Drug-Resistant Tuberculosis(DR-TB)
ContentWhat is Drug-Resistant Tuberculosis?
-
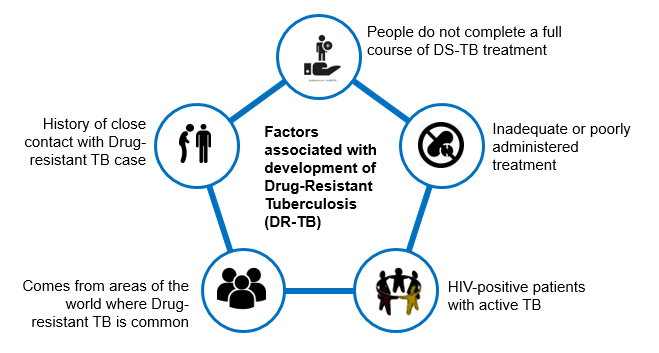
Drug-Resistant TB occurs when bacteria become resistant to the drugs used to treat TB. This means that the drug can no longer kill the TB bacteria.
-
Multidrug-resistant TB (MDR TB) is a type of DR-TB where TB bacteria is resistant to both Isoniazid and Rifampicin, the two most potent anti-TB drugs.
Figure: High Risk for Drug-Resistant Tuberculosis (DRTB)
Resources:
-
Types of Drug Resistance Tuberculosis -DRTB
ContentResistant Sensitive
Unknown / Sensitive Types of Drug Resistance TB (DR TB) Resistance to Isoniazid (H) Resistance to Rifampicin (R) Resistance to Fluroquinolone (FQ)
- Ofloxacin,
- Levofloxacin,
- Moxifloxacin
Resistance to Group A Drugs
- Bedaquiline or
- Linezolid
H Mono / Poly Drug Resistance
- Resistant to Isoniazid (H)
- Sensitive to Rifampicin (R)
- Unknown / Sensitive to Fluoroquinolone (FQ) or Group A Drugs - Bedaquiline or Linezolid
Rifampicin Resistance (RR)
- Resistant to Rifampicin (R)
- Unknown / Sensitive to other drugs
Multi Drug Resistance TB (MDR TB)
- Resistant to Isoniazid (H) and Rifampicin (R)
- Unknown / Sensitive to Fluoroquinolone (FQ) or Group A Drugs - Bedaquiline or Linezolid
Pre-Extensive Drug Resistance (Pre -XDR)
-
Resistant to Isoniazid (H), Rifampicin (R) and any Fluroquinolone (FQ)
- Sensitive/ Unknown to Group A Drugs - Bedaquiline or Linezolid
Extensive Drug Resistance (XDR)
- Resistant to Isoniazid (H) , Rifampicin (R) and any Fluoroquinolone (FQ) and at least one additional Group A Drugs - (presently to either Bedaquiline or linezolid [or both])
Resources:
Goals of DR-TB Treatment
ContentGoals of Drug-resistant Tuberculosis (DR-TB) treatment under the National Tuberculosis Elimination Program (NTEP) are as follows:
Image

Figure: Goals of DR-TB Treatment; Source: Guidelines for PMDT in India, March 2021, p41.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- Technical and Operational Guidelines for TB in India, 2016.
Kindly provide your valuable feedback on the page to the link provided HERE
Newer Anti-TB Drugs
Content
Figure: Sirturo 100 mg Bedaquiline Tablets
- Newer anti-TB drugs are needed to improve the treatment outcomes of DR-TB, shorten the duration of treatment, address the problem of drug resistance, and have less toxic drugs.
- Five decades after the discovery of Rifampicin, two newer drugs with anti-TB effects were approved for the treatment of multidrug-resistant tuberculosis (MDR-TB) by the Central Drugs Standard Control Organization (CDSCO). These are:
- Bedaquiline (Bdq)
- Delamanid (Dlm)
- In July 2020, the Drug Controller General of India (DCGI) also approved a third newer drug - Pretomanid (Pa) to use under the Conditional Access Programme (CAP) under the National Tuberculosis Elimination Program (NTEP).
Resources
- The Use of Bedaquiline in the Treatment of Multidrug-resistant Tuberculosis, Interim Policy Guidance, WHO, 2013.
- The Use of Delamanid in the Treatment of Multidrug-resistant Tuberculosis in Children and Adolescents, Interim Policy Guidance, WHO, 2016.
- WHO Consolidated Guidelines on Tuberculosis, Module 4: Treatment- Drug-resistant TB Treatment.
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
Kindly provide your valuable feedback on the page to the link provided HERE
Weight Band-wise Dosages of DR-TB Drugs for Adults
ContentThe dosage for Drug-resistant TB (DR-TB) drugs used in the regimen by weight bands for adults are enumerated in the table below.
Table: Weight Band-wise Drug Dosage of DR-TB Drugs for Adults; Source: Guidelines for PMDT, India 2021, pp.51,64. SR NO
DRUGS 16-29 KG 30-45 KG 46-70 KG >70 KG 1 Levofloxacin (Lfx) 250 mg 750 mg 1000 mg 1000 mg 2 Moxifloxacin (Mfx) 200 mg 400 mg 400 mg 400 mg 3 High dose Mfx (Mfxh) 400 mg 600 mg 600 mg 600 mg 4 Bedaquiline (Bdq) Week 0–2: Bdq 400 mg daily
Week 3–24: Bdq 200 mg 3 times per week
5 Clofazimine (Cfz) 50 mg 100 mg 100 mg 200 mg 6 Cycloserine (Cs)3 250 mg 500 mg 750 mg 1000 mg 7 Linezolid (Lzd) 300 mg 600 mg 600 mg 600 mg 8 Delamanid (Dlm) 50 mg twice daily (100 mg) for 24 weeks in 6-11 years of age
100 mg twice daily (200 mg) for 24 weeks for ≥12 years of age
9 Amikacin (Am)1 500 m 750 mg 750 mg 1000 mg 10 Pyrazinamide (Z) 750 mg 1250 mg 1750 mg 2000 mg 11 Ethionamide (Eto)3 375 mg 500 mg 750 mg 1000 mg 12 Na - PAS (60% weight/ vol)2,3 10 gm 14 gm 16 gm 22 gm 13 Ethambutol (E) 400 mg 800 mg 1200 mg 1600 mg 14 Imipenem - Cilastatin (Imp-Cln)3 2 vials (1 g + 1 g) bd (to be used with Clavulanic acid) 15 Meropenems (Mpm)3 1000 mg three times daily (alternative dosing is 2000 mg twice daily 16 Amoxicillin-Clavulanate (Amx-Clv) (to be given with Carbapenems only) 875/125 mg bd 875/125 mg bd 875/125 mg bd 875/125 mg bd 17 High-dose H (Hh) 300 mg 600 mg 900 mg 900 mg 18 Rifampicin (R) 300 mg 450 mg 600 mg 750 mg 19 Pyridoxine (Pdx) 50 mg 100 mg 100 mg 100 mg 1For adults more than 60 yrs of age, dose of Second Line Injectable (SLI) should be reduced to 10 mg/kg (max up to 750 mg)
2In patients on Para-aminosalicylic Acid (PAS) with 80% weight/volume the dose will be changed to 7.5 gm (16-29 kg); 10 gm (30- 45 kg); 12 gm (46-70 kg) and 16 gm (>70 kg)
3Drugs can be given in divided doses in a day in the event of intolerance
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-resistant Tuberculosis, 2014.
