-
CHO-CH5: Diagnostic Technologies
FullscreenTesting for TB diagnosis
ContentNational Tuberculosis Elimination Programme (NTEP) strives for all presumptive TB patients to be microbiologically confirmed. Under NTEP, the acceptable methods for microbiological diagnosis of TB are:
Sputum Smear Microscopy (for Acid Fast Bacilli - AFB): Sputum Smear microscopy is the primary tool which is reliable, inexpensive, easily accessible and rapid method of diagnosing PTB, where in the bacilli are demonstrated in the sputum. Two types:
-
Ziehl-Neelsen Staining
-
Fluorescence staining
Rapid diagnostic molecular test: Rapid molecular tests that use techniques like NAAT are very specific. They amplify the genomic material in the patient sample and hence enhances detection
-
Nucleic Acid Amplification Test (NAAT) e.g., GeneXpert, TrueNat
Figure: Genxpert Machine for CBNAAT
Figure: Truenat Machine
- Line Probe Assay
Culture and DST: A culture test involves studying bacteria by growing the bacteria on different substances. This is to find out if particular bacteria are present. In the case of the TB culture test, the test is to see if the TB bacteria Mycobacterium tuberculosis, are present.
Two types:
-
Solid (Lowenstein Jensen) media
-
Liquid media (Middlebrook) e.g., Bactec MGIT etc.
-
Cartridge Based Nucleic Acid Amplification Test [CBNAAT]
ContentCartridge Based Nucleic Acid Amplification Test (CBNAAT) is a rapid molecular diagnostic test. It is used for diagnosis of Tuberculosis (TB) and Rif-resistant Tuberculosis (RR-TB) in NTEP. Results are obtained from unprocessed sputum samples in about 2hours which helps in early detection and treatment of TB patients.
India has vast number of CBNAAT laboratories which are utilized for TB/RR-TB detection and Universal Drug Susceptibility Testing (UDST) under the National TB Elimination Program (NTEP).

Figure: CBNAAT Cartridge and Machine in Use (Image courtesy: USAID supported Challenge TB Project)
The CB-NAAT system detects DNA sequences specific for Mycobacterium tuberculosis complex and rifampicin resistance by Polymerase Chain Reaction (PCR). It concentrates Mycobacterium tuberculosis bacilli from sputum samples, isolates genomic material from the captured bacteria by sonication and subsequently amplifies the genomic DNA by PCR. The process identifies clinically relevant rifampicin resistance-inducing mutations in the RNA polymerase beta (rpoB) gene in the Mycobacterium tuberculosis genome in a real-time format using fluorescent probes called molecular beacons.
Video fileVideo: Cartridge-Based Nucleic Acid Amplification Test [CBNAAT] - GeneXpert Technology
Resources
- Training Module (1-4) for Program Managers and Medical Officers, NTEP, MoHFW, 2020.
- India TB Report 2021, National TB Elimination Program (NTEP), MoHFW, 2021.
Assessment Questions
Question
Answer 1
Answer 2
Answer3
Answer 4
Correct Answer
Correct explanation
Part of pre-test
Part of post-test
Under NTEP, CBNAAT is offered upfront for which of these categories?
PLHIV
Paediatric presumptive TB
Presumptive DR-TB
All of the above
4
Under NTEP, CBNAAT is recommended upfront for People living with HIV, Paediatric Presumptive TB patients, Presumptive DR-TB patients and patients notified from the Private sector.
Yes
Yes
CBNAAT requires the processing of sputum samples before testing
True
False
2
Results are obtained from unprocessed sputum samples in about 2hours from a CBNAAT machine
Yes
Yes
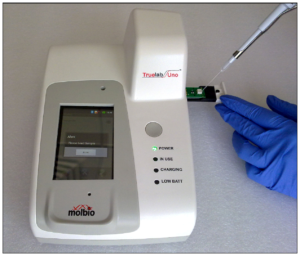
Truenat
ContentTruenat is an indigenous rapid molecular test platform that is currently under use in NTEP for diagnosis of TB and Rif Resistance. It is a platform utilising real-time Polymerase Chain Reaction (PCR) technology built into micro-PCR chips.
