-
CTP: TUBERCULOSIS
FullscreenTuberculosis
ContentTuberculosis (TB) is a communicable disease* that is a major cause of ill health, one of the top 10 causes of death worldwide and the leading cause of death from a single infectious agent (ranking above HIV/ AIDS).
TB is caused by the bacillus Mycobacterium tuberculosis, which is spread when people who are sick with TB expel bacteria into the air; for example, by coughing.
TB is a disease of poverty. Economic distress, vulnerability, marginalization, stigma and discrimination are often faced by people affected by TB.
TB is curable and preventable. About 85% of people who develop TB disease can be successfully treated with a 6-month drug regimen.
*Communicable diseases are diseases that can be spread from one person to another and cause a large number of people to get sick
Resources:
- Key facts on Tuberculosis: https://www.who.int/news-room/fact-sheets/detail/tuberculosis
Kindly provide your valuable feedback on the page to the link provided HERE
Burden of TB in India
ContentTB is one of the top burdensome infectious diseases in India. It is estimated that, around 1/4th (26%) of the world's TB cases are in India, translating to about 30 Lakhs new TB cases emerging each year (TB incidence). Against this estimated incidence the National TB Elimination program reported around 19 lakh new and relapse cases in the year 2021.
An estimated 5 Lakhs deaths occur due to TB each year in the country, translating to about 1 case of TB death every one-two minutes. Compared to this, there are only about 60 thousand deaths due to HIV and about 77 deaths due to Malaria each year.
TB diagnosis and treatment services although provided free of cost in the public sector, the cost of accessing these services and related loss of wages drive the affected people with poverty (catastrophic costs). TB also has a huge impact on the world's and the country's economy because of loss of workdays (100 million workdays per year).
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test What is the estimated number of incident TB cases that emerge each year in India? 35 Lakh cases 26 Lakh Cases 26% of the Global Burden 19 Lakh Cases 2 The estimated number of new and relapse (incident) cases in India that emerge each year is about 26 Lakh Yes Yes How many cases of deaths are estimated to be caused by TB in India Approximately One death every 2-3 minutes Approximately 5 Lakh deaths 60 Thousand deaths each year 1 and 2 4 In India it is estimated that there is around one death caused due to TB every one to two minutes, translating to about 5Lakh deaths each year in India Yes Yes Resources:
TB Causative organism
Content
Figure Mycobacterium tuberculosis
TB is caused due to the infection by a bacterium called Mycobacterium tuberculosis.

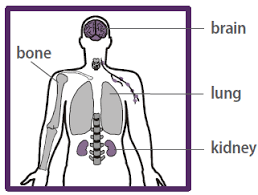
Figure: Extra-Pulmonary Tuberculosis
It often affects the lungs, and in such cases it is called Pulmonary Tuberculosis. But, it can affect almost any part of the body (except the hair and the nails), in which it is known as Extra-Pulmonary Tuberculosis.
Resources:
Mode of TB Transmission
ContentTuberculosis is transmitted mainly through the air via droplet nuclei generated when a TB patient coughs or sneezes.
It is estimated that every sputum smear-positive patient spreads the infection to 10 – 15 persons annually, if untreated..

Figure: Transmission of TB bacteria through air via droplet
Resources:
- Technical and Operational Guidelines for TB Control in India 2016
- WHO - Fact sheet details on Tuberculosis
Kindly provide your valuable feedback on the page to the link provided HERE
Determinants of TB Disease
ContentDeterminants are any characteristics that affect the health of a patient.
Biological Determinants Behavioral Determinants Socio Economic Determinants Occupational Determinants - People living with HIV(PL HIV)
- History of contact with a case of TB
- People with underlying medical conditions like Diabetes, Kidney disease, Cancer etc.