Kindly provide your valuable feedback on the page to the link provided HERE
Treatment of DR-TB in Children
ContentThe principles of designing Drug-resistant TB (DR-TB) treatment regimens (Shorter or longer oral Multi (M)/ Extensively Drug-resistant TB (XDR-TB), and H mono/ poly DR-TB regimens in children are similar to adults:
- Children, aged 5 years to less than 18 years of age and weighing at least 15 kg, are eligible for both longer oral and shorter oral Bedaquiline-containing Multidrug-resistant (MDR)/ Rifampicin-resistant TB (RR-TB) regimens.
- Management of H mono/ poly DR-TB in children will be the same as in adults and child-friendly formulations can be used.
- The drug doses should be used as per paediatric weight bands.
- Bedaquiline (Bdq) tablets suspended in water have been shown to have the same bioavailability as tablets swallowed whole and therefore, should be used to treat DR-TB in children until a child-friendly formulation becomes available.
- Delamanid (Dlm) is already approved for treating M/XDR-TB under the National TB Elimination Programme (NTEP) for children from 6 years onwards.
- As in adults, the extension of Bdq beyond 6 months and concomitant use of Bdq and Dlm in special situations will apply to children as well.
- Treatment can be directly extended to 9 months in certain conditions like extensive disease, extrapulmonary TB, uncontrolled comorbidity, smear-positive cases at the end of the 4th month and when the regimen is modified.
- Shortening the total treatment duration to less than 18 months may be considered in children without the extensive disease.
- For children under 5 years of age, where neither Bdq nor Dlm is approved yet, the longer oral M/XDR-TB regimen should be suitably modified as per the replacement drug. A suitable regimen can be designed considering child-friendly formulations where Bdq can be replaced with Amikacin (Am), Pyrazinamide (Z) or Ethionamide (Eto) in the initial phase.
- Children below 5 years are not excluded from short-course regimens, instead receive short course injectables till further evidence on the use of Bdq is available.
- The use of injectable agents in children should be exceptional and limited to salvage treatment and be monitored for early detection of ototoxicity.
- Meropenem is the preferred drug over imipenem in TB meningitis considering the risk of seizures in children due to Imipenem.
Additional Information
- Achieving an appropriate dose in children aged 3-5 years will be easier when the special formulation dispersible 25 mg tablet used in trials in these age groups becomes available.
- The recent data review for the World Health Organization (WHO) guidelines suggested that there are no additional safety concerns for concurrent use of Dlm with Bdq.
- For treatment and management of adverse drug reactions in children, there should be provision for treatment in consultation with a specialist.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- Consolidated Guidelines on Tuberculosis: Module 4 - Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
DR-TB Treatment Care Cascade
ContentThe Drug-resistant TB (DR-TB) treatment process for all DR-TB patients follows a care cascade.
- DR-TB patient tracing by health staff
- Referral for treatment initiation to health facility/ district or nodal DR-TB site
- Pre-treatment evaluation
- Decision on patient’s treatment regimen by DR-TB committee
- DR-TB treatment initiation*
- Counselling of patient and his/her family
- Treatment supporter identification in consultation with the patient
- Active Drug Safety Monitoring (aDSM) form filling
- Adverse Drug Reaction (ADR) Management (as and when needed)
- Follow up visits to the nearest Health Facility (HF)
- Adverse Drug Reaction (ADR) Management (as and when needed)
- Active Drug Safety Monitoring (aDSM) form filling
- Treatment supporter identification in consultation with the patient
- Counselling of patient and his/her family
- DR-TB treatment initiation*
- Referral for treatment initiation to health facility/ district or nodal DR-TB site
*(H Mono/ Poly DR-TB Patient - Any health facility; Multidrug/ Extensively DR-TB (M/ XDR-TB) Patient - Nodal/ District DR-TB Centre (N/DDR-TBC); Contact of MDR/ DD-TB with FQ-susceptibility - TB Preventive Therapy after ruling out active disease)
HFs are responsible for updating the information of DR-TB patients in Nikshay on a real-time basis.
This entire care cascade needs to be monitored by the Medical Officer of the TB Unit (MO-TU) and the senior DR-TB TB-HIV supervisor. The figure below elaborates on these processes that should be followed in the DR-TB treatment care cascade.
