-
CHO-CH10: General concepts in TB Treatment
FullscreenGoals of treatment
ContentThe goals of tuberculosis treatment are:
-
Rendering the patient non-infectious, breaking the chain of transmission and decreasing the infection pool
-
Decreasing case fatality and morbidity by ensuring relapse-free cure
-
Minimising and preventing the development of drug resistance.
To meet the goals of treatment, the regimens should be:
- Safe, easy to administer and aid treatment adherence
- Long enough to achieve the long-term cure of the disease, and short enough to increase patient compliance.
Any treatment regimen which reduces the pill count but increases the overall treatment success is an ideal regimen to meet the goals of tuberculosis treatment.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
In what scenarios is a TB treatment regimen considered efficient?
High sputum conversion
High treatment success
Low emergence of drug resistance
All of the above
4
The goal of TB treatment ties in with how we consider a regimen efficient, and this occurs when the regimen results in high sputum conversion and treatment success, and low relapse rates and emergence of drug resistance.
-
Treatment Phases
ContentStandard TB Treatment is divided into two phases
- Intensive Phase(IP): In this phase,
- Kills most of the TB bacteria during the first 8 weeks of treatment, but some bacteria can survive longer
- Therefore, more drugs are administered to kill the bacteria and reduce the severity of disease.
- Treatment in this phase usually is of short duration(2 to 6 Months or more) in comparison to Continuation Phase(CP)
- Continuation Phase(CP): In this phase,
- All the remaining TB bacteria are in the dormant stage i.e., stage when growth and development of bacteria are temporarily stopped.
- Therefore, fewer but powerful antibiotics are administered to kill those bacteria.
- Treatment in this phase usually lasts longer than Intensive Phase(IP)(4 to 18 Months or more)
Kindly provide your valuable feedback on the page to the link provided HERE
- Intensive Phase(IP): In this phase,
Fixed Dose Combinations [FDC]s
ContentFixed-dose combinations (FDCs) are drug formulations where two or more drugs are combined physically into one formulation such as a tablet or pill.
This is more convenient to the patients taking medicines and it also simplifies the supply chain.

Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Advantages of FDCs
ContentFixed-Dose Combination(FDC) provides a simple approach to deliver the correct number of drugs at the right dosage as all the necessary drugs are combined in a single tablet. By altering the number of pills according to the patient’s body weight, complete treatment is delivered without the need for calculation of dose
Figure: Advantages of Fixed Dose Combination(FDC)
FDCs used in NTEP
ContentImage
TB Drug Regimen
ContentA regimen means a prescribed systematic form of treatment for a course of drug(s). For TB treatment, Multi drug combination of regimen is followed.
All TB drug regimens have an initial intensive phase(IP) followed by a continuation phase(CP).
Following are some of the main TB drug regimens used based on the drug resistance pattern detected for TB patients.
- First-Line Anti TB Drugs(Prescribed for Drug Sensitive TB DS-TB)
- Daily weight band wise FDC
- Second-Line Anti TB Drugs (Prescribed for Drug Resistance TB - DR-TB)
- H Mono Poly Regimen
- Shorter oral Bedaquiline containing MDR-TB regimen
- Longer oral Bedaquiline containing regimen
- Shorter injectable containing MDR-TB regimen
- First-Line Anti TB Drugs(Prescribed for Drug Sensitive TB DS-TB)
TB Treatment Initiation
ContentThe Medical Officer (MO) of the referring health facility initiates TB treatment on receipt of the diagnostic test results. All efforts are made to initiate the treatment at the earliest.
The treatment regimen is decided based on the type of patient and TB (based on drug sensitivity pattern, i.e., drug-sensitive TB or H-mono/ poly resistance, history of adverse drug reaction to anti-TB drugs).
The patient needs constant support of a health volunteer or peer, who can monitor the treatment, help him in getting a follow-up, keep him motivated, counsel the family/ contacts, etc. These health volunteers/ peers are called treatment supporters in NTEP.
The steps in treatment initiation include:
- The MO performs a clinical evaluation of the patient and assesses for comorbidities.
- Counselling of TB patients and their families should be done.
- Peripheral health worker/ treatment supporters responsible for monitoring treatment adherence and treatment providers acceptable to the patient should be assigned.
- A treatment card should be opened for each patient.
- Each patient should be given a TB Identity Card.
- Drugs should be made available at the treatment centre.
- Public health action for all notified TB patients should be initiated.
All the process related to patient treatment initiation should be documented in Nikshay.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What key activities are included during TB treatment initiation?
Clinical evaluation
Counselling
Treatment card and TB ID card opened, Nikshay updated with treatment details
All the above
4
During TB treatment initiation the key activities include clinical evaluation of the patient; counselling of patient and family members; opening of treatment card and TB ID card and updating of treatment details on Nikshay.
Yes
Yes
Follow-up of TB patient
ContentTo know the TB treatment response and to determine that if patient is cured, TB patients are clinically evaluated at the end of every four weeks of treatment, and they are also followed up by performing sputum test at end of each treatment phase (i.e. Intensive phase and Continuation phase)
TB patients during clinical evaluations are assessed to
- Identify possible adverse reactions to medications;
- Check for any comorbid conditions;
- Weight change;
- monitor adherence; and determine treatment efficacy by observing their symptoms
Although each patient responds to treatment at a different pace, all TB symptoms should gradually improve and eventually go away.
Patients whose symptoms do not improve during the first 2 months of treatment, or whose symptoms worsen after improving initially, should be re-evaluated for adherence issues and development of drug resistance.
TB Treatment Outcome
ContentWhen a TB patient consumes all the doses under the prescribed regimen, then Treatment Outcome is declared for a Patient.
Treatment Outcome
Description
Cured
A TB patient who was microbiologically confirmed for TB at the beginning of treatment but who is smear or culture negative at the end of complete treatment
Treatment Complete
A TB patient who completed treatment without evidence of failure or clinical deterioration BUT with no record to show that the smear or culture results of biological specimen in the last month of treatment was negative, either because the test was not done or because the result is unavailable
Treatment Failure
A TB patient whose biological specimen is positive by smear or culture at the end of treatment
A case of paediatric TB who fails to have microbiological conversion to negative status or fails to respond clinically/or deteriorates after 4 weeks of compliant intensive phase shall be deemed to have failed response provided alternative diagnoses/reasons for non-response have been ruled out.
Loss to Follow up
A TB patient whose treatment was interrupted continuously for one month or more
Not Evaluated
A TB patient for whom no treatment outcome is assigned
Treatment Regimen Changed
A TB patient who is on first line regimen and has been diagnosed as having TB(DR-TB) and switched to DR-TB regimen prior to being declared as failed
Died
A patient who has died during anti-TB treatment(due to any reason)
Treatment success is considered when a TB patient either Cured or Treatment completed is accounted in treatment success
Closing Cases and Assigning Treatment Outcomes
ContentVideo fileVideo:
Closing Cases and Assigning Treatment Outcomes (Web)
Video fileVideo:
Closing Cases and Assigning Treatment Outcomes (Mobile)
Adverse Drug Reactions
ContentAdverse Drug Reactions(ADR) are unwanted or harmful reactions experienced following the use of a drug or combination of drugs and are suspected to be related to a drug. Severity of adverse effects varies from tolerable and mild ADRs to serious and life threatening ADRs.