Testing on Truenat involves three components:
- Workstation (consisting of 2 devices)
- Trueprep AUTO Universal Cartridge-based Sample Prep Device for the automated extraction and purification of DNA
- Truelab Real-time micro PCR Analyzer for performing real-time PCR. It is available as 1 (Uno), 2 (Duo) or 4 (Quattro) chip ports.
- Cartridge and Chip
- Reagent kits (Sample Pre-treatment and Prep kits)

Figure: Truenat Source: MolBio Products.
Test results for MTB detection and Rif Resistance has a turn around time of 1-2 hours. Depending on the micro-PCR chips used various tests can be performed using Truenat. Truenat MTB micro-PCR chips detect Mycobacterium tuberculosis bacteria for TB diagnosis. Truenat MTB RIF micro-PCR chip is used as a reflex test to detect resistance to Rifampicin (RIF), the first-line drug for TB treatment
Truenat has many advantages. Truenat is designed to be mobile and is battery operated (~8 hours on full charge). It can be deployed in peripheral laboratories and microscopy centres with minimal or no added facilities and hence it is more point-of-care. Biosafety requirements are similar to smear microscopy. However, it is multi staged and partially automated, requiring the presence of a Lab Technician through out the test.
Resources
- Truenat MTB Kit Insert.
- Trueprep AUTO Universal Cartridge-based Sample Prep Device.
- Practical Guide to Implementation of Truenat Tests for the Detection of TB and Rifampicin-resistance, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Truenat is used in NTEP for: MTB detection Rif Resistance Detection INH resistance Detection MTB and Rif Resistance Detection 4 Truenat is used for MTB and Rif Resistance detection in NTEP Yes Yes The Truelab Analyzer is available in how many chip ports?
2 (Duo)
1 (Uno), 2 (Duo) and 4 (Quattro)
1 (Uno)
4 (Quattro)
2
The Truelab Analyzer is available as 1 (Uno), 2 (Duo) and 4 (Quattro) chip ports.
Yes Yes - Workstation (consisting of 2 devices)
Line Probe Assay [LPA]
ContentLine Probe Assay (LPA) is a rapid molecular test available at centralised laboratories.
The assay is based on Polymerase Chain Reaction (PCR) that can simultaneously detect Mycobacterium tuberculosis complex as well as drug sensitivity to anti-TB drugs.

Figure 1: The GenoType MTBDRplus Molecular LPA Procedure; Source: Molecular Detection of Drug-resistant Tuberculosis by Line Probe Assay.
Advantages of LPA
- Rapid molecular test. (Turnaround time: 3-5 days)
- Highly sensitive and specific.
- Performed directly from sputum smear-positive specimens and on isolates of M. tuberculosis complex grown from smear-negative and smear-positive specimens.
- Detects multiple gene mutations in anti-TB drugs.
- First-line LPA detects mutations to rifampicin and isoniazid
- Second-line LPA detects mutations to fluoroquinolones and aminoglycosides.
- Suitable for low and high-throughput labs.
Disadvantages of LPA
- Cannot be used as a point-of-care test.
- Requires appropriate laboratory infrastructure, equipment and biosafety precautions.
- Different rooms (DNA extraction, pre-amplification, amplification, post-amplification/ hybridization) are required to perform different steps (Figure 2).
- Requires trained manpower to perform tests and interpret test results.
- Stringent internal quality control is required to prevent contamination.

Figure 2: Amplification (A) and Post-amplification Laboratory (B) for LPA; Source: Molecular Detection of Drug-resistant Tuberculosis by Line Probe Assay.
Resources
- Guidelines for PMDT in India, 2021.
- Molecular Detection of Drug-resistant Tuberculosis by Line Probe Assay.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test LPA can be used as a point-of-care test. True False 2 LPA cannot be used as a point-of-care test. Yes Yes Solid and Liquid Culture in TB
ContentCulturing TB Bacilli is well known and historic method for detection/ confirmation of Tuberculosis. It is a highly sensitive and specific phenotypic test; it can detect even a few viable bacilli in the sample (Upto 10 Colony Forming Units- CFUs). TB bacilli multiply in the culture and form colonies of TB bacilli which can are easily be identified.
Based on the growth media used Culture is divided in to two types, Solid and Liquid Culture methods. Types Culture:
- Solid Culture on Lowenstein Jensen media : Historic gold standard culture test. Results take usually upto 2 months (60 days).