- Existing lung disease
- Old age
- Use of tobacco and alcohol
- Malnutrition
- Person in contact with TB infected patient
- Person living in areas with poor ventilation & over crowding
- Poverty and Malnutrition
- Homeless
- Mining work
- Quarry work(Silicosis)
- Construction work
- Migrant worker
- Daily wagers
Vulnerable Population for Tuberculosis
ContentTB can affect anyone but it is more prevalent in some communities which are vulnerable to TB disease due to various factors which are mentioned below:
Increased exposure of TB due to where they live or work
- prisoners
- slum dwellers
- miners
- hospital visitors
- healthcare workers
Limited access to Quality TB services
- Migrant workers
- Women in settings with gender disparity,
- Children
- Physically challenged
- Transgender population
- Tribal and population living in hard to reach areas
- Refugees or internally displaced people
- Illegal miners and undocumented migrants
Increased risk because of biological or behavioural factors that compromise immune functions in people who:
- People who live with HIV
- have diabetes or silicosis
- undergo immunosuppressive therapy
- are undernourished
- use tobacco
- suffer from alcohol use disorders.
- inject drugs
Progression to TB Disease
ContentAfter exposure to infective droplets containing M.TB, only a small proportion gets infected and further progresses to active TB disease.
- Majority of those that get infected persist in a stage of clinical latency known as TB infection (previously known as Latent TB infection). They do not have TB disease and do not show any symptoms of TB and no evidence of any TB related changes on chest X-ray.
- A small proportion of those with prior infection may progress to active TB disease due to various environmental/ agent/ host factors.

Figure: Flow chart for TB disease progression
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
TB Infection
Content-
TB Infection (or previously known as Latent TB infection) is a stage in between uninfected and having active TB. In this stage the person has no symptoms and can only be identified using laboratory tests.
-
The vast majority of infected people may never develop TB disease. However, to achieve TB elimination, it is important to treat TB infection in people at risk of developing active TB disease.
-
It is a state of persistent immune response to stimulation by Mycobacterium tuberculosis antigens with no evidence of clinically manifested active TB.
-
There is no single acceptable/reliable test for direct identification of Mycobacterium tuberculosis infection in humans. Tuberculin Skin Test (TST) and Interferon-gamma release assay (IGRA) are commonly used tests for identifying TB infection.
Resources:
-
TB Infection Vs Active TB Disease
ContentTB Infection Active TB Disease May not have any signs & symptoms Has sign and symptoms such as cough for more than two weeks, fever, weight loss and blood in sputum Has dormant, contained bacteria is the body Has active, multiplying bacteria in the body Doesn't spread TB bacteria to others May spread TB bacteria to others Chest X-ray usually normal Lesion in Chest X- ray (usually) May advance to active TB. It is estimated that the lifetime risk of an individual with TB infection for progression to active TB is 5–10%. Needs treatment for TB disease Resources:
Drug-Sensitive Tuberculosis(DS-TB)
ContentWhat is Drug-Sensitive Tuberculosis (DS-TB)?
-
DSTB is a case where a person is infected with TB bacteria that are susceptible to all first line anti-TB drugs. It means that all of the first line TB drugs will be effective as long as they are taken properly and regularly.
-
This type of TB has the best prognosis and the shortest treatment duration.
-
Patients diagnosed with TB are considered to be DS-TB case, till such time s/he detected with resistance to any anti-TB drugs.
Kindly provide your valuable feedback on the page to the link provided HERE
-
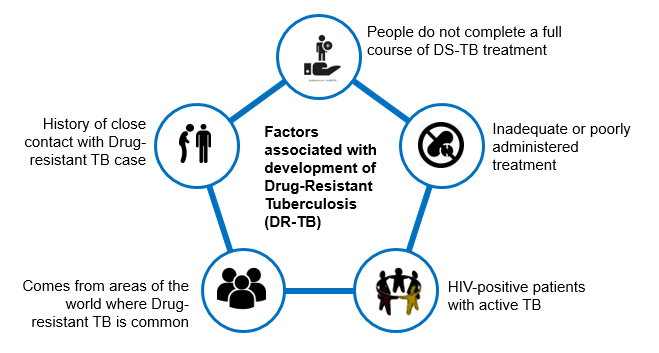
Drug-Resistant Tuberculosis(DR-TB)
ContentWhat is Drug-Resistant Tuberculosis?
-
Drug-Resistant TB occurs when bacteria become resistant to the drugs used to treat TB. This means that the drug can no longer kill the TB bacteria.