Figure: Various Adverse Drug Reactions
Common ADR Symptoms:
- Pain in upper abdominal area, with loss of appetite
- Nausea – Uneasy feeling with inclination to vomit, after having the drugs
- Gastritis – Burning sensation in lower chest region, bloating sensation, sourness in mouth
- Diarrhoea - Loose stool(2-3 in a day)
Types of ADR of TB Treatment
ContentAdverse Drug Reactions(ADR) are classified into serious and non-serious ADR depending upon the intensity of symptoms experienced by the patient. Below is the brief overview
Common ADRs
Non-serious ADR
Serious ADR
(Refer to the nearest health facility)
Nausea and Vomiting
Symptoms of dehydration like thirst, dizziness, tiredness, dry mouth and eyes
- Extreme vomiting,
- Signs and symptoms of severe dehydration
- Blood in vomit
- Electrolyte imbalance and
- Altered level of consciousness
Gastritis and Pain in abdomen
- Occasional Discomfort
- Sour taste in mouth with acid reflux
- Burning sensation in upper abdominal region
- Severe pain in abdomen
- Acidity, Burping, Flatulence, Vomiting
- Blood in vomit
- Electrolyte imbalance and
- Altered level of consciousness.
Diarrhoea
2-3 /3-10 loose liquid stools with signs and symptoms of dehydration.
- More than 10 watery stools
- Signs and symptoms of dehydration
- Blood in stool
- Fever
- Intense abdominal pain
- Electrolyte imbalance and
- Altered level of consciousness
Tingling, Burning, Numbness in hands and feet
- Mild numbness and weakness in hands and feet.
- Prickling, stabbing, burning or tingling along with gradual increase in severity of numbness and weakness.
- Signs and symptoms of moderate neuropathy
- Extreme sensitivity to touch,
- Lack of coordination and balance
- Muscle Weakness
- Poor control of bowel and bladder
Pain in Joints
- Pain on touching joints
- Pain on walking, swelling and redness
- Warmth in and around joints
- Stiffness and signs of increased tenderness
- Severe weakness and restricted joint movement
Skin rashes, itchiness, and allergic reactions
•Itching and skin rashes with tingling and burning sensations
- Itching with increased size and raised wheels
- Swelling of lips and tongue
- Severe allergic reactions /Serious disorder of the skin with painful rashes /Shredding of skin.
Management of Adverse Drug Reactions(ADRs) of TB Treatment
Content- Counsel and reassure the patient as the common occurring adverse effects usually resolve with time.
- Advise the patient to take all the drugs together.
- Advise patient to take light meal (biscuits, bread, rice etc.) before taking drugs.
- Inform patients that they may take drugs embedded in banana or at the bedtime to reduce their associated side effects.
- Encourage patients to keep themselves hydrated by increasing fluid intake.
- Provide ORS (Oral Rehydration Solution) to counter dehydration due to loose motion and vomiting.
Figure: Referral to PHI for ADR
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Long Term Post-treatment follow up of TB patients
ContentAfter completion of TB treatment, all patients should be followed up at the end of
- 6 months,
- 12 months,
- 18 months &
- 24 months
TB patients at the follow up should be screened for any clinical symptoms and/or cough. If found positive on screening, then sputum microscopy and/or culture should be considered. This is important in detecting the recurrence of TB at the earliest.
After completion of TB treatment, if the patient has not developed any clinical symptoms and/or cough and also if the microscopy remains negative during their follow up, then the patient is considered as “Relapse Free Cure from TB.”
TB Treatment Card
ContentThe Tuberculosis Treatment Card is a paper-based recording form that is kept in the institution treating the TB patient under the National TB Elimination Programme (NTEP). It is a pre-requisite documentation related to treatment services offered to TB patients under NTEP.
Uses of the TB Treatment Card
The TB treatment card is primarily used for:
- Documenting administered drugs with their dosages
- Documenting follow-up investigation results
- Monitoring adherence to treatment
- Recording adverse events
- Recording treatment outcomes
There are two pages in the TB treatment card and details in each page is delineated in the table below.
Table: Parts of the Treatment Card; Source: NTEP Training Module 2 for Programme Managers & Medical Officers, p. 105
PAGE
DETAILS CONTAINED IN PAGE
The First Page
Patient details such as name, age, sex and address of the patient
Type of disease History of anti-TB treatment Regimen prescribed and duration of treatment Results of investigation before and during treatment Comorbidity-related information Contact tracing and chemoprophylaxis details Social habits such as tobacco and alcohol use The Back Page
Details of intensive and continuation phases of treatment including drug details and adherence monitoring
Retrieval actions for missing doses Adverse events Post treatment follow-up, nutritional support details and remarks Treatment outcome Important Points to Note
- The TB treatment card is filled at the Peripheral Health Institution (PHI) when a patient is initiated on treatment.
- The original TB treatment card is kept at the PHI and updated fortnightly.
- A duplicate treatment card is to be given to the treatment supporter for documentation of daily events.
- The treatment supporter should be trained on how to record the treatment card.
- Details on the patient’s HIV status are not included in the treatment supporter’s copy to maintain confidentiality.
The figure below shows the 1st page of the TB treatment card. Click here to access the full form in the NTEP Training Modules 1-4 for Programme Managers & Medical Officers, p. 223.
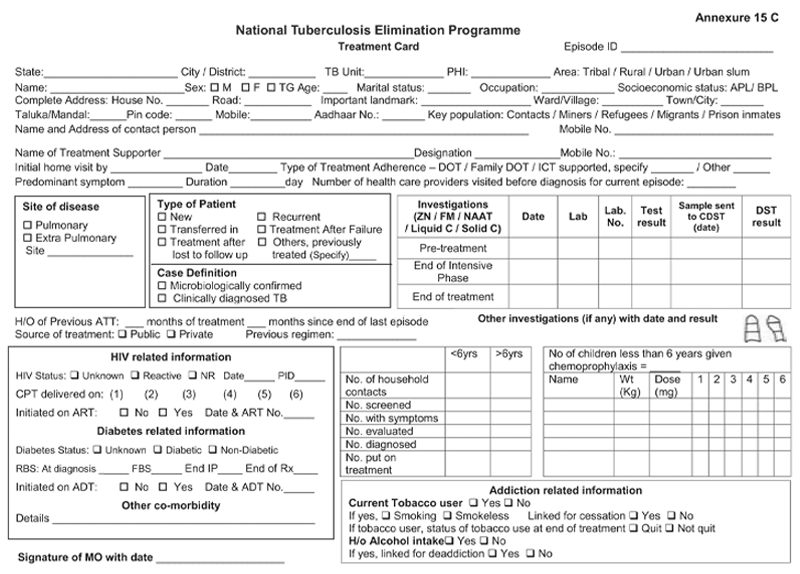
Figure: First Page of the TB Treatment Card; Source: NTEP Training Modules 1-4 for Programme Managers & Medical Officers, p. 223
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Transfer of TB Patient
ContentTB patients may not stay in one place throughout the treatment duration. When they move from one place to other, there should be a mechanism to hand over the responsibility of continuing the patient's treatment in a facility near the new place of the patient. This is the concept of patient transfer and can be easily managed in Nikshay portal.