- Modern Liquid culture systems: (e.g. BACTEC MGIT 960, BacT Alert or Versatrek etc.) Results take usually up to 42 days.
Uses
- Solid culture is the gold standard diagnostic test for TB. But it is not used for the purpose of TB diagnosis due to the long turn around time of 2 months. It is largely used for research purposes where it is used as the baseline test on which the sensitivity and specificity of other tests are calculated.
- Liquid Culture is being used for follow-up monitoring of patients on drug resistant TB treatment to detect treatment failure. Liquid culture is also used for long term follow up patients who have successfully completed treatment to detect recurrence.
- Liquid culture is used as a previous step to grow bacilli and obtain isolates prior to Drug Susceptibility Testing.
- Liquid cultures are also used in TB prevalence surveys for its high sensitivity and specificity
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Culture Drug Susceptibility Testing [CDST]
ContentCulture Drug Susceptibility Testing (CDST) is a growth-based phenotypic method used to check the susceptibility of Mycobacterium tuberculosis strains to various first and second line anti-TB drugs. Mycobacterial resistance to a particular drug is identified if there is growth observed in culture in presence of that drug.

In NTEP CDST is the standard method to detect resistance in samples of patients who have tested positive on followup. While CDST is possible on both Solid and Liquid culture, currently, the NTEP utilizes only liquid culture as a method for DST, due to faster Turn around times.
CDST testing services are available under NTEP in designated, specialized laboratories called CDST Labs both in public and private sector. Currently there are 80 such laboratories (60 certified for First Line and 49 for Second line drugs). Such designated laboratories are subject to regular external quality assessment, often by the National Reference Laboratory at that region.
Quality assured DST to R, H, Z, Mfx, Lfx, Lzd, Am, Km and Cm are available across the country.
Resources
-
CHO-CH6: Dignostic Network and Hierarchy
FullscreenLaboratory Hierarchy and Network
ContentNTEP laboratory network is comprising of National Reference Laboratories (NRLs), state level Intermediate reference laboratories (IRLs), Culture & Drug Susceptibility Testing (C & DST) laboratories and peripheral level laboratories. Peripheral level laboratories consist of designated microscopy centres (DMCs) and NAAT labs.
NTEP has a quality assured laboratory network for bacteriological examination of sputum in a 3-tiered system.
Figure: Laboratory network of NTEP
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
NAAT Labs and their role
ContentThe National Tuberculosis (TB) Elimination Program (NTEP) has a network of Nucleic Acid Amplification Tests (NAAT) laboratories coupled with Designated Microscopy Centers (DMCs) to form the backbone of the diagnostic component of TB services.
Nucleic Acid Amplification Tests (NAAT) laboratories includes Cartridge-based NAAT (CBNAAT) and TrueNat tests. These tests detect tuberculosis as well as rifampicin resistance and are more sensitive than smear microscopy.
Functions of Nucleic Acid Amplification Test (NAAT) Laboratories:
- Acting as a hub for collection of samples from public and private health facilities (spokes)
- Universal Drug Susceptibility Testing (UDST) to rule out rifampicin resistance among confirmed TB patients
- Timely provision of NAAT test result to the TB patient, medical officer of the concerned health facility and NTEP staff for related actions
- Acting as a sample dispatch center for the Culture DST laboratory for subsequent processing of samples for first-line line probe assay (LPA) and second-line drug resistance testing utilizing second line LPA and liquid culture DST
- Recording and reporting including digitization of diagnostic process from collection to test result in NTEP Nikshay portal and Laboratory Information Management System
- Management of supplies and logistic associated with laboratory logistic (CBNAAT cartridges and TrueNAT chips) and reporting any additional requirement thereof
- Supporting the quality assurance activities undertaken by District or Intermediate Reference Laboratory under NTEP
- Support health system in carrying out special drives for vulnerable and at-risk population and their testing directly by CBNAAT (slum population, diabetic population, smoker, malnourished people, patients of silicosis and kidney dialysis etc.)
Resources
- RNTCP Technical and Operational Guidelines for TB Control in India, 2016.
- Guidelines for Programmatic Management of Drug Resistant Tuberculosis in India, 2021.