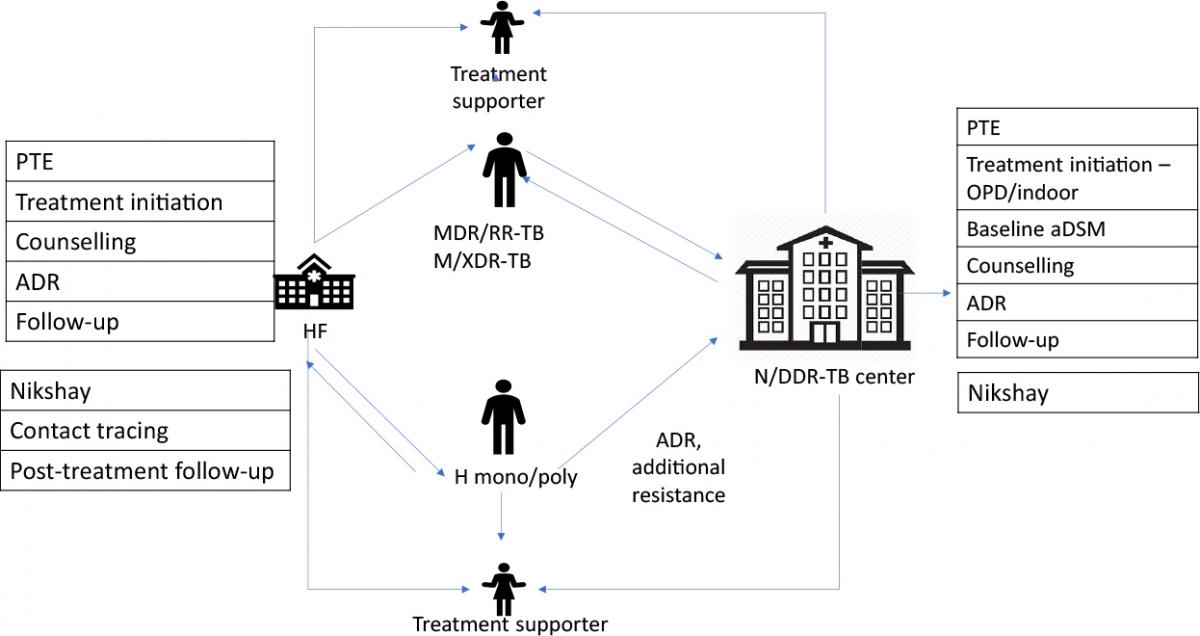
Figure: Processes for all DR-TB Patients in the Treatment Care Cascade; Source: PMDT Guidelines India, 2021, p43.
Abbr: PTE: Pre-treatment Evaluation; ADR: Adverse Drug Reaction; aDSM: Active Drug Safety Monitoring
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-resistant Tuberculosis, 2014.
- WHO Consolidated Guidelines on Tuberculosis, Module 4 - Treatment: Drug-resistant TB Treatment.
Kindly provide your valuable feedback on the page to the link provided HERE
- DR-TB patient tracing by health staff
Pre-treatment Counselling of DR-TB Patients
ContentPre-treatment counselling must serve as an informed decision-making process that enables patients to make a duly informed decision regarding the use of all anti-TB drugs and regimen, including newer drugs.
Written consent is not needed for any treatment regimen under National TB Elimination Programme (NTEP).
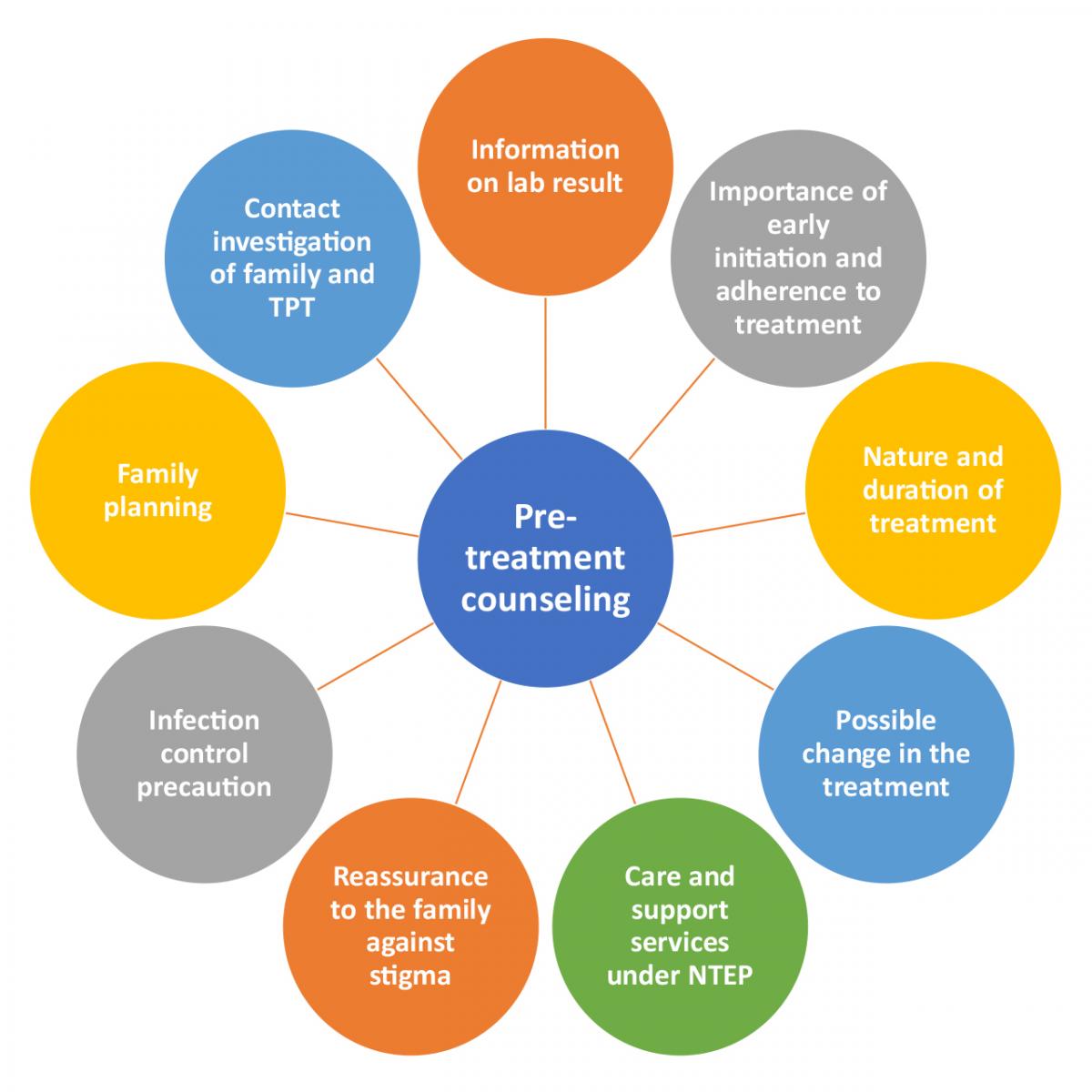
Figure: Key points to be covered during pre-treatment counselling; Source: PMDT Guidelines India, 2021, p45.
Abbr: TPT: TB Preventive Treatment
Training of counsellor:
- All key points depicted in the figure here should be covered.
- A counselling register must be maintained for all patients.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- Technical and Operational Guidelines for TB in India, 2016.