- The transfer module in Nikshay enables transfer requests of patients between Health Facilities (HFs) across the country.
- Provision of shifting of patient from one HF to another is possible if the patient changes his/her residence for the purpose of treatment.
- The requests are of two types: “Transfer In” and “Transfer Out”.
- All transfer requests needs to be accepted by the “District/ TB Unit (TU)/ Peripheral Health Institute (PHI)” where the transfer request is made in order for it to take effect.
- Transfer requests can be made to even the District/ TU level. However, it can be completed only once the “Transferred to PHI” has been assigned.

Figure: Transfer Management in Nikshay; Source: Nikshay Zendesk, Nikshay Knowledge Base, Advanced Transfer in Web.
Steps in Transfer of TB Patient
1. In Nikshay, the referring HF updates details from the current HF of patient to the HF where patient is being transferred.
2. The receiving HF gets the intimation about the transfer.
The patient transfer module also provides the provision to pull the patient belonging to another HF to the recipient HF. The accountability of the transferred patients is now with the receiving HF and the treatment initiating facility.
A separate transfer register is also available to get details about various transfers from and to a given district, which can be downloaded from Nikshay reports.
Resources
- Nikshay Zendesk, Nikshay Knowledge Base, Advanced Transfer in Web.
- Guidelines for PMDT in India, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Transfer requests include "Transfer In" and "Transfer Out".
True
False
1
Transfer requests include "Transfer In" and "Transfer Out".
Yes
Yes
Follow up sputum examination
ContentFollow-up Sputum Examination is useful for the clinical follow-up which helps in assessing the response to treatment, and to establish cure or failure at the end of treatment.
Significance:
The most important tool in the diagnosis of tuberculosis is direct microscopic examination of appropriately stained sputum specimens for acid-fast bacilli (AFB). The technique is simple and inexpensive, and used in the detection of tuberculosis. Sputum microscopy is also useful for the clinical follow up which helps in assessing the response to treatment, and to establish cure or failure at the end of treatment.
Schedule
In case of Drug-sensitive Tuberculosis (DS-TB), the follow-up is done at the end of Intensive Phase (IP) and at the end of Continuation Phase (CP).
In case of Drug-resistant Tuberculosis (DR-TB), the follow up schedule is different for all the three regimen described below:
Isoniazid (H) mono/ poly DR-TB regimen
- Monthly from month 3 onwards, till the end of treatment
- Conduct sputum microscopy within 7 days, if the smear at month 4 or later is positive to rapidly ascertain bacteriological conversion/ reversion.
Shorter oral Bedaquiline-containing Multidrug-Resistant (MDR)/ Rifampicin-Resistant (RR)-TB regimen
- Monthly from 3rd month onwards, till end of IP
- Monthly in extended IP, only if previous month S+ve
- Conduct sputum microscopy within 7 days, if the smear at 6 months is positive to rapidly ascertain bacteriological conversion/ reversion.
Longer oral M/ XDR-TB regimen
- With culture at Culture and Drug Susceptibility (C&DST) lab
- Conduct sputum microscopy within 7 days if any smear at 6 month or later is positive to rapidly ascertain bacteriological conversion/ reversion.
After completion of treatment, the patients should be followed-up at the end of 6, 12, 18 & 24 months for detecting recurrence of TB at the earliest. In presence of any clinical symptoms and/or cough, sputum microscopy and/or culture should be considered. This is important in detecting recurrence of TB at the earliest.
Implications
The sputum follow-up examination is a quick and reliable method which helps in monitoring the progress of the treatment and gives an early indication of any recurrence.
ResourcesAssessment
-
CHO-CH11: DS-TB Treatment and care
FullscreenDrug-sensitive Tuberculosis
ContentWhat is Drug-Sensitive Tuberculosis (DS-TB)?
-
DSTB is a case where a person is infected with TB bacteria that are susceptible to all first line anti-TB drugs. It means that all of the first line TB drugs will be effective as long as they are taken properly and regularly.
-
This type of TB has the best prognosis and the shortest treatment duration.
-
Patients diagnosed with TB are considered to be DS-TB case, till such time s/he detected with resistance to any anti-TB drugs.
Kindly provide your valuable feedback on the page to the link provided HERE
-
Categorization of TB Treatment Regimen
ContentDaily Regimen is prescribed for TB patients, where patients need to consume the medicine daily.
Daily Regimen comprises of the first line Anti TB drugs, based on
- Age: Adult/Paediatric
- Weight of the patient: Weight Bands
Age: Based on the age, patients are categorized into
- Adults: Patient's age should be 19 years or more.
- Paediatrics: Patient's age up to 18 years and weight less than 39 Kgs
Weight Bands:
- Treatment dosage is based on the TB patient’s weight.
- A weight band category is defined for Adult and Paediatric patients separately and medicines are issued based on that weight category.
Treatment Regimen for DSTB – Adult
ContentIntensive Phase(IP): Consists of eight weeks (56 doses) of HRZE in daily dosages as per weight of patient.
Continuation Phase(CP): Consists of 16 weeks (112 doses) of HRE in daily dosages as per weight of patient.
For adults, there are five weight bands, as shown in the table below. The table also indicates the number of FDC tablets that have to be consumed in each weight band
Weight band category
Intensive phase(IP)
(HRZE - 75/150/400/275)
Continuation phase(CP)
(HRE - 75/150/275)
25–34 kgs
2
2
35–49 kgs
3
3
50–64 kgs
4
4
65–75 kgs
5
5
>=75 kgs
6
6
Regular monthly follow up of the patient needs to be done and if patient loses or gains approx. 5 kg weight and if weight band changes during the treatment, then the dose of the patient needs to be recalculated.
Treatment Regimen for DSTB - Pediatrics
ContentIntensive Phase (IP)
Consists of eight weeks (56 doses) of HRZ in daily dosages as per weight of patient.
Ethambutol (E) is given separately for children to monitor ophthalmic side effects.
Continuous Phase (CP)
Consists of 16 weeks (112 doses) of HRE in daily dosages as per the weight of the patient.
In Pediatric, there are six weight bands’s as shown in the table below. The table also indicates the number of FDC tablets that has to be consumed in each weight band
Weight Band category
Fixed-Dose Combinations (FDCs)
Intensive phase (IP)
(HRZE - 75/150/400/275)
Continuation phase (CP)
(HRE - 75/150/275)
4-7 kgs
1 1 8-11 kgs
2 2 12-15 kgs
3 3 16-24 Kgs
4 4 25-29 Kgs
3 + 1A 3 + 1A 30-39 Kgs
2 + 2A 2 + 2A Regular monthly follow-up of the paediatric patient needs to be done and if the patient weight crosses the range of the weight band during the treatment, then the weight band of the patient should be changed immediately.
Children above 39 kg shall usually be adolescents, the drug dosage requirement for them would be similar to adults
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Adverse Drug Reactions(ADRs) to First Line Treatment
ContentSymptoms
Drug Responsible
Action to be taken by Community Health Volunteers
Gastrointestinal Symptoms
Any Oral Medications
-
Reassure patient.
-
Give TB Drugs with less water at a longer interval.