Kindly provide your valuable feedback on the page to the link provided HERE
Functions of a Designated Microscopy Centres [DMC]
ContentFunctions and Integrated Services of the DMC
- Testing of Sputum samples by Microscopy.
- Request/ referral for microscopy or Nucleic Acid Amplification Test (NAAT) or Culture and Drug Susceptibility Test (C&DST) or Chest X-ray (CXR) or Tuberculin Skin Test (TST) is generated at the PHI-DMC, as well as follow-up tests.
- Maintain consumables and logistics required for testing/ packaging and transport.
- Maintain TB laboratory registers for recording and reporting.
- Notify every TB patient in Nikshay at the earliest and update information of patients on comorbidity, treatment adherence, treatment outcome, contact investigation and TB Preventive Treatment (TPT).
- Biomedical waste management for the waste generated at DMCs.
- A DMC is required to participate in the External Quality Assurance system(EQA) of NTEP to ensure standardized quality diagnostic testing.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Sputum Collection centres
ContentTo increase access to diagnostic services, NTEP has a provision for sputum collection centres in areas where the health facility is not equipped with key requirements to conduct sputum microscopy, molecular tests, drug susceptibility testing or follow up examinations.
Sputum collection centres are dedicated locations where sputum samples are collected, packaged and then transported to nearby TB diagnostic centres. It could be attached to any near-by health-facility as well.
Requirements of a Sputum Collection Centre
To function as sputum collection centres, the following is essential:
- Linkage/ mapping (time and distance) to testing laboratory
- Availability of adequate number of sputum cups and falcon tubes, logistics for sample packaging and transport
- Identification of open areas for sputum collection
- Staff trained in NTEP guidelines on sputum collection, sample packaging and transport, complete and correct documentation of laboratory request form, and infection control practices
- Feasibility and financial measures required for sample transport
- Inclusion of local volunteers, courier services, sample transportation under National Health Mission Free Diagnostic Services or other mechanisms as decided by the state/district
- Availability of Information, Education and Communication (IEC) material, training modules, and job-aids
Sputum collection centres are established in:
- Ayushman Bharat Health and Wellness Centres/Sub-centres
- Urban primary health centres
- Tribal, hilly, desert and difficult-to-reach areas of the country
Resources
- Training Modules for Programme Managers and Medical Officers
- Operational Guidelines for TB Services at Ayushman Bharat Health and Wellness Centres
- Mycobacteriology Laboratory Manual, GLI Initiative, 2014
Assessment:
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Under NTEP, where are sputum collection centres established to increase access to diagnostic services? Tribal areas Ayushman Bharat health and wellness centres Difficult-to-reach areas All of the above 4 To increase access to diagnostic services, sputum collection centres are established in Ayushman Bharat health and wellness centres, Urban health centres, tribal, hilly, desert and difficult-to-reach areas of the country. Yes Yes
-
CHO-CH7: Approaches to TB Case Finding
FullscreenApproaches to TB Case Finding
ContentPeople who have been exposed to patients with infectious TB are known as TB contacts; they constitute a high-risk group for TB. Case finding investigation contributes to the early detection of TB cases, and results in identifying a significant number of additional patients.
Figure: Approaches to Tuberculosis Case Finding
Active case-finding requires systematic screening and clinical evaluation of populations who are at high risk of developing TB, such as people living in slums, tribal areas, congregate settings, persons who are household contacts of TB cases
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Active Case Finding
ContentSystematic screening of all individuals of a defined population is known as active case finding. It is applied outside of health facilities at the community level by the health system.
Objective of ACF is to:
- identify cases early, initiate prompt treatment, reduce risk of poor treatment outcomes and reduce risk of further transmission of TB
- to provide access to diagnosis services to populations that would have been otherwise unreached
It is effort intensive and is recommended only in population groups where there is estimated high case load. In NTEP, ACF is recommended only to be performed in Key / vulnerable population.
ACF can also be clubbed with suitable ACSM campaigns to create awareness about the signs and symptoms and about TB in the target population/ community. It can also be combined with other health activities/ campaigns (such as Pulse Polio/ Leprosy screening/ population based screening for NCDs) for increased efficiency.
Resources
- Training Modules for Programme Managers and Medical Officers.
- Active TB Case Finding, Guidance Document.