- Central TB Division, MoHFW GOI - Training Modules (1-4) For Programme Managers & Medical Officers (NTEP), 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Pre treatment evaluation of a DRTB cases
ContentLet us understand the objective and importance of Pre-treatment Evaluation (PTE) of Drug-resistant TB (DR-TB) patients.PTE ObjectiveDrugs used for the treatment of drug-resistant TB have significant adverse effects. Hence, there is a need for PTE to rule out any underlying condition at the baseline, like co-morbid conditions, radiological abnormalities, Electrocardiogram (ECG) changes, or biochemical derangements.PTE is essential to identify:- The patient's eligibility for initiation of a particular regimen
- Patients who require special attention during treatment
- Regimen modifications from the beginning of treatment
Important Points
- In the majority of Multidrug-resistant (MDR)/ Rifampicin-resistant Tuberculosis (RR-TB) patients, PTE can be done on an outpatient basis.
- The District TB Officer (DTO) and Medical Officer of the TB Unit (MO-TU) can arrange for PTE at the Nodal and District DR-TB Centre (N/DDR-TBC) or at the sub-district level health facility, wherever feasible.
- No additional investigations are required for H Mono/ Poly DR-TB patients unless clinically indicated.
- The PTE carried out at the time of treatment initiation can be considered valid for 1 month from the date of the test result and the patient can be re-initiated on a subsequent regimen considering the previously conducted PTEs.
- Active Drug Safety Management and Monitoring (aDSM) treatment initiation forms are required to be completed for all DR-TB patients at the time of initiation of each new episode of treatment.
- PTE should include a thorough clinical evaluation by a physician and expert consultation as per the need.
- Laboratory-based tests should be performed based on the drugs used in the treatment regimen.
- Pre-treatment evaluation should be made available free of charge to the patient.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- WHO Consolidated Guidelines on Tuberculosis: Module 4 -Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
DR-TB Treatment – Patient Flow
ContentAfter getting diagnosed with Drug-Resistant TB(DR-TB), the patient is referred to District DRTB Centre(DDR-TBC) for initiation of treatment. Few clinically complicated cases are referred to the Nodal DRTB Centre(NDR TBC). Since the drugs used for the treatment of DR-TB have significant adverse effects and to rule out any underlying comorbid conditions or radiological or ECG, or biochemical derangements, a Pre-treatment evaluation is done to check eligibility of patients for DR-TB regimen and to identify those patients requiring special attention and regimen modifications before initiating patients on TB treatment.
After initiation of treatment, patients are monitored every month. If the sputum test is positive during the follow-up, then the sputum sample is sent for further testing, and if needed, the regimen is changed. And if the sputum sample turns out to be negative during follow up sputum test, then the same treatment regimen is continued till treatment completion.
Post-treatment completion, patients are evaluated at the interval of 6, 12, 18 and 24 months, screened for any clinical signs and symptoms, and, if found suspected, then referred for sputum microscopy and /or culture test.
Figure: TB patient flow after being diagnosed with Multi Drug Resistance TB(MDR/RR TB)
Second Line anti TB drugs
ContentThe anti-TB drugs recommended for treatment of Multi- and Extensively Drug-resistant (M/XDR) TB patients are grouped into three groups – A, B and C (Figure below).
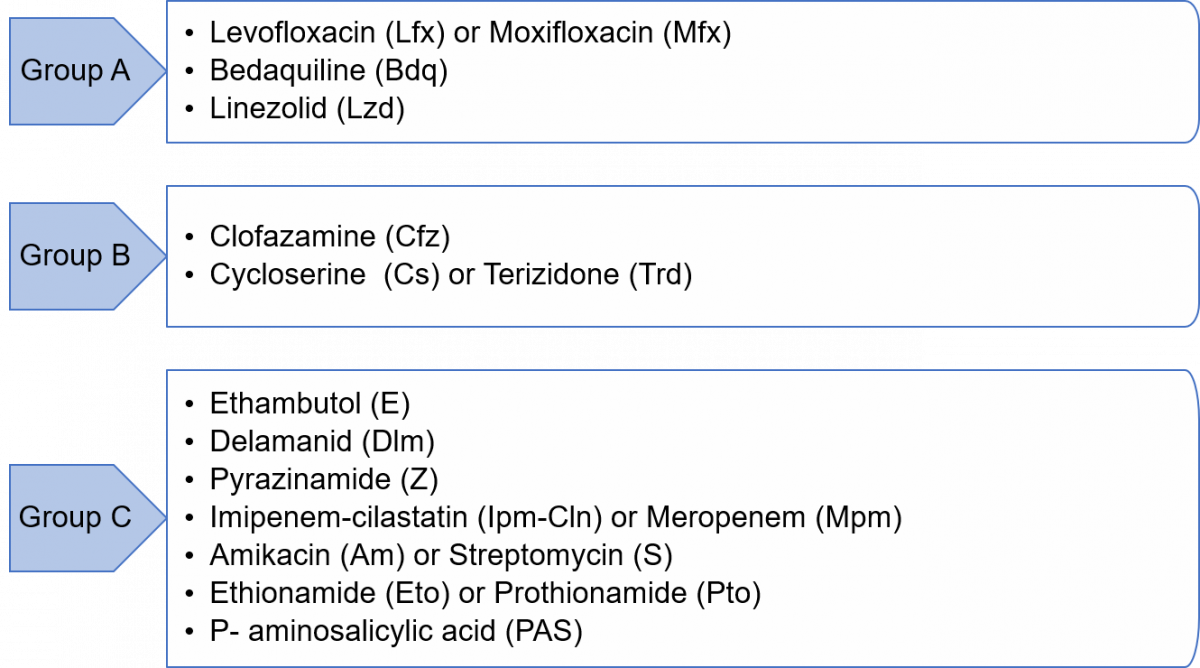
Figure: Groups A, B and C of Anti-TB Drugs used in Treatment of M/XDR-TB Patients
Grouping of drugs is done based on their efficacy, experience of use and drug class. This grouping is intended to guide the design of individualized, longer M/XDR-TB regimens (the composition of the recommended shorter MDR/RR-TB regimen is largely standardized).
Resources
- Guidelines for Programmatic Management of Tuberculosis in India, 2021.
- WHO Consolidated Guidelines on Tuberculosis, Module 4 - Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
DR-TB Treatment Regimens
ContentDepending upon type of drug resistance, there are four broad DRTB Treatment regimen.