-
If symptom persists, refer to the nearest health facility
Itching/Rashes
Isoniazid
-
Reassure patient.
-
In case of severe itching, refer the patient to the nearest health facility
Tingling/ burning/ numbness in the hands & feet
Isoniazid
-
Refer the patient to the nearest health facility
Joint Pains
Pyrazinamide
-
Reassure patient.
-
Increase intake of liquids.
-
If severe, refer the patient to the nearest health facility
Impaired Vision
Ethambutol
-
Refer the patient to the nearest health facility
Ringing in the ears, Loss of hearing, Dizziness and loss of balance
Isoniazid, Rifampicin or Pyrazinamide
-
Refer the patient to the nearest health facility
Hepatitis: Anorexia/ nausea/ vomiting/ jaundice
Isoniazid, Ethambutol, Rifampicin or Pyrazinamide
-
If patient detected with signs of jaundice, refer the patient to the nearest health facility
-
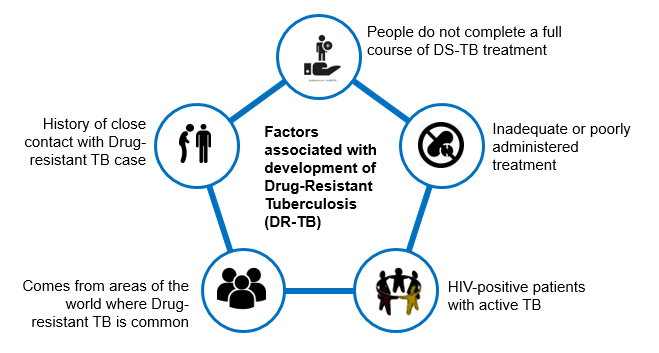
Drug-Resistant Tuberculosis(DR-TB)
ContentWhat is Drug-Resistant Tuberculosis?
-
Drug-Resistant TB occurs when bacteria become resistant to the drugs used to treat TB. This means that the drug can no longer kill the TB bacteria.
-
Multidrug-resistant TB (MDR TB) is a type of DR-TB where TB bacteria is resistant to both Isoniazid and Rifampicin, the two most potent anti-TB drugs.
Figure: High Risk for Drug-Resistant Tuberculosis (DRTB)
Resources:
-
Types of Drug Resistance Tuberculosis -DRTB
ContentResistant Sensitive
Unknown / Sensitive Types of Drug Resistance TB (DR TB) Resistance to Isoniazid (H) Resistance to Rifampicin (R) Resistance to Fluroquinolone (FQ)
- Ofloxacin,
- Levofloxacin,
- Moxifloxacin
Resistance to Group A Drugs
- Bedaquiline or
- Linezolid
H Mono / Poly Drug Resistance
- Resistant to Isoniazid (H)
- Sensitive to Rifampicin (R)
- Unknown / Sensitive to Fluoroquinolone (FQ) or Group A Drugs - Bedaquiline or Linezolid
Rifampicin Resistance (RR)
- Resistant to Rifampicin (R)
- Unknown / Sensitive to other drugs
Multi Drug Resistance TB (MDR TB)
- Resistant to Isoniazid (H) and Rifampicin (R)
- Unknown / Sensitive to Fluoroquinolone (FQ) or Group A Drugs - Bedaquiline or Linezolid
Pre-Extensive Drug Resistance (Pre -XDR)
-
Resistant to Isoniazid (H), Rifampicin (R) and any Fluroquinolone (FQ)
- Sensitive/ Unknown to Group A Drugs - Bedaquiline or Linezolid
Extensive Drug Resistance (XDR)
- Resistant to Isoniazid (H) , Rifampicin (R) and any Fluoroquinolone (FQ) and at least one additional Group A Drugs - (presently to either Bedaquiline or linezolid [or both])
Resources:
DR-TB Treatment Regimens
ContentDepending upon type of drug resistance, there are four broad DRTB Treatment regimen.
- H Mono/Poly Treatment Regimen(6-9 months)
- Shorter oral Bedaquiline containing MDR/RR-TB regimen(9-11 months)
- Shorter injectable containing regimen(9-11 months)
- Longer oral M/XDR-TB regimen(18-20 months)
Drugs administered for DRTB Regimen:
- Drugs are decided based on the drug resistance detected for a patient and will be informed by the medical officer.
- Injections might also be administered to the admitted patient.
- H Mono/Poly Regimen can be initiated at any health facility, while the other two regimen need to be initiated at N/DDR-TB Centre
Figure: Patient wise boxes(PWB) for DRTB Treatment
Pre treatment evaluation of a DRTB cases
ContentLet us understand the objective and importance of Pre-treatment Evaluation (PTE) of Drug-resistant TB (DR-TB) patients.PTE ObjectiveDrugs used for the treatment of drug-resistant TB have significant adverse effects. Hence, there is a need for PTE to rule out any underlying condition at the baseline, like co-morbid conditions, radiological abnormalities, Electrocardiogram (ECG) changes, or biochemical derangements.PTE is essential to identify:- The patient's eligibility for initiation of a particular regimen
- Patients who require special attention during treatment
- Regimen modifications from the beginning of treatment
Important Points
- In the majority of Multidrug-resistant (MDR)/ Rifampicin-resistant Tuberculosis (RR-TB) patients, PTE can be done on an outpatient basis.
- The District TB Officer (DTO) and Medical Officer of the TB Unit (MO-TU) can arrange for PTE at the Nodal and District DR-TB Centre (N/DDR-TBC) or at the sub-district level health facility, wherever feasible.
- No additional investigations are required for H Mono/ Poly DR-TB patients unless clinically indicated.
- The PTE carried out at the time of treatment initiation can be considered valid for 1 month from the date of the test result and the patient can be re-initiated on a subsequent regimen considering the previously conducted PTEs.
- Active Drug Safety Management and Monitoring (aDSM) treatment initiation forms are required to be completed for all DR-TB patients at the time of initiation of each new episode of treatment.
- PTE should include a thorough clinical evaluation by a physician and expert consultation as per the need.
- Laboratory-based tests should be performed based on the drugs used in the treatment regimen.
- Pre-treatment evaluation should be made available free of charge to the patient.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- WHO Consolidated Guidelines on Tuberculosis: Module 4 -Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Second Line anti TB drugs
ContentThe anti-TB drugs recommended for treatment of Multi- and Extensively Drug-resistant (M/XDR) TB patients are grouped into three groups – A, B and C (Figure below).