- WHO recommendations for Systematic Screening for Active Tuberculosis
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following is not a primary objective of ACF? Increase TB notification Early identification of cases. Reduce the risk of transmission of TB. Reduce the risk of poor treatment outcomes. 1 Notification is not a primary objective of ACF. Yes Yes Passive Case Finding
ContentPassive case finding is essentially where the patient self reports to the health care provider with symptoms. This requires that affected individuals are aware of their symptoms, have access to health facilities, and are evaluated by health workers or volunteers who recognise the symptoms of TB and link those individuals for TB testing services.
This approach to case finding has the least effort and cost and is a minimum expectation. In a Peripheral Health Institution (PHI), it is estimated that about 2-3% of new adult outpatients are symptomatic that require referral for TB diagnosis (presumptive TB cases).
Passive case finding may miss TB patients if :
- The disease is mild/ transient.
- Access to healthcare is poor.
- Health providers do not have an adequate index of suspicion and are unable to reliably link respiratory symptoms to TB.
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following can be considered a passive case finding? TB case finding for all patients attending an HIV clinic. TB case finding in all inmates of an elderly home. Patients attending a PHC with symptoms are referred for testing by the doctor. TB case finding among household contacts of a TB case. 3 All other examples except those attending PHC referred for TB testing are cases of active or intensified case finding effort. Yes Yes What may cause a passive case finding to miss cases? Healthcare providers fail to notify the case. Healthcare providers do not refer cases for TB testing. There are no health facilities in the area. Both 2 and 3 4 Healthcare providers failing to notify cases is missing notification and not related to passive case finding. Yes Yes Intensified Case Finding
ContentIntensified Case Finding (ICF) is a case finding approach between Active and Passive approaches. Here individuals coming in contact with the health system through any activity are screened actively for symptoms of TB and referred for testing.
This approach brings the benefit of active case finding approach by active screening for TB symptoms, but does limit the extensive effort required by restricting to only those people who has some or the other healthcare problem. This approach is considered for people attending a healthcare facility.
Some examples of ICF are screening for TB symptoms and referral for testing in:
- all cases attending an HIV clinic.
- among children with malnourishment who attend a nutrition clinic.
- all mothers attending the antenatal clinics
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following is an example of an intensified case finding?
Systematic screening for TB of all contacts of TB cases. Screening all cases attending an OPD with respiratory symptoms for TB testing. Referring cases that report more than 2 weeks of cough from an OPD for TB testing. Screening all people belonging to a slum for TB symptoms. 2 Systematic screening of TB contacts and those belonging to a slum population are examples of active case finding.
Referring to cases that report TB symptoms is a passive case finding.
Yes Yes Bidirectional Screening
ContentBidirectional screening is a method to identify cases in diseases which have predisposition to each other or has a significant influence on each other. For example TB and HIV, where having HIV increases risk of developing TB and cases with TB would have poor outcomes if co-infected with HIV.
Screening for TB is done through four-symptoms complex based screening or through Chest X-ray. Screening for the linked disease is carried out as per the policies of the corresponding health program.
Bi-directional screening policies are implemented by various disease control programs. For example, with NTEP the following disease control efforts implement a bidirectional screening policy:
- HIV through NACO
- COVID19
- Diabetes Mellitus (DM) through NPCDCS
- Tobacco through National Tobacco Control Program
Both programs monitor bidirectional screening, referral and testing as per their own policies.
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Bidirectional screening for TB is not done in which of the following conditions? Diabetes Tobacco abuse/ addiction Pregnancy COVID-19 3 Although pregnant mothers may be screened for TB as a part of intensified case finding, all TB cases are not actively/ routinely screened for pregnancy. Yes Yes
-
CHO-CH8: TB Case Finding in NTEP
FullscreenClassification of TB cases based on history of Previous TB treatment
Content- New case - A TB patient who has never had treatment for TB or has taken anti-TB drugs for less than one month is considered as a new case.
- Previously treated patients have received 1 month or more of anti-TB drugs in the past. They could be further classified as:
- Recurrent TB case - A TB patient previously declared as successfully treated(cured/treatment completed) and is subsequently found to be microbiologically confirmed TB case is a recurrent TB case.
