM activities is recorded.
The planning format also collects historical budgets proposed, allotted and spent for previous years to see if allotted budgets were properly utilised. The current allocation depends on the historical trend of spending.
Table: Example of ACSM Implementation Plan Format
Activity
Timeline
Budget
Justification/ Remarks
Q1
Q2
Q3
Q4
(Apr - June)
(July - Sep)
(Oct - Dec)
(Jan - Mar)
1. State Level
Image
Advocacy, Communication and Social Mobilisation
Justification/ Remarks
Activity
Budget Proposed in last annual action plan
(2012 – 2013)
Amount available in this Head (2012 – 2013)
Amount spent by district (2012 - 2013)
Approved ACSM Plan for 2013 -2014
Amount spent in 2013-2014 (till Sep 2013)
Permissible Budget as per population norm for 2014 - 2015
Budget proposed for 2013 - 2014
Total
0
Name of Activity
Number of activities undertaken in 2012-2013
Number of activities undertaken in 2013-2014 (till Sep 2013)
Number of Activities Proposed in 2014-15
Budget Proposed for Next FY 2014-2015
Apr-Jun
Jul-Sep
Oct-Dec
Jan-Mar
Total
Community meeting
0
Patient – provider meeting
0
School activity
0
Outreach activity
0
CME
0
0
0
0
Total
0
0
0
0
0
0
0
0
Resources
Assessment
Question
Answer
1
Answer 2 Answer 3 Answer 4 Correct answer Correct explanation How many components are there in the ACSM planning format? 3 4 5 2 2 Activity, Timeline, Budget and Justification are the key components of PIPs for ACSM. Developing ACSM Annual Action Plan
ContentThree Levels of Advocacy, Communication and Social Mobilisation (ACSM) Activities
- Preparation of district- and state-level Project Implementation Plans (PIPs) is an important component of the National TB Elimination Programme (NTEP) under the umbrella of the National Health Mission (NHM).
- State PIP is prepared annually which helps states in identifying and quantifying their targets for programme implementation during the year.
- This takes a bottom-up participatory approach that promotes need-based and decentralised planning.
Image
Figure 1: Bottom-up approach used in developing ACSM annual action plan
Steps in Planning ACSM PIP
- Draft of district PIPs are discussed in groups of 4–5 districts and ‘finalised’ as district PIPs.
- The district PIPs are consolidated into one document as the draft of state PIP by the IEC officer, in consultation with the STO and other concerned staff.
- In the process, the district PIPs and the state PIP are finalised and sent to Central TB Division (CTD) for approval.
- Once the state ACSM PIP and budget are approved by the CTD, the State IEC Officer (SIECO) should rework the state and district PIPs to reprioritise ACSM activities based on the allotted budget.
Image
Figure 2:Steps in Planning ACSM PIP
Abbr: DMC: Designated Microscopy Centre; PHI: Peripheral Health Institute; TU: TB Unit; DTO: District TB Officer; STO: State TB Officer; NTEP: National TB Elimination Programme.
Resources
Assessment
Question Answer
1
Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Planning of ACSM activities is a bottom-up approach. False True 2 ACSM project implementation plan takes inputs from all implementing levels - DMC, PHI, and TUs. Planning at the sub-district level starts as a bottom-up approach.
-
Fullscreen