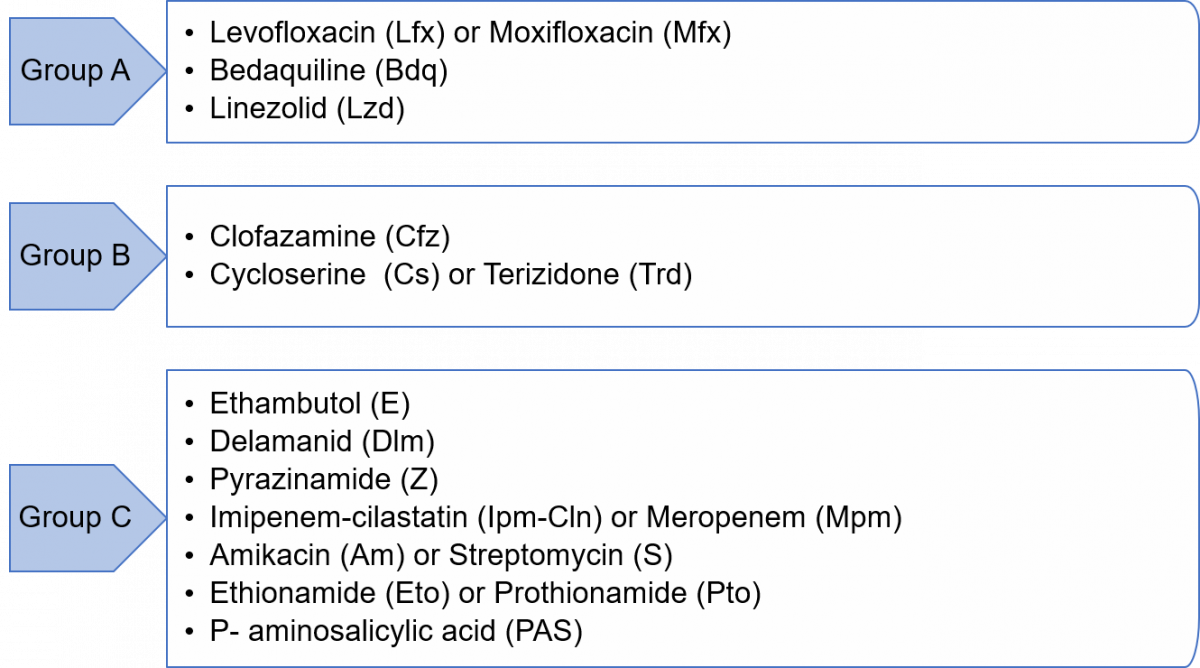
Figure: Groups A, B and C of Anti-TB Drugs used in Treatment of M/XDR-TB Patients
Grouping of drugs is done based on their efficacy, experience of use and drug class. This grouping is intended to guide the design of individualized, longer M/XDR-TB regimens (the composition of the recommended shorter MDR/RR-TB regimen is largely standardized).
Resources
- Guidelines for Programmatic Management of Tuberculosis in India, 2021.
- WHO Consolidated Guidelines on Tuberculosis, Module 4 - Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
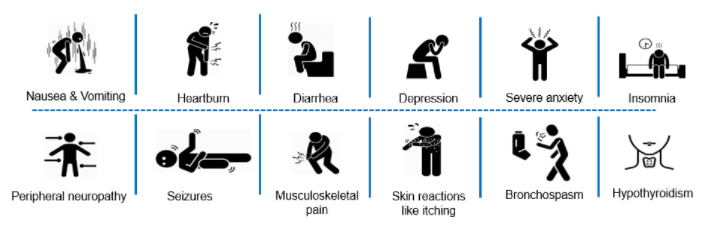
Adverse Drug Reactions(ADRs) to Second Line Treatment
ContentCommon Adverse events to second line treatment are as below
Figure: Adverse Drug Reaction to Second line drugs
Adverse events should be identified, monitored and be referred to
- Nearest treating doctor for minor symptoms or
- District DR-TB Centres for major symptoms
If required, hospitalization can be done at the District DR-TB Centers where inpatient facility is available or referred to a Nodal DRTB Centre for admission
-
CHO-CH12: TB Infection treatment and care
FullscreenTB Infection
Content-
TB Infection (or previously known as Latent TB infection) is a stage in between uninfected and having active TB. In this stage the person has no symptoms and can only be identified using laboratory tests.
-
The vast majority of infected people may never develop TB disease. However, to achieve TB elimination, it is important to treat TB infection in people at risk of developing active TB disease.
-
It is a state of persistent immune response to stimulation by Mycobacterium tuberculosis antigens with no evidence of clinically manifested active TB.
-
There is no single acceptable/reliable test for direct identification of Mycobacterium tuberculosis infection in humans. Tuberculin Skin Test (TST) and Interferon-gamma release assay (IGRA) are commonly used tests for identifying TB infection.
Resources:
-
Testing for TB Infection
ContentFor TB infection, there are two recommended tests which can be used to identify such patients.
Tuberculin Skin Test (TST)
The skin test is done by injecting a small amount (0.5 ml) of TB antigens into the top layer of skin on your inner forearm. If one has ever been exposed to TB bacteria (Mycobacterium tuberculosis), there will be a reaction indicated by the development of a firm red bump (induration) >= 10 mm at the site within 2 days.
Image
Figure: Tuberculin Skin Test
Interferon-gamma release assay (IGRA)
IGRA is a Blood test. If one has been exposed to TB bacteria, the white blood cell in the blood will release a substance called gamma interferon when the cells are exposed to specific TB antigens.
Image
Figure: Interferon-gamma release assay (IGRA)
Resources:
- Latent Tuberculosis Infection Guideline
- Guideline for Programmatic Management of Tuberculosis Preventive Treatment in India
Kindly provide your valuable feedback on the page to the link provided HERE
TB Preventive Therapy
ContentTPT treatment options recommended under NTEP include:
- 3-month weekly Isoniazid and Rifapentine (3HP)
- 6-months daily isoniazid (6H)

Table 1: TPT Options for Target Population; Source: (Guidelines for Programmatic Management of Tuberculosis Preventive Treatment)

Table 2: TPT dosage based on age and weight band recommended by NTEP; Source: Guidelines for Programmatic Management of Tuberculosis Preventive Treatment
Resources
- Guidelines for Programmatic Management of Tuberculosis Preventive Treatment
- National Strategic Plan for TB Elimination
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test TPT options recommended under NTEP include which of the following? 3-month weekly Isoniazid and Rifapentine (3HP) Rifampicin 6-months daily isoniazid (6H) 1 and 3 4 TPT options recommended under NTEP include 3-month weekly Isoniazid and Rifapentine (3HP) and 6-months daily isoniazid (6H). Yes Yes Counselling for TPT
ContentCounselling is of paramount importance for TB Preventive Treatment (TPT) initiation and completion as most of the target population screened and found eligible would know that they do not have TB disease, would be symptom-free or otherwise healthy and would not feel the need to take any treatment, especially Household Contacts (HHC).
Stakeholders Involved in Counselling for TPT (Figure below)

Figure: Stakeholders involved in counselling for TPT
Abbr: HWCs: Health and Wellness Centres; PHC: Primary Health Centre; ICTC: Integrated Counselling and Testing Centres; ART: Anti-retroviral Therapy; PLHIV: People Living with HIV
Components of Counselling for TPT
While counselling the person and family members, the treating doctors/ staff must follow the steps outlined in the table below for an effective counselling session.
Component
Actions to be taken
Confidentiality
Ensure confidentiality when seeking a person’s commitment to complete the course before initiating TPT.
Information
Provide information on:
- TB infection
- Need for TPT and protective benefits to the individual, household and wider community
- TPT is available free of charge under National Tuberculosis Elimination Programme (NTEP)
- TPT regimen prescribed, including duration, schedule of medication collection, and directions on how to take the medications
- Potential side-effects and adverse events involved and what to do in the event of various side-effects. People treated with rifamycins should be alerted in advance about the pink discolouration of secretions due to this medicine
- Importance of completing the full course of TPT
- Reasons and schedule of regular clinical and laboratory follow-up for treatment and monitoring
- Signs and symptoms of TB and advise on steps if they develop them
Medication adherence support
Agree on the best way to support treatment adherence, including the most suitable location for drug intake and the need for a treatment supporter, if required.