-
Multidrug-resistant TB (MDR TB) is a type of DR-TB where TB bacteria is resistant to both Isoniazid and Rifampicin, the two most potent anti-TB drugs.
Figure: High Risk for Drug-Resistant Tuberculosis (DRTB)
Resources:
-
Stages in TB Patient's Lifecycle
ContentThose who are suspected of having TB disease are first screened for symptoms like cough and fever for more than 2 weeks, blood stained sputum and weight-loss. If found positive on screening, then TB patients are referred for testing to the nearest health facility. If diagnosed with TB, then they are subsequently initiated on treatment. The TB patients initiated on treatment are regularly monitored with the help of field staff or digital interventions like 99DOTS and MERM (Medication Event Reminder Monitor) technology. NTEP staff also ensures that the TB patients are regularly followed up on monthly basis till their treatment completion.

Figure: Patient Flow
Kindly provide your valuable feedback on the page to the link provided HERE
Nikshay
ContentNikshay is an Integrated ICT system for TB patient management and care in India. Nikshay was launched in 2012 and since then, various improvements have been made in the system.
Nikshay provides-
- A Unified interface for public and private sector health care providers
- Different types of Logins such as State, District, TU, PHI, Staff logins, Private providers, Chemist, Labs and PPSA/JEET Logins
- Integration of all adherence technologies such as 99DOTS and MERM
- Unified DSTB and DRTB data entry forms
- Mobile friendly website with mobile app
Nikshay is accessible either via web browser(https://Nikshay.in ) or mobile App called ‘Nikshay’ that can be downloaded from Google Play Store(Android).
Figure: Nikshay Login Pages
TB Arogya Saathi Application
ContentTB Aarogya Sathi empowers Citizens (including TB Patients under NTEP) and to serve as a Direct interface with the national TB program.
Citizen: The App is aimed at increasing awareness among the citizens. It is available for all Citizens using the App (no login required to access this content)
- Information on TB (Symptoms, Side Effects)
- Health Facility Search
- BMI Assessment
- Nikshay Sampark Helpline
- Nutritional Advice
Patient: Patients registered with Nikshay will have access to the Adherence, Treatment Progress and DBT Details.
- Patients registered under Nikshay get access to their TB health record additional information (after login)
- Adherence Details
- Treatment Progress Details
- DBT Details
TB Aarogya Sathi App is available in Google play store and can be download using this QR Code


Figure: TB Aarogya Sathi Application snapshot
Resources:
-
CTP: TB DIAGNOSIS AND CASE FINDINGS
FullscreenSymptoms of TB Disease
ContentActive TB disease has 4 major symptoms (the 4 Symptom complex). Presence of any one of these symptoms without any other reason warrants evaluation for TB. These are:

Figure: Signs and Symptoms of TB
People affected with TB may experience other symptoms as well. These may be based on the site that is affected with TB or other more non-specific symptoms of an infection. The physician or doctor would evaluate these symptoms in view of diagnosis of TB.
Resources:
Presumptive TB
ContentPresumptive TB case refers to a patient who presents with symptoms or signs suggestive of TB disease (previously known as a TB suspect) and where further diagnostic workup including bacteriological investigation is required.