- H Mono/Poly Treatment Regimen(6-9 months)
- Shorter oral Bedaquiline containing MDR/RR-TB regimen(9-11 months)
- Shorter injectable containing regimen(9-11 months)
- Longer oral M/XDR-TB regimen(18-20 months)
Drugs administered for DRTB Regimen:
- Drugs are decided based on the drug resistance detected for a patient and will be informed by the medical officer.
- Injections might also be administered to the admitted patient.
- H Mono/Poly Regimen can be initiated at any health facility, while the other two regimen need to be initiated at N/DDR-TB Centre
Figure: Patient wise boxes(PWB) for DRTB Treatment
Treatment Algorithm for MDR/RR-TB
ContentThe treatment algorithm for Multidrug-resistant/ Rifampicin-resistant TB (MDR/ RR-TB) patients is a part of an integrated diagnostic and treatment algorithm under Programmatic Management of Drug-resistant Tuberculosis (PMDT).
A shorter oral Bedaquiline (Bdq)-containing MDR/ RR-TB regimen is recommended for those MDR/ RR-TB patients in whom resistance to the component drugs has been excluded or those who have not been previously treated for more than one month with second-line drugs used in shorter oral Bdq - containing MDR/ RR-TB regimen and have no other exclusion criteria.
All those MDR/ RR-TB patients who are not eligible for a shorter Bdq - containing regimen, after careful evaluation, are considered for a longer M/ XDR-TB regimen.
The treatment algorithm for MDR/ RR-TB patients is shown below.
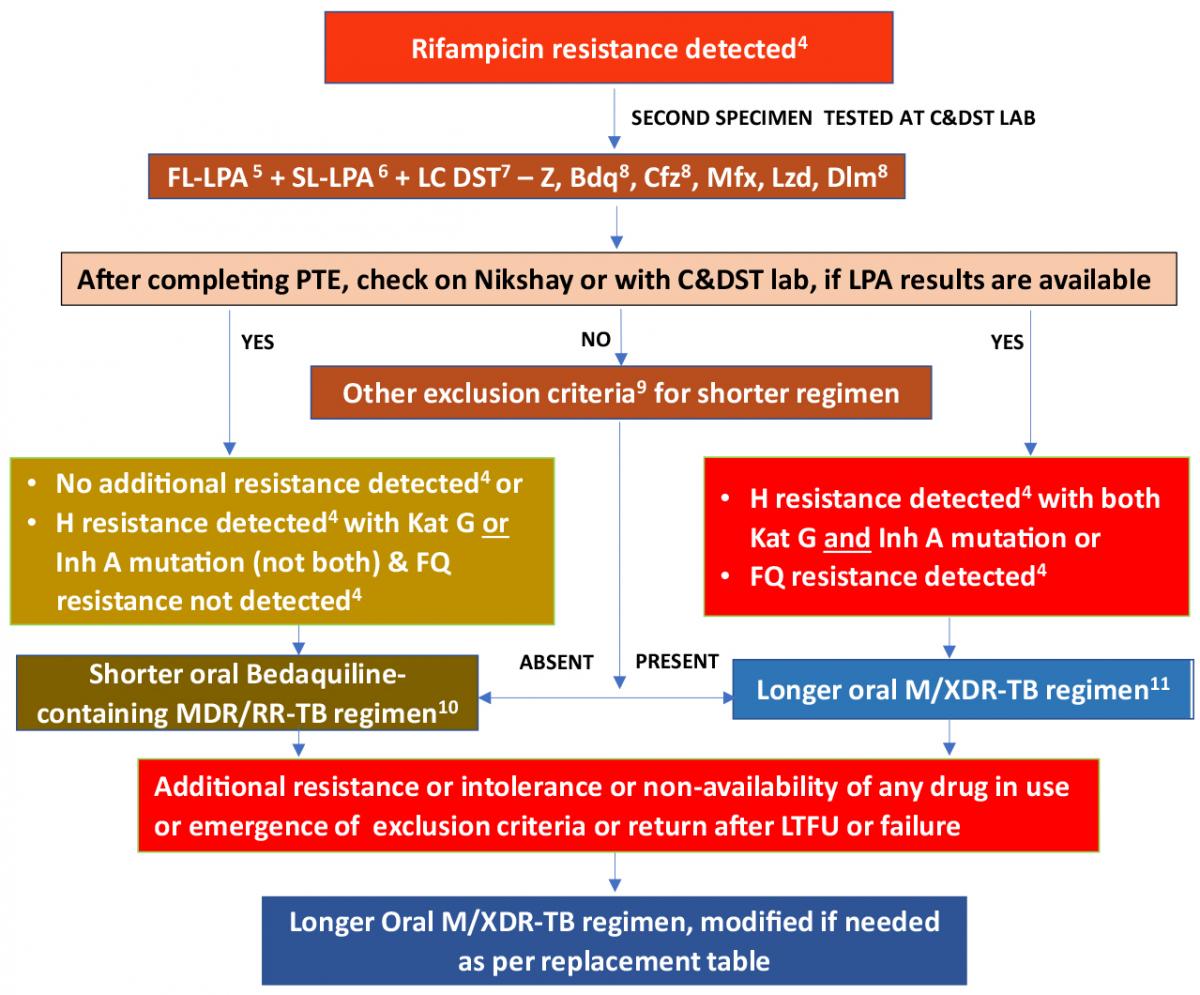
Figure: Treatment Algorithm for MDR/RR-TB; Source: PMDT Guidelines India, March 2021, p46.
Footnotes for the Algorithm
4 As per mutation pattern, includes resistance inferred.
5 Discordance in RR results between Nucleic Acid Amplification Tests (NAAT) & First-line Line Probe Assay (FL-LPA) to be resolved with a repeat NAAT at Culture and Drug Susceptibility Testing (C&DST) lab and microbiologists will provide the final decision. InhA mutation is associated with Eto resistance. Use other exclusion criteria to decide regimen if FL-LPA is done on culture isolates for patients with smear-negative specimens.