Family support
Involve family members and caregivers in health education when possible.
Openness
Invite clarification questions and provide clear and simple answers.
Information, Education and Communication materials
- Provide information materials in the local language and at the appropriate literacy level of the person concerned.
- Reinforce supportive educational messages at each contact during treatment.
Call support (in case of emergencies)
Provide a telephone number of the HCW staff/ TB Health Visitors and Senior Treatment Supervisors concerned to call for other queries or a need to contact health services for advice.
The National TB Elimination Programme (NTEP) national call centre (NIKSHAY SAMPARK – Toll-free number 1800116666) may be provided to index TB patients, those initiated on TPT and family members to serve as a resource for information, counselling and troubleshooting as required to enable TPT initiation, follow-up monitoring and completion.
Resources:
Guidelines for Programmatic Management of Tuberculosis Preventive Treatment in India.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following people are involved when counselling for TPT?
Index TB patients
Caregivers
Family members
All of the above
4
When counselling persons eligible for TPT, it is best to involve the index TB patients, their families and caregivers.
Yes Yes Monitoring adherence to TPT
ContentTo achieve high treatment completion rates and the desired epidemiological impact of the TB Preventive Treatment (TPT), monitoring TPT treatment adherence, including management of missed doses and Adverse Drug Reactions (ADRs), is of paramount importance under the National TB Elimination Programme (NTEP).
Significance of Monitoring Adherence to TPT
Adherence to the TPT course and treatment completion are important determinants of clinical benefit, both at the individual and population levels as:
- Irregular or inadequate treatment reduces the protective efficacy of the TPT regimen.
- Poor adherence or early cessation of TPT can potentially increase the risk of the individual developing TB, including drug-resistant TB.
- Efficacy of TPT is greatest if at least 80% of the doses are taken within the duration of the regimen. The total number of doses taken is also a key determinant of the extent of TB prevention.

Figure: Strategies to Promote Adherence
Prevent TB India App and Integration with Nikshay as a Monitoring Tool
- Currently, under the NTEP, the person’s lifecycle approach and TB treatment episode level are recorded in Nikshay.
- TPT information management is integrated with this existing Nikshay approach. This includes information on screening, testing, eligibility assessment, TPT initiation, adherence monitoring and follow-up till treatment completion.
- The NTEP has adapted the World Health Organisation (WHO) Prevent TB India app and hosted it on Nikshay as an interim solution till the Nikshay TPT module is developed and fully functional.
- Health workers or treatment supporters will make entries directly into the app.
- The TPT monitoring dashboard can be accessed by various levels of supervisors using their respective Nikshay login ids using a link provided in the Nikshay Reports section on TPT Reports.
- A web-based comprehensive dashboard for Prevent TB initiative is also available at https://ltbi.nikshay.in/ltbi-generic-new/#/
Table: Roles of Stakeholders in Monitoring Adherence to TPT Role
Stakeholder
Treatment support and adherence monitoring including entry of daily doses taken in the Prevent TB India app/ Nikshay TPT module.
Community volunteers (TB survivors/ champions, Accredited Social Health Activists (ASHAs) and Anganwadi Workers)
- Regularly undertake home visits or tele/ video calls to monitor TPT adherence.
- Identify treatment interruptions at the earliest (Dashboards of Prevent TB India app/ Nikshay TPT module may be checked every week along with pill counting).
- HWCs/ sub-centre/ urban health posts (Community Health Officers (CHOs), Auxillary Nurse Midwives (ANMs), multipurpose workers and other field staff)
- Primary Health Centres (PHCs)/ Urban PHCs/ Private clinic (Medical Officers (MO), staff nurse)
- Adherence support and clinical monitoring through the concerned PHC/ sub-centre.
- Supportive supervision and handholding support to field level facilities and frontline workers, ASHAs and community volunteers on digital recording, using Prevent TB India app and monitoring TPT and follow-up examinations.
TB Unit (MO, Laboratory Technicians (LTs), staff nurse, pharmacist, counsellor (if available), Senior Treatment Supervisors (STS), Senior TB Laboroary Supervisors (STLS), TB Health Visitors (TBHV))
Ensuring adherence support for People Living with HIV (PLHIV) on TPT through mechanisms such as outreach workers, PLHIV networks, peer support groups, etc.
Anti Retroviral Therapy (ART) centre/ Link ART centre (MO, pharmacist, (institutional) staff nurse, counsellor, care coordinator)
Monitor and support adherence to TPT.
Tertiary care/ Medical colleges/ Corporate hospitals/ District hospitals/ Dialysis/ Cancer facilities (doctors, staff nurses)
Review data updating in Prevent TB India app/ Nikshay TPT module wherever available, check the quality of data regularly and provide feedback to TPT treatment supporters and for retrieval of TPT interrupters.
Supervisory staff at all health facilities including the State/ District TB cell (State TB Officers (STO), District TB Officers (DTO), State/ District Programme Coordinators)
Resources:
- Guidelines for Programmatic Management of Tuberculosis Preventive Treatment.
- Prevent TB Dashboard.
- Prevent TB India Mobile App.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which tools are used to monitor TPT adherence under the NTEP?
Video calls
Counting empty blisters
Directly asking the patient
Options 1 and 2
4
TPT adherence monitoring tools include direct observation of drug intake, 99DOTS/ MERM, counting empty blisters, tele/ video calls and refill monitoring.
Which of the following apps are currently used by NTEP to monitor TPT adherence?
TB Aarogya Sathi
Prevent TB India App
TPT app for NTEP
None of the above
2
NTEP has adapted the WHO Prevent TB India app and hosted it on Nikshay to monitor the entire TPT care cascade, including TPT adherence.
-
CHO-CH13: TB-Comorbidities and special situations
FullscreenComorbidity & special situation with TB
ContentSeveral medical conditions are risk factors for TB and poor TB treatment outcomes. Similarly, TB can complicate the course of some diseases. Therefore, it is important to identify these comorbidities in people diagnosed with TB to ensure early diagnosis and improved outcomes. When these conditions are highly prevalent in the general population, they can significantly contribute to the TB burden. Consequently, reducing the prevalence of these conditions can help prevent TB.
TB shares underlying social determinants with many of these conditions. Addressing the social determinants of health is a shared responsibility across disease programmes and other stakeholders within and beyond the health sector.
Figure: Various comorbid and special situation related with tuberculosis
HIV in TB Patients
ContentThe primary impact of HIV on TB is that the risk of developing TB becomes higher in patients with HIV. Overall, HIV-infected persons have an approximately 8-times greater risk of TB than persons without HIV infection.
Screen TB PLHIV patients for symptoms of TB and HIV
Figure: Screening steps for TB - HIV patients
Treatment for TB HIV Patients
- All TB patients who have been diagnosed and registered under NTEP should be referred for screening for HIV.