Presumptive TB can be categorized into
-
Presumptive Pulmonary TB (P TB) - Symptoms are directly related to lungs (Cough, hemoptysis)
-
Presumptive Extra Pulmonary TB (EP TB) - Symptoms/ signs are specific to an extra pulmonary site (example: Lymph node swelling)
-
Presumptive Pediatric TB - Symptoms of TB in young children are more difficult to identify and can be more general (fever, weight loss)
Resources:
- Technical and Operational Guidelines for TB Control in India 2016
- Definitions and reporting framework for tuberculosis
Kindly provide your valuable feedback on the page to the link provided HERE
-
Presumptive Pulmonary TB
ContentPulmonary TB(PTB) is primarily involves lungs. Screening should be done for the following symptoms:
Figure: Signs and Symptoms of active TB
Regular screening of Presumptive TB cases with unexplained cough of any duration should be done and checked for:
- History of close contact with known active TB case
- Whether the patient has developed Presumptive/confirmed extrapulmonary TB(EPTB)
- High-risk groups: PL HIV, Diabetics, Malnourished, Cancer patients, patients on immunosuppressive therapy or steroids
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Testing for TB diagnosis
ContentNational Tuberculosis Elimination Programme (NTEP) strives for all presumptive TB patients to be microbiologically confirmed. Under NTEP, the acceptable methods for microbiological diagnosis of TB are:
Sputum Smear Microscopy (for Acid Fast Bacilli - AFB): Sputum Smear microscopy is the primary tool which is reliable, inexpensive, easily accessible and rapid method of diagnosing PTB, where in the bacilli are demonstrated in the sputum. Two types:
-
Ziehl-Neelsen Staining
-
Fluorescence staining
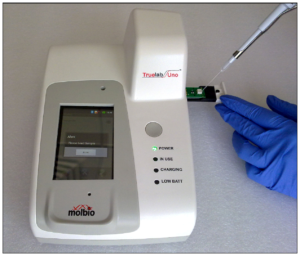
Rapid diagnostic molecular test: Rapid molecular tests that use techniques like NAAT are very specific. They amplify the genomic material in the patient sample and hence enhances detection
-
Nucleic Acid Amplification Test (NAAT) e.g., GeneXpert, TrueNat
Figure: Genxpert Machine for CBNAAT
Figure: Truenat Machine
- Line Probe Assay
Culture and DST: A culture test involves studying bacteria by growing the bacteria on different substances. This is to find out if particular bacteria are present. In the case of the TB culture test, the test is to see if the TB bacteria Mycobacterium tuberculosis, are present.
Two types:
-
Solid (Lowenstein Jensen) media
-
Liquid media (Middlebrook) e.g., Bactec MGIT etc.
-
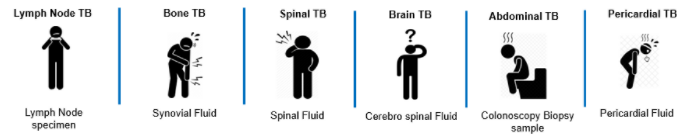
Biological Specimen for Diagnosis of TB
ContentFor laboratory diagnosis of TB, different biological specimens are used.
Pulmonary TB: Sputum sample is used. Sputum is a thick fluid produced in the lungs and in the adjacent airways. Normally, a spot sample and a fresh morning sample is preferred for the bacteriological examination of sputum.
Extra Pulmonary TB:
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Approaches to TB Case Finding
ContentPeople who have been exposed to patients with infectious TB are known as TB contacts; they constitute a high-risk group for TB. Case finding investigation contributes to the early detection of TB cases, and results in identifying a significant number of additional patients.
Figure: Approaches to Tuberculosis Case Finding
Active case-finding requires systematic screening and clinical evaluation of populations who are at high risk of developing TB, such as people living in slums, tribal areas, congregate settings, persons who are household contacts of TB cases
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Prevention of TB
ContentAs TB is an airborne infection, TB bacteria are released into the air when someone with infectious TB coughs or sneezes. The risk of infection can be reduced by taking simple precautions:
Figure: Measures for control and prevention of tuberculosis
TB Preventive Treatment(TPT) also has a very important role in prevention of TB. Presently, household contacts of sputum-positive TB patients are given TPT upon confirmation of TB infection and ruling our active Tuberculosis.
Resources:
-
CTP: TB TREATMENT AND CARE
FullscreenFirst line anti TB drugs
ContentFirst line drugs are the least toxic and most effective drugs that are used in first line of therapy.
The first-line antituberculosis drugs that form the core of treatment regimens are
Drugs Characteristics
Rifampicin (R)
Helps in early clearance of tuberculosis bacteria from the specimen
Isoniazid (H)
Most Powerful drug, that destroys all population of tuberculosis organism
Pyrazinamide (Z)
Kills or stops the growth of certain populations of TB bacilli
Ethambutol (E)
Prevents the growth of TB bacilli in association with other tuberculosis drugs to prevent emergence of resistant bacilli
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Treatment Phases
ContentStandard TB Treatment is divided into two phases
- Intensive Phase(IP): In this phase,
- Kills most of the TB bacteria during the first 8 weeks of treatment, but some bacteria can survive longer
- Therefore, more drugs are administered to kill the bacteria and reduce the severity of disease.