6 To assess Levofloxacin (Lfx), Moxifloxacin (Mfx) and Amikacin (Am) resistance.
7 Start treatment based on Line Probe Assay (LPA) results and modify based on Liquid Culture (LC) and DST results later.
8 Whenever DST is available.
9 Other exclusion criteria for shorter oral Bdq-containing MDR/ RR-TB regimen includes:
- History of exposure for > 1 month to Bdq, Lfx, Ethionamide (Eto), or Clofazimine (Cfz), if the result for DST (Bdq, Fluoroquinolone (FQ), Inh A mutation, Cfz & Pyrazinamide (Z)) is not available.
- Intolerance to any drug or risk of toxicity from a drug in the shorter oral Bdq-containing MDR/ RR-TB regimen (e.g. drug-drug interactions).
- Extensive TB disease – the presence of bilateral cavitary disease or extensive parenchymal damage on chest radiography. In children aged under 15 years, presence of cavities or bilateral disease on chest radiography.
- Severe Extrapulmonary TB (EP-TB) disease - the presence of miliary TB or TB meningitis or Central Nervous System (CNS) TB. In children aged under 15 years, extra-pulmonary forms of disease other than lymphadenopathy (peripheral nodes or isolated mediastinal mass without compression).
- Pregnant and lactating women (with conditional exceptions).
- Children below 5 years.
10 This portion applies as states move to a shorter oral Bdq-containing MDR/ RR-TB regimen under the guidance of the National TB Elimination Programme (NTEP).
11 Patients who were on a longer oral M/ XDR-TB regimen based on the history of exposure for >1 month and in whom resistance is not detected to Isoniazid (H) or FQ may be switched to shorter oral Bedaquiline containing MDR/ RR-TB regimen based on the FL and Second-line LPA (SL-LPA) results if the duration of longer oral M/ XDR-TB regimen drugs consumed is <1 month.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, 2021.
- WHO Consolidated Guidelines on Tuberculosis: Module 4 – Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Management of M/XDR-TB Treatment During Pregnancy
ContentIn pregnant women diagnosed with multi-drug resistant (MDR)/rifampicin-resistant TB (RR-TB), if the duration of pregnancy is <20 weeks*, the patient should be advised to opt for medical termination of pregnancy (MTP) in view of the potential severe risk to both the mother and the fetus. Figure 1 shows the management algorithm for pregnant patients based on their gestational age.
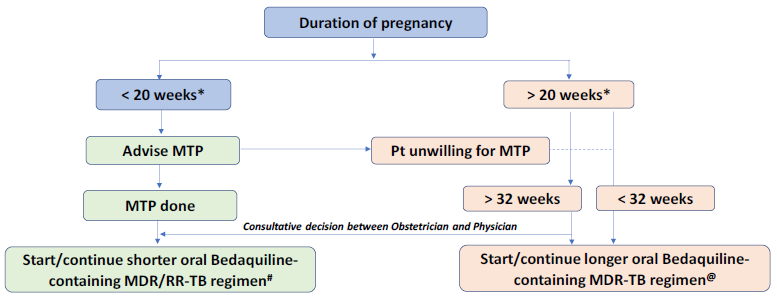
Figure 1: Management of M/XDR-TB patients during pregnancy based on gestation age; Source: Guidelines for PMDT, India 2021, p.71
* 24 weeks will apply wherever the bill is passed.
# Regimen: 4-6 Bdq (6m) Lfx, Cfz, Eto, Hh, Z, E / 5 Lfx, Cfz, Z, E. No modifications allowed.
@ Regimen:18-20 Lfx, Bdq(6m or longer) Lzd#, Cfz, Cs. Lzd dose to be tapered to half after 6-8 months based
on bacteriological response. Modify regimen if one or more drug cannot be used due to reasons of resistance,
tolerability, contraindication, availability etc.
• in the order of Z E PAS.
• Eto may be considered after 32 weeks’ gestation.
• Am may be considered in post-partum period only. Am will not be started in the final 12 months of treatment.- If the pregnancy is ≤ 20 weeks* and the patient is willing to opt for MTP, she should be referred to a gynecologist or obstetrician for MTP after which shorter oral Bedaquiline-containing MDR/RR-TB regimen can be initiated (if the patient has not started treatment) or continued (if the patient is already on treatment) by the DR-TB Centre committee.
- If she does not opt for MTP or has a pregnancy >20 weeks* duration, she will be shifted to a longer oral M/XDR-TB regimen.
- For patients who are unwilling for MTP or have a pregnancy of >20 weeks* (making them ineligible for MTP), the risk to the mother and the fetus should be explained clearly and the pregnant DR-TB patients need to be monitored carefully, both in relation to the treatment and progress of the pregnancy.
- Shorter oral Bedaquiline-containing MDR/RR-TB regimen cannot be administered in pregnant women before 32 weeks due to Ethionamide (Eto)-led potential teratogenicity in the first trimester and risk of hypothyroidism in the infant in the second trimester.
- Beyond 32 weeks, the choice of regimen (shorter/longer) needs to be a consultative decision between the obstetrician and physician at the nodal (N)/district DR-TB Centre (DDR-TBC). More compelling evidence on toxicity causes attributed to the use of specific anti-TB drugs during pregnancy and lactation is needed.
Resources
- Guidelines for Programmatic Management of Drug Resistant Tuberculosis in India, March 2021
- Consolidated Guidelines on Tuberculosis: Module 4- Treatment: Drug resistant TB Treatment , 2020
- Technical and Operational Guidelines for TB in India, 2016
- Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-Resistant Tuberculosis, 2014
Kindly provide your valuable feedback on the page to the link provided HERE
DR-TB Treatment in Pregnancy: Recommendation for the Use of Contraception
ContentAll women of childbearing age who are awaiting results of the Culture and Drug Susceptibility Test (C&DST), as well as those receiving Drug-resistant TB (DR-TB) treatment, should be advised and counselled intensively to use birth control measures because of the potential risk to both the mother and the foetus.
- It should be noted that oral contraceptives might have decreased efficacy due to vomiting and drug interactions with DR-TB drugs (use of Rifampicin in mono/poly resistant TB).
- Contraception methods that can be used during DR-TB treatment, based on individual preference and eligibility are:
- Barrier methods (e.g., condoms/ diaphragms), intrauterine devices (e.g., CuT), Depot medroxyprogesterone (Depo-provera).
- In women, the Isoniazid (H) mono/poly DR-TB regimen may be started or continued safely, except that care should be taken while using oral contraceptives.
- A woman on oral contraception, while receiving rifampicin treatment may choose between two options following consultation with a physician:
- Use of an oral contraceptive pill containing a higher dose of oestrogen (50 μg)
- Use of another form of contraception.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- Consolidated Guidelines on Tuberculosis: Module 4 - Treatment: Drug-resistant TB Treatment, 2020.
- Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-resistant Tuberculosis, 2014.
- Collaborative Framework for Management of Tuberculosis in Pregnant Women, 2021.
Kindly provide your valuable feedback on the page to the link provided HERE
Follow-up Monitoring of DR-TB Patients
ContentThe following points should be covered in follow-up monitoring of Drug-resistant TB (DR-TB) patients:
- Monitor DR-TB treatment progress and disease response.
- Monitor bacteriological and radiological improvements in DR-TB treatment.
- Identify derangements in bio-chemical results and on Electrocardiogram (ECG) which are indicative of systemic disorders that could result in drug-induced adverse events, or comorbidities that may require timely interventions to address and improve the probability of treatment success, survival and quality of life.
- Follow-up monitoring to be done periodically based on the type of TB/ severity of disease/ type of regimen used, etc.
Components of Follow-up Monitoring
- Clinical monitoring
- Follow-up evaluations
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- WHO Consolidated Guidelines on Tuberculosis: Module 4 - Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Rehabilitation service to TB patients
ContentThe holistic management of Tuberculosis (TB) patients can improve their life expectancy. The importance of addressing malnutrition, adverse drug reactions, psycho-social well-being, and catastrophic expenses correctly and in a timely fashion is essential in reducing morbidity and mortality.
Table: Rehabilitation services for TB patients Rehabilitation Services for TB Patients Care Providers Key Components Nutritional Rehabilitation 1. Senior Treatment Supervisor
2. TB Health Visitors
3. Accredited Social Health Activists (ASHAs)
4. Auxiliary Nurse Midwife (ANM)
5. TB treatment supporter
6. Medical officers at Peripheral Health Centre (PHC), Community Health Centre (CHC) level
-
Supporting nutritional needs of TB patients through Ni-kshay Poshan Yojana
-
Management of undernutrition in nutrition rehabilitation centres (NRCs)
-
Linkages for extra nutritional support for TB patients like the public distribution system (PDS) or food security act.
Pulmonary Rehabilitation
1.Physiotherapists (preferable one male and one female)
2. Nurses
3. Attendant
Management of physical and psychological impairment due to the disease to lower the handicap. Physical Rehabilitation -
therapists (preferable one male and one female)
-
Nurse Doctors
-
Surgeons
-
Physio
-
Attendant
-
Management of post-treatment sequelae by early identification and periodic assessment.
-
Comorbidity management
Social Rehabilitation 1. TB Health Visitors
2. Accredited Social
3. Health Activists (ASHAs)
4. Auxiliary Nurse Midwife (ANM)
5. TB treatment supporter
6. Medical officers at PHC, CHC level
7. Ni-kshay Mitra
-
Linkage for vocational rehabilitation e.g., Skill India
-
Synergy between social welfare support systems like:
-
Rashtriya Swasthya Bima Yojana (RSBY)
-
TB pension schemes
-
National rural employment guarantee scheme
-
National Health Protection Scheme (NHPS) for palliative care and rehabilitation
Mental Rehabilitation 1. Psychiatrist
2. Psychologists / Counsellors
3. TB Health Visitors
4. Accredited Social
5. Health Activists (ASHAs)
6. Auxiliary Nurse Midwife (ANM)
7. TB treatment supporter
8. Medical officers at PHC, CHC level
-
Psychological counselling to the patient and caregivers.
-
Assisting patients in the planning of decisions related to the end-of-life stage.
Patient rehabilitation is ensured by:
-
1. IT-based monitoring via Ni-kshay platform
-
2. Community-based monitoring
-
3. Surveillance: A comprehensive surveillance system for TB patients and their providers built into eNikshay. This is supported by a call centre for user-friendly private reporting and patient monitoring.
Resource
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Rehabilitation services to TB patients comprise Nutritional, Physical, Pulmonary, Social and Mental Rehabilitation.
False
True
2
The holistic management of tuberculosis (TB) patients can improve life expectancy. The importance of addressing malnutrition, adverse drug reactions, psycho-social well-being, and catastrophic expenses correctly and in a timely fashion is essential in reducing morbidity and mortality.
-
Palliative Care in DR-TB
ContentThe World Health Organization (WHO) defines palliative care as an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illnesses, through prevention and relief of suffering by means of early identification, impeccable assessment, and treatment of pain and other physical, psychosocial and spiritual problems.
The goal of such treatment is to improve the quality of life for both the patient and their family.
Drug-resistant TB (DR-TB) remains a life-threatening condition with high mortality and poor cure rates, considering this palliative care is more relevant in DR-TB patients. Palliative care is being considered under the National TB Elimination Programme (NTEP) for DR-TB patients who have advanced disease and reduced lung functions. The approach involves systematically engaging institutes with expertise in palliative care (public as well as private facilities) for providing such care to needy TB patients.
The benefits of DR-TB patients receiving palliative care are as follows:
- Provides relief from respiratory distress, pain and other symptoms.
- Affirms life and regards dying as a normal process and intends neither to hasten nor postpone death.
- Integrates the psychological and spiritual aspects of patient care.
- Offers a support system to help patients live as actively as possible until death.
- Offers a support system to help the family cope during the patient’s illness and in their bereavement.
- Enhances quality of life and may also positively influence the course of illness.
Resources
- Companion Handbook to the WHO Guidelines for the Programmatic Management Of Drug-resistant Tuberculosis, 2014.
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, 2021.
Kindly provide your valuable feedback on the page to the link provided HERE
Need for Palliative Care in DR-TB Patients
ContentThe current TB treatment strategy is based on a patient-centred approach to treatment and alleviation of patients' suffering that has been restricted mostly to its physical aspects. However, difficulties faced by patients and families affected by life-threatening diseases span across physical, psychological, social and spiritual aspects. Therefore, a more holistic approach to patient treatment requires broadening to a patient-centric care approach with palliative care services.
Palliative care would be necessary for the care of:
- Patients who are chronically ill with extensive drug resistance and extensive fibro-cavitary or disseminated bilateral lung disease
- Patients who have failed regimen for Extensively Drug-resistant Tuberculosis (XDR-TB) or mixed pattern resistance
- Patients for whom the World Health Organization (WHO)-recommended regimen cannot be designed even with new drugs.