- Referral of TB patients for screening for HIV and its recording & reporting is the responsibility of the Peripheral Health Institutions(PHI) where TB treatment is initiated.
- TB patients diagnosed with HIV will receive the same duration of TB treatment with daily regimen as non-HIV TB patients.
- TB patients must be referred to the nearest ART(Anti - Retroviral Treatment) centre for management of HIV.
Diabetes in TB Patients
ContentAs a consequence of urbanization as well as social and economic development, there has been a rapidly growing epidemic of Diabetes Mellitus(DM). India has the second largest number of diabetic people in the world.
Screen TB patients for symptoms of diabetes
Figure: Screening steps for TB - Diabetic Patients
Treatment for TB Diabetes Patients
- All TB patients who have been diagnosed and registered under NTEP will be referred for screening for Diabetes.
- Referral of TB patients for screening for DM and its recording & reporting is the responsibility of the Peripheral Health Institutions(PHI) where TB treatment is initiated.
- TB patients diagnosed with diabetes will receive the same duration of TB treatment with daily regimen as non-diabetic TB patients.
- TB patients must be referred to the nearest healthcare facility for management of DM.
- Regular monitoring of blood sugar levels is advised.
Malnutrition in TB Patients
ContentMalnutrition refers to deficiencies, excesses or imbalances in a person’s intake of energy and/or nutrients. The term malnutrition covers 2 broad groups of conditions.
- One is ‘undernutrition’—which includes stunting(low height for age), wasting(low weight for height), underweight(low weight for age) and micronutrient deficiencies or insufficiencies(a lack of important vitamins and minerals).
- The other is overweight, obesity and diet-related non communicable diseases (such as heart disease, stroke, diabetes, and cancer).
Screen TB Malnutrition patients for nutritional needs
Figure: Screening Steps for TB - Malnutrition patients
Treatment for TB Malnutrition Patients
Cases of TB with SAM and moderate undernutrition should be referred to the nearest health facility of NTEP for further management. Special focus should be given to the following categories:
- Children below five years
- School-age children and adolescents(Up to age 18 years)
- Adults, including pregnant and lactating women, with active TB and SAM
Alcoholism in TB Patients
ContentAbout 10% TB deaths globally have been attributed to alcohol as a risk factor(WHO, Global TB Report 2017). Alcohol abuse is associated with threefold increase in risk of contracting tuberculosis.
Side effects of anti TB drugs in this situation might get aggravated.
Figure: Impact of Alcoholism on TB patients
Treatment for Alcoholic TB Patients:
- Patients with TB and a history of alcohol use should be referred to the nearest health facility of NTEP to manage TB and alcoholism.
- While registering as a TB case, the status of alcohol use should be recorded in the patient records. If the TB patient is an alcohol user, he/she should be counselled to quit it. If the patient doesn't quit alcohol, s/he may be referred to the nearest alcohol de-addiction facility.
- The patient should be assessed at every follow-up visit for TB and the status of use of alcohol.
- At the end of treatment, his/her status of alcohol use should be recorded on the treatment card. If the patient has not quit alcohol, he/she should be referred to the nearest alcohol de-addiction facility and Alcohol Anonymous wherever available.
Tobacco in TB Patients
ContentAlmost 38% of TB deaths are associated with the use of tobacco. The prevalence of TB is three times higher among ever-smokers as compared to that of never-smokers. Mortality from TB is three to four times higher among ever-smokers as compared to never-smokers. Smoking contributes to 50% of male deaths in the 25-69 age group from TB in India.
Figure: Impact of Tobacco on TB patients
Treatment for TB - Tobacco Patients:
- While registering as a TB case, the status of tobacco use is recorded on the TB treatment card.
- If the TB patient is a smoker or tobacco user, he/she is counselled to quit tobacco use. The patient is assessed at every visit for follow up for TB and the status of tobacco use.
- At the end of treatment, his/her status of tobacco use is recorded in the treatment card. If the patient has not quit tobacco use, he/she will be referred to the nearest Tobacco Cessation Clinic(TCC) or Quit Line or M-Cessation Initiative.
Silicosis in TB Patients
ContentSilicosis is a progressive and disabling interstitial lung disease caused by inhalation and deposition in the lungs of particles of free silica.
Mutual Risk of TB and Silicosis
- TB is a clinical complication of silicosis, called silico-tuberculosis. Silica-exposed workers with or without silicosis are at increased risk for TB. There is also an increased risk of extrapulmonary TB in individuals exposed to silica.
- The risk of a patient with silicosis developing TB is 2.8 – 3.9 times higher than a healthy individual.
- The risk of TB relapse in patients with silicosis is approximately 1.5 times higher than in patients without silicosis.
The presence of silica particles in the lung and silicosis may:
- Facilitate initiation of TB infection and progression to active TB
- Exacerbate the course and outcome of TB, including prognosis and survival
Diagnosis
The diagnosis of silicosis is made based on a history of exposure to silica accompanied by a clinical and radiological profile consistent with the disease.
Under the Integrated Management Algorithm for TB disease and TB infection released by the National TB Elimination Programme (NTEP), patients with silicosis are first screened according to the four-symptom complex to rule out/in active TB and tested for TB accordingly.
If active TB is ruled out >> Refer for Tuberculin Skin Test (TST)/ Interferon Gamma Release Assay (IGRA) >> Positive test >> Evaluate with Chest X-ray (CXR) >> Commence TB Preventive Therapy (TPT) irrespective of CXR results.
CXR often indicates TB in silicosis patients earlier than the clinical symptoms, and regular radiographic screening is required for early TB detection. Radiographic comparison of serial films is done with particular attention to:
- Rapid appearance of new opacities, symmetric nodules or consolidation and the finding of pleural effusion or excavations.
- Cavitation is the strongest indicator of probable silico-tuberculosis.
Other diagnostic tools that can help in diagnosis are:
- Chest Computed Tomography (CT) scan
- Bronchoscopy with bronchoalveolar lavage in conjunction with transbronchial biopsy
- Spirometry
Treatment and Follow-up
To keep the disease from getting worse, all silicosis patients need to eliminate any more exposure to silica. Supportive measures include the use of cough medicines, bronchodilators, oxygen therapy and pulmonary rehabilitation.
TB treatment in patients with silicosis is challenging, perhaps due to impairment of macrophage function by free silica and/or poor drug penetration into fibrotic nodules. Usual anti-TB drugs with directly observed therapy are recommended but for an extended duration of at least 8 months, to reduce the chances of relapse.
Follow-up of patients with silicosis and TB follow the same schedule as is in prevailing guidelines.
Prevention
TB prevention in silicosis patients is essential and includes:
- Active surveillance of vulnerable groups including workers
- Adoption of measures to reduce exposure to silica dust
- Patients with silicosis are eligible for TPT after ruling out active TB
NTEP is in the process of engaging with the Ministry of Labour and Mining to identify high priority districts with stone crushing units/ mining industry. Specific guidelines will be developed to support persons with an occupational risk for TB and provide access, diagnosis and treatment services from the programme.
Resources
- NTEP at a Glance; Comprehensive Clinical Management Protocol of Tuberculosis, 2022.
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Silico-tuberculosis, Silicosis and Other Respiratory Morbidities Among Sandstone Mine-workers in Rajasthan - A Cross-sectional Study, Saranya Rajavel et al., 2020.