- Treatment After failure patients are those who have previously been treated for TB and whose treatment failed at the end of their most recent course of treatment.
- Treatment after loss to follow-up A TB patient previously treated for TB for 1 month or more and was declared lost to follow-up in their most recent course of treatment and subsequently found microbiologically confirmed TB case
- Other previously treated patients are those who have previously been treated for TB but whose outcome after their most recent course of treatment is unknown or undocumented.
- Transferred In: A TB patient who is received for treatment in a Tuberculosis Unit, after registered for treatment in another TB unit is considered as a case of transfer in.
- Transferred Out : A patient who has been transferred to another recording and reporting unit and whose treatment outcome is unknown.
Classification of TB on the basis of Drug Resistance
ContentResistant Sensitive Unknown / Sensitive Types of Drug Resistance TB (DR TB) Resistant to Isoniazid (H) Rifampicin (R) Fluroquinolones (FQ) =
Ofloxacin, Levofloxacin,
MoxifloxacinGroup A Drugs =
Bedaquiline/ LinezolidH Mono / Poly Drug Resistance Resistant Sensitive Unknown/ Sensitive Unknown/ Sensitive Rifampicin Resistance (RR) Unknown/ Sensitive Resistant Unknown/ Sensitive Unknown/ Sensitive Multi Drug Resistance TB (MDR TB Resistant Resistant Unknown/ Sensitive Unknown/ Sensitive Pre-Extensive Drug Resistance (Pre -XDR) Resistant Resistant Resistant Unknown/ Sensitive Extensive Drug Resistance (XDR) Resistant
Resistant Resistant Resistant Resources:
Classification of TB on the basis of diagnosis
ContentOn the basis of diagnosis, Tuberculosis (TB) can be classified into 2 main types:
- Microbiologically confirmed TB
- Clinically diagnosed TB
Microbiologically Confirmed TB
- Microbiologically confirmed TB refers to a presumptive TB case from which a biological specimen is positive for acid-fast bacilli/ Mycobacterium tuberculosis on smear microscopy, culture, or on a rapid diagnostic molecular test (such as Cartridge-based Nucleic Acid Amplification Test (CBNAAT)/ Truenat).
- All such diagnosed cases should be notified at the source, regardless of whether TB treatment has started.
Clinically Diagnosed TB
- Clinically diagnosed TB refers to a presumptive TB case that is not microbiologically confirmed but has been diagnosed with active TB by a clinician who has decided to give the patient a full course of anti-TB treatment.
- This definition includes cases diagnosed on the basis of X-ray abnormalities or suggestive histology or extrapulmonary cases without laboratory confirmation.
- Clinically diagnosed cases subsequently found to be microbiologically positive (before or after starting treatment) should be reclassified as microbiologically confirmed.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Definitions and Reporting Framework for Tuberculosis, WHO, 2013.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test TB is classified on the basis of diagnosis into which of the following? Microbiologically confirmed TB and clinically diagnosed TB Mono-resistant TB and poly-resistant TB Recurrent cases and previously treated cases None of the above 1 TB can be classified on the basis of diagnosis into 2 main types: Microbiologically confirmed TB and Clinically diagnosed TB.
-
CHO-CH9: Active Case Finding Campaign
FullscreenACF campaign activities
ContentActive Case Finding (ACF) is a provider-initiated activity with the primary objective of detecting TB cases early by active case finding in targeted groups and to initiate treatment promptly.
- It can target people who anyway would have sought health care with or without symptoms or signs of TB and also people who do not seek care.
- Increased coverage can be achieved by focusing on clinically, socially and occupationally vulnerable populations.
- ACF activities in a campaign mode will create mass awareness about the signs and symptoms in general population
Objective of ACF campaign activities- Reaching the unreached in a campaign mode to enhance TB case finding

Figure 1: Objectives of active case finding
Beyond TB disease, screening can also identify individuals who are eligible for and would benefit from TB preventive treatment (TPT) once TB disease is ruled out, thus further averting future incident TB.