There is significant suffering associated with Drug-resistant TB (DR-TB) illness and its treatment. This kind of burden increases the possibility of TB patients not being able to adhere to treatment which many times results in the treatment failing to cure them.
Delivering palliative care to alleviate the suffering of patients during Multidrug-resistant TB (MDR-TB) treatment, especially when all possibilities of treatment have failed, is an ethical imperative.
Thus, the need for palliative and end-of-life care is being increasingly recognized as an important part of the continuum of care for DR-TB patients.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, 2021.
- Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-resistant Tuberculosis, 2014.
Kindly provide your valuable feedback on the page to the link provided HERE
Interim Treatment Outcomes of DR-TB Cases
ContentThere are two main interim treatment outcomes that can occur during Drug-resistant TB (DR-TB) treatment. These are:
Bacteriological Conversion: This occurs after bacteriological confirmation of TB in at least two consecutive cultures (applicable for DR-TB and Drug-sensitive (DS-TB)) or smears (applicable for DS-TB only), taken on different occasions, at least 7 days apart, are found to be negative.
Bacteriological Reversion: This occurs when at least two consecutive cultures (applicable for DR-TB and DS-TB) or smears (applicable for DS-TB only), taken on different occasions, at least 7 days apart, are found to be positive, either after the initial conversion or for patients without bacteriological confirmation of TB.
For defining treatment failed, bacteriological reversion is considered only when it occurs in the continuation phase.
Time-to-culture conversion is calculated as the interval between the date of DR-TB treatment initiation and the date of the first of these two negative consecutive cultures taken 7 days apart (date of sputum specimens collected for culture should be used).
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- WHO Consolidated Guidelines on Tuberculosis: Module 4 – Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Final Treatment Outcomes of DR-TB Cases
ContentUnder the National TB Elimination Programme (NTEP), the treatment outcome definitions of Drug-susceptible TB (DS-TB) and Drug-resistant TB (DR-TB) have been aligned in recent times. However, the treatment outcome is declared at different time points for certain outcomes (e.g., cured/ treatment completed) since the duration of DR-TB treatment is longer when compared to DS-TB treatment.
Table: Final DR-TB Treatment Outcomes
TREATMENT OUTCOMES
DEFINITION
REMARKS
Treatment failed
A patient whose treatment regimen needs to be terminated or permanently changed to a new regimen option or treatment strategy.
Reasons for the change include:
- No clinical and/or bacteriological response (a bacteriological conversion with no reversion)
- Adverse Drug Reactions (ADRs)
- Evidence of additional drug resistance to medicines in the regimen
Cured
A pulmonary TB patient with bacteriologically confirmed TB at the beginning of treatment who completed the treatment as recommended by the national policy with evidence of bacteriological response and no evidence of treatment failed.
Bacteriological response - bacteriological conversion with no reversion. Treatment completed
A patient who completed the treatment as recommended by the national policy whose outcome does not meet the definition for cured or treatment failed.
---
Died
A patient who died before starting or during the course of treatment.
Patient died of any reason.
Lost to follow-up
A patient who did not start the treatment or whose treatment was interrupted for 2 consecutive months or more.
---
Not evaluated
A patient for whom no treatment outcome was assigned.
This includes cases “transferred out” to another treatment unit and whose treatment outcome is unknown and excludes patients who lost to follow-up.
Points to Note
- In case of a change in the regimen within the scope of the guidelines, from shorter to longer or vice-versa in the initial months before any definitive treatment outcome applies, the outcome of only the changed regimen needs to be reported. The patient needs to be moved out of the denominator of the previous regimen.
- Patients who are still on treatment due to frequent short interruptions (less than 2 consecutive months) due to patient or provider requirements can be reported as not evaluated as an outcome is not assigned at the time of reporting, but the data can be cleaned and updated later when the outcome is available.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
Interim reports of DR-TB Treatment
ContentAs Drug-resistant TB (DR-TB) treatment is of relatively long duration, the interim treatment reports are prepared in Ni-kshay to assess the interim treatment outcomes in the programme.
Criteria
- The interim report assessment period is six calendar months, usually counted from January to the end of June and July to the end of December.
- All patients registered and starting treatment during the assessment period are included in the calculation.
Interpretation
- Interim results of DR-TB patients who started treatment during the first semester of a year (1 January to 30 June), should be calculated at the beginning of April of the following year.
- The interim report form should be completed 9 months after the closing day of the cohort so as to allow culture information at 6 months of treatment to be included for all patients in the cohort.
Sl. No.
DR-TB Regimen
Time point for interim reporting
Cohort for interim evaluation, reporting and monitoring (Here ‘X’ is the reporting month)
If reporting month
is X= April 2023,
following are the corresponding cohort for interim
report evaluation1
Isoniazid (H) - mono/ poly DR-TB regimen
4th month of treatment
X - 6 months
Cohort of October 2022 and previous
2
Shorter oral Bedaquiline-containing Multidrug-resistant (MDR)/ Rifampicin-resistant (RR)-TB regimen
4th month of treatment
X - 6 months
Cohort of October 2022 and previous
3
Longer oral Multidrug-resistant/ Extensively Drug-resistant TB (M/XDR-TB) regimen
6th month of treatment
X - 10 months
Cohort of June 2022 and previous
4
BPal (Bedaquiline, Pretomanid, Linezolid) regimen
4th month of treatment
X - 6 months
Cohort of October 2022 and previous
5
Prior longer M/XDR-TB regimen (Drug Susceptibility Testing (DST) guided regimen)
6th month of treatment
X - 10 months
Cohort of June 2022 and previous
Importance
- Culture conversion (for confirmed DR-TB cases) and death by six months are important predictors of final outcomes.
- It also provides early information on the number of patients initiated on second-line drugs for MDR-TB that turned out not to be XDR.
- Information on treatment interruption at the end of six months is important for programme review and implementing corrective actions.
- Overall interim reports are important for supervision, monitoring and evaluation at all programmatic levels.
Resources
- Guidelines on Programmatic Management of Drug-resistant TB (PMDT) in India, 2021, CTD, MoHFW, India.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
What is the duration of the assessment of the interim report in NTEP?
2 Calendar months
3 Calendar months
6 Calendar months
12 Calendar months
3
The interim report assessment period is six calendar months, usually counted from January to the end of June and July to the end of December.
Yes
Yes
PMDT Report
ContentVideo fileVideo: PMDT Report
Fullscreen