- Treatment in this phase usually is of short duration(2 to 6 Months or more) in comparison to Continuation Phase(CP)
- Continuation Phase(CP): In this phase,
- All the remaining TB bacteria are in the dormant stage i.e., stage when growth and development of bacteria are temporarily stopped.
- Therefore, fewer but powerful antibiotics are administered to kill those bacteria.
- Treatment in this phase usually lasts longer than Intensive Phase(IP)(4 to 18 Months or more)
Kindly provide your valuable feedback on the page to the link provided HERE
- Intensive Phase(IP): In this phase,
FDCs used in NTEP
ContentImage
Follow-up of TB patient
ContentTo know the TB treatment response and to determine that if patient is cured, TB patients are clinically evaluated at the end of every four weeks of treatment, and they are also followed up by performing sputum test at end of each treatment phase (i.e. Intensive phase and Continuation phase)
TB patients during clinical evaluations are assessed to
- Identify possible adverse reactions to medications;
- Check for any comorbid conditions;
- Weight change;
- monitor adherence; and determine treatment efficacy by observing their symptoms
Although each patient responds to treatment at a different pace, all TB symptoms should gradually improve and eventually go away.
Patients whose symptoms do not improve during the first 2 months of treatment, or whose symptoms worsen after improving initially, should be re-evaluated for adherence issues and development of drug resistance.
Long Term Post-treatment follow up of TB patients
ContentAfter completion of TB treatment, all patients should be followed up at the end of
- 6 months,
- 12 months,
- 18 months &
- 24 months
TB patients at the follow up should be screened for any clinical symptoms and/or cough. If found positive on screening, then sputum microscopy and/or culture should be considered. This is important in detecting the recurrence of TB at the earliest.
After completion of TB treatment, if the patient has not developed any clinical symptoms and/or cough and also if the microscopy remains negative during their follow up, then the patient is considered as “Relapse Free Cure from TB.”
TB Treatment Adherence
ContentTuberculosis(TB) is curable if patients are treated with effective, uninterrupted anti-tuberculous treatment. Treatment adherence is critical for curing individual patients, controlling the spread of infection in the community, and minimizing the development of drug resistance.
Adherence to treatment means that a patient follows the recommended course of treatment by taking all the prescribed medications for the entire length of time, as necessary. In other words, “right dose for the right duration”.
In Drug Sensitive Tuberculosis(DSTB), a TB patient completes 168 doses of TB treatment and adheres to TB treatment.
Importance of Treatment adherence
ContentAdherence to tuberculosis(TB) treatment is important for promoting individual and public health. Poor adherence to TB treatment results in:
- More individual suffering and death,
- Costly treatment as treatment regimens lengthen and
- Increases the risk for Drug Resistant Tuberculosis
Proper treatment of all forms of TB is critical to reducing individual morbidity and mortality and to interrupting transmission among family and community members.
Recording and Monitoring Adherence
ContentRecording of Treatment Adherence can be done as
- Manually by DOT/Health Care Provider in TB Treatment Card of a patient.
- Self-reported by Patient using digital tools for reporting adherence using 99 DOTS and MERM technologies.
Monitoring Treatment Adherence:
All TB patients should be monitored to assess their response to TB treatment. Nikshay Adherence calendar has a colour legend for various doses taken by a patient
Figure: Sample Nikshay Adherence Calendar in web and Mobile App
COLOUR LEGEND DOSE DESCRIPTION Treatment Start /End Denotes Treatment start and End Date Digitally Reported Dose Denotes that the patient has successfully called the Toll Free Number displayed on the envelope Manually Reported Dose Indicates that the staff has marked manually confirmed dose for the day Unreported Dose Indicates that there was no call event received on Nikshay for that day Manually Reported Missed Dose Indicates that the staff has marked a manually confirmed missed dose for the day Digitally Reported(From Shared Phone Number) Indicates that the patient has been calling from a shaed number(A mobile number that is common for more than one patient) Image
Figure: DSTB Treatment Card (Paper)
Fullscreen