General process is as below:

Figure 2: ACF campaign general process
Resources
- WHO consolidated guidelines on tuberculosis: Module 2: Screening, Systematic screening for TB disease;WHO 2021
- India TB Report 2022, Central TB Division, MoHFW 2022
- Active TB Case Finding- Guidance document, Central TB Division & DGHS, MoHFW 2017
Assessment:
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test ACF will help in reducing spread of tuberculosis True False 1 ACF helps in early case detection & treatment initiation, thus reducing community level prevalence of TB disease & limit spread
Mapping the population for ACF
ContentMapping of vulnerable population is a pre-requisite for conducting an efficient ACF campaign. It involves understanding the population characteristics, identifying and enumerating and mapping the target population.
Guidelines for mapping
- Identify & map high risk/ vulnerable populations in the local area with the following guidance. If additional information is available locally, it can be used for the prioritisation of target groups.
Priority Urban area Rural area Tribal area
1 Slum Difficult to reach villages Difficult to reach villages & hamlets 2 Prisons inmates Mineworkers Villages with a known higher caseload 3 Old Age homes Stone crusher workers Tribal school hostels 4 Construction site workers Populations groups with known high malnutrition Areas with known high malnutrition 5 Refugee camps Populations known to drink raw milk Villages seeking care from traditional healers 6 Night shelters Populations known to eat uncooked meat Populations known to drink raw milk 7 NACO/SACS identified HRG for HIV NACO/ SACS identified HRG for HIV Populations known to eat uncooked meat 8 Homeless Weaving & Glass industrial workers Tribal areas with little ventilated huts 9 Street children Cotton mill workers 10 Orphanages Unorganised labour 11 Homes for destitute Tea garden workers 12 Asylums Villages largely seeking care from traditional healers 
Figure 1: Schematic map for house to house survey of identified vulnerable population
- Without proper mapping, there is a high chance of missing cases. The success of the active TB case finding campaign relies on how good the mapping is.
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test ACF campaign activities are done in all individuals of a defined area. True False 2 Symptom screening as part of the ACF campaign will be done in the identified and mapped target groups only (not in the general population).
Yes Yes Microplanning and execution of ACF campaign
ContentMicroplanning for ACF Campaign
A microplan is a detailed plan of action in terms of human resources, materials, money and time. A good microplan ensures that the health intervention reaches each individual beneficiary and is crucial to the success of the activity. For Active Case Finding (ACF), microplanning is performed at the health facility level and collated at the block, district and state levels. Training for the same is given to concerned personnel during state, district and block level meetings prior to the campaign. Microplan at PHI, Block, District and State levels should be ready at least 15 days prior to the initiation of field activities.
Microplanning is done with respect to:
I. Advocacy, Communication and Social Mobilization (ACSM)
A comprehensive IEC plan should be made with communication material for mass media, mid-media and print media to reach out up to the remotest village in advance.
II. Logistics
- Microplan should include planning additional consumables required for the campaign
- It includes additional slides, laboratory reagents, sputum cups, falcon tubes, sample transport boxes, X-ray films, Cartridge-based Nucleic Acid Amplification Test (CBNAAT) cartridges, etc. Additional sputum containers (minimum 1000 per lakh population) will be procured and supplied to health staff for collecting sputum sample from the eligible symptomatic two weeks before the start of field activities
- Linkages of Peripheral Health Institute (PHI) areas with Designated Microscopy Centre (DMC), X-ray facilities, CBNAAT lab, Extra Pulmonary (EP) sample collection and EP testing should be included in the planning up-front.
- Laboratory technicians of the linked DMC and CBNAAT labs should be well informed about the increase in workload and recording of information during ACF activities.
III. Field activities including human resources
- Maps prepared for other campaigns like Pulse Polio, Leprosy Case Detection Campaign (LCDC), etc. must be used while planning. If maps are not available with local bodies, search team members and supervisors should be sent to the area before the ACF campaign, in order to become familiar with the area and develop maps.
- The number of houses to be covered each day should be mentioned in the microplan. This number may vary from day to day depending upon the geographical situation of the area planned to be covered by the team on a particular day.
- Teams of two persons each should go house-to-house. Out of the two members in each team, one should be a local volunteer (including Accredited Social Health Activist (ASHA)).
- Each team should be allocated clear-cut, well-demarcated areas clearly mentioning the starting and ending points, identifiable with landmarks; for each day of House to House (h-t-h) activity.
- In special areas, one additional person from the local community, where the team will be working, should accompany the team.
- Human resources required for covering the mapped vulnerable population during field activities should be calculated and recorded.