- Mini-review: Silico-tuberculosis; Massimiliano Lanzafame et al, 2021.
- Immunity to the Dual Threat of Silica Exposure and Mycobacterium tuberculosis, Petr Konečný et al., 2019.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following statement/s about silicosis and TB is/are incorrect?
TB is a clinical complication of silicosis, called silico-tuberculosis.
Silica-exposed workers with or without silicosis are at increased risk for TB and EPTB.
TB in patients with silicosis is easily diagnosed clinically as the patient coughs up silica particles.
TB treatment in patients with silicosis is often of extended duration to prevent relapse.
3
Clinical diagnosis of active TB superimposed on silicosis is often difficult, particularly in the initial phases, when clinical manifestations may not be indicative and radiological alterations can be indistinguishable from those due to the pre-existing silicosis.
Yes Yes Cancer in TB patients
ContentRelationship between Cancer and Tuberculosis (TB)
TB and malignancy may be related in the following four ways:
- TB as a marker for occult cancer: Occult cancer may lead to locally-reduced infection barriers and/or generalised immunosuppression, rendering a cancer patient susceptible to TB infection/ reactivation.
- TB as a risk factor for cancer: TB may increase the risk of cancer locally and systemically through chronic inflammation, fibrosis and production of carcinogenic molecules.
- Shared risk factors for TB and some cancers: Shared risk factors such as smoking, alcoholism, Chronic Obstructive Pulmonary Disease (COPD) and immunosuppression, including HIV, may lead to both TB and cancer, affecting both prevalent and subsequent cancer risk.
- Treatment of cancer-fueling TB: Many cancers are treated with immunosuppressants or steroids. These drugs might induce immunosuppression in the patients undergoing treatment for cancer and hence, a flare-up of TB.
Mutual Risk of Cancer and TB
- TB patients are 2-11 times more likely than non-TB patients to develop lung cancer, according to studies.
- After cancer diagnosis, the incidence of TB also increases, both in the short term and long-term.
- All types of cancer increase the risk of the development of active TB, but with varying degrees. Haematologic cancer patients had the highest rates of active TB, followed by head and neck cancers, lung cancer and breast cancer patients.
There is intrinsic immunosuppression due to the cancer itself, immunosuppressive effects of chemotherapy, or other host factors (e.g., smoking, malnutrition) that may increase the susceptibility to both cancer and TB. Thus, there is increased incidence of TB in cancer patients, and vice-versa.
Diagnosis of TB in Cancer Patients: Under the Integrated Management Algorithm for TB disease and TB infection released by the National TB Elimination Programme (NTEP), cancer patients are first screened according to the four-symptom complex to rule out/in active TB and all presumptive TB cases need to undergo testing for TB.
Co-existence of TB and cancer poses a diagnostic challenge since clinical and radiological presentations between TB and cancers are similar, hence the need for bidirectional screening. E.g., if biopsy specimens reveal infiltration by malignant cells, still send sample for microbiological confirmation of M. tuberculosis. Thus, allowing for accurate diagnosis and initiation of anti-TB treatment instead of attributing clinical deterioration to chemotherapy complications and progression of underlying malignancy.
Diagnosis of lung cancer in TB patients is usually done in consultation with a clinical specialist and can include examination of induced sputum specimens for malignant cells, as well as use of other diagnostic tools such as Computed Tomography (CT) scans, bronchoscopy, Positron Emission Tomography (PET) scans, Magnetic Resonance Imaging (MRI), histopathology and the use of biological markers.
Treatment
TB treatment in cancer patients uses the standard DS-TB/DR-TB regimens and course, except that the treating physician should assess the drug interactions between anti-TB and anti-cancer drugs. For cancer treatment, drugs may have to be modified to accommodate anti-TB treatment and to aid better prognosis of the TB outcome. However, all decisions must be taken by a competent specialist after examining the individual case.
Curative resection, chemotherapy and radiation therapy are the mainstay treatment options for cancer in TB patients. Co-existence of TB in cancer patients necessitates anti-TB treatment with extended duration, if required. Follow-up during and after treatment also follows prevailing guidelines.
Prevention
Under the NTEP, TB prevention in cancer patients is essential and includes:
- Regular screening for signs and symptoms of TB infection among all patients on immunosuppressive therapy and anti-Tumour Necrosis Factor (TNF) medicines.
- Education and referral of patients who do not have TB symptoms for TB infection testing/assessment of their eligibility for TPT.
Resources
- NTEP at a Glance; Comprehensive Clinical Management Protocol of Tuberculosis, 2022.
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Tuberculosis and Risk of Cancer: A Danish Nationwide Cohort Study, D. F. Simonsen et al., International Journal of Tuberculosis and Lung Diseases, The Union, 2014.
- Increased Risk of Active Tuberculosis after Cancer Diagnosis, Dennis F. Simonsen et al., Journal of Infection, 2017.
- Pulmonary Tuberculosis as Differential Diagnosis of Lung Cancer; MLB Bhatt et al., South Asian Journal of Cancer, 2012.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following statement/s about cancer and TB is/are incorrect?
Under NTEP, regular screening for signs and symptoms of TB infection among all patients on immunosuppressive therapy and anti-TNF medicines is done.
TB increases the risk of developing cancer, but cancer patients do not usually get TB.
Sputum smear microscopy is important when diagnosing TB in cancer patients.
All of the above
2
There is mutual risk between cancer and TB. TB increases the risk of developing cancer, and cancer patients are more likely to develop TB.
Yes Yes Pregnancy and Lactation in TB Patients
ContentThe presence of tuberculosis disease during pregnancy, delivery, and postpartum is known to result in unfavourable outcomes for both pregnant women and their infants. These outcomes include a roughly two-fold increased risk of preterm birth, low birth weight, intrauterine growth restriction, and a six-fold increase in perinatal death.
Screen TB patients in Pregnancy & Lactating Patients
Figure: Screening Steps in special situation - Pregnancy and Lactating TB Patients
Treatment for TB - Pregnant & Lactating Patients
- Cases of pregnant/lactating women with active TB should be referred to the nearest health facility of NTEP for further management.
- They should be continued on iron and folic acid and other vitamins and minerals to complement their maternal micronutrient needs.
- In situations when calcium intake is low, calcium supplementation is recommended as part of antenatal care.
COVID-19 in TB patients
ContentTuberculosis and COVID-19 are infectious diseases which primarily attack the lungs. They present with similar symptoms of cough, fever and difficulty in breathing, although TB disease has a longer incubation period and a slower onset of disease.
Screen patients for symptoms of TB and COVID-19
Figure: Screening steps for TB - COVID 19 Patients
Management of TB & COVID-19 Patients
People with TB are likely to be at increased risk of COVID-19 infection, illness and death. So, TB patients should take precautions as advised by health authorities to be protected from COVID-19 and continue their TB treatment as prescribed.
Prevention: While both TB and COVID-19 are spread by close contact between people, the exact mode of transmission differs. Thus, the patient should be explained the following measures to control disease spread.
- Apart from that keeping rooms well ventilated, avoiding crowds and Respiratory precautions are thus important in the control of COVID-19 and TB Disease
Fullscreen