- For planning and implementation purposes, urban areas should be divided into smaller planning units based on municipal wards or assemblies, or by roads or prominent landmarks. Each such unit should be put under the charge of a medical officer or nodal officer.
- Involvement of the local community, leaders, health officials, municipal bodies and their staff is essential in planning.
- Local staff is familiar with the layout of the urban areas and their inputs are vital for planning and supervision of house-to-house activities.
Execution of Microplan
The ACF campaign is executed as per the microplan and supervision is done with reference to the microplan
The House to House (h-t-h) survey is done for 2 weeks
A survey team consisting of 2 persons - one NTEP staff/ partner organization staff/ General Health services staff and one local volunteer / ASHA worker. They go from house to house in the mapped vulnerable areas/ key population groups and screen individuals for symptoms of TB. After screening, the eligible population for sputum examination includes: Persistent cough for ≥2 weeks, Fever for ≥2 weeks, Significant weight loss (>5% weight loss over last 3 months), Presence of blood in sputum any time during the last 6 months, Chest pain in the last one month, History of Anti-TB Treatment (previous/ current). If any one of these is present, a sputum cup or falcon tube is given to them and a sputum sample is collected. Sputum samples thus collected are transported to a designated lab using the sample transport system existing in the area. testing using smear microscopy/CBNAAT will be done for all symptomatic persons as per the state policy. Those who are microbiologically confirmed to be positive should be initiated on treatment within 2 days. Additionally, the team will look for other symptoms/diseases also. If person is having any symptoms or other ill health, s/he will be referred for evaluation by a Medical Officer for further management, if needed. Field Activity Report will be submitted by each health staff on a daily basis to the Medical Officer of the Peripheral Health Institution
Resources
- Active TB Case Finding – Guidance Document, 2017, Central TB Division, MoHWF, New Delhi.
- Active Case Finding for Tuberculosis in India: A Syntheses of Activities and Outcomes Reported by the National Tuberculosis Elimination Programme, Burugina Nagaraja S et al, Trop Med Infect Dis., 2021.
Assessment
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Which of the following is wrong about microplanning in ACF?
Microplan is first made at the state level. It is a detailed plan of the human resources, logistics and field activities required in the ACF campaign.
A good microplan is important for the success of the ACF campaign.
Supervision of field activities is done with reference to the microplan.
1
Microplan is made at the health facility level and then collated at subsequent levels.
Yes
Yes
Recording formats under ACF campaign
ContentVulnerability mapping and Microplanning are 2 important activities of Active Case Finding which precede field activities. Vulnerable populations should be mapped and recorded in prescribed formats from health facility level onwards. Mapping data from PHI are consolidated at Block level, those at Block level are consolidated at district level and those at district level are consolidated at state level. Data from mapping formats is used for microplanning. Microplanning forms the basis of field activities. Microplans are also consolidated at subsequent levels. During supervision and monitoring, it is important to assess the activities with respect to the microplan.
The recording formats for ACF include:
1. Formats for mapping - Health Facility Level, Block Level, District Level and State Level
2. Formats for microplanning - Manpower, Logistics, Field Activity
FORMATS FOR MAPPING





Mapping details should also be entered in Ni-kshay under the section shown below:
Image
Fig: Ni-kshay section for reporting various ACF activities
FORMATS FOR MICROPLANNING
Based on the requirement obtained from the mapping exercise, microplanning is done with respect to human resource, logistics and field activities
Human Resource Planning Form



Field activities are captured in Form 1 & 2 of the ACF. The data from field activities are compiled at the PHI level and submitted to the District and State using google sheets at present. Although there is no specific mechanism to demarcate the presumptive TB patients and the confirmed (clinical and microbiological) TB cases in Ni-kshay, States follow different mechanism including marking in the Laboratory register as ACF testing and sending a separate sheet to the district in paper format.
Reference:
1. Active TB Case Finding - Guidance Document, Central TB Division & DGHS, MoHFW, 2017
Assessment:
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Vulnerability mapping and microplans for ACF should be recorded at
Health facility level
District level
State level
All the above
4
Mapping activities should be recorded at health facility level and consolidated at subsequent levels (district, state, etc)
Yes
Yes
Fullscreen