Community Engagement
ContentCommunity engagement is a process of developing relationships that enable stakeholders to work together to address health-related issues and promote well-being to achieve positive health impact and outcomes.
Mobilize communities to engage them in TB care and to increase ownership of the Programme by communities.
Why Community Engagement?
Figure: Importance of Community Engagement
Importance of Community Engagement in TB
ContentCommunity-based TB activities are conducted outside the premises of formal health facilities (e.g. hospitals and clinics) in community-based structures (e.g. schools and places of worship) and homesteads. Community health workers and community volunteers carry out community-based TB activities. Both can be supported by nongovernmental organizations and/or the government.
Community Engagement is a cost effective intervention to improve health service coverage and deliver accessible and people-centered integrated care.
Figure: Importance of Community Engagement
Strategies of Community Engagement in NTEP
Content- Scaling up community participation in the National TB Elimination Programme through community-led activities and working with various community groups, especially TB survivors and key populations
- Empower TB survivors and affected populations to act as mentor’s/change agents and build their capacity for engaging them in programme planning, implementation and monitoring
- Working with community stakeholders to aid in early case identification amongst the vulnerable population
- Increasing accountability of the service delivery system through community participation
State TB Forum
ContentThe TB forum for community engagement aims to empower and engage the TB-affected community. The forum acts as a bridge between the community, TB patients, the health system and civil society. In these forums, advocacy activities are undertaken to influence policy changes for accessible, affordable, supportive TB services to the entire population with a special focus on poor and vulnerable groups.
Under the National TB Elimination Programme (NTEP), there are provisions for the constitution of state TB forums at the state level. The state TB forum consists of various stakeholders as shown in the table below. The meetings of these forums are to be convened at least every 6 months at the state level.
Table: Composition of the State TB Forum
Chairperson Principal Secretary / Secretary Health & Family Welfare, State Govt. Co-Chairperson Mission Director (National Health Mission) Members - Project Director, SACS
- Director Health Services
- WHO Representative – TB Consultant
- State Chairman/ Secretary, Tuberculosis Association of India
- Public Health Foundation of India/ any reputed public health institute
- State President, Indian Medical Association
- Professor of Pulmonary Medicine and Professor of Community Medicine of Medical Colleges
- Two representatives of reputed local NGOs/ CSOs on a rotation basis
- One representative from NTEP partners on a rotation basis (REACH/ UNION/ CHAI/ PATH/ FIND/ WHP/ KHPT)
- Representative of PLHIV Networks
- Five TB patient representatives (past TB patients/ family members)
- Representative of Corporate Sector/ Industry/ PSU
- State TB Officer
- One representative each from SACS, NPCDCS, SPMU, RCH, NUHM
Abbr: SACS: State AIDS Control Society; WHO: World Health Organisation; NGOs/CSOs: Non-governmental and Civil Society Organisations; NTEP: National TB Elimination Programme; WHP: World Health Partners, PLHIV: People Living with HIV; PSU: Public Sector Undertaking; NPCDCS: National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular diseases and Stroke; SPMU: State Programme Management Unit; RCH: Reproductive Child Health; NUHM: National Urban Health Mission Functions of the State TB Forum
- To advise on strategies for engaging communities affected by TB and increasing community participation in TB programs by forming a network of people affected by TB.
- To periodically review the progress of community involvement and network of people affected by TB.
- Highlight the concerns and needs of TB patients, work with the government and a broad range of individuals/ organisations to develop better and more responsive health services.
- Advocate for greater and more equitable access to quality, accurate and independent information for patients. To focus on reducing health inequalities by campaigning for patients to have the right to be involved in decision-making.
- Enable dialogue between all stakeholders involved in a TB patient’s care such as government (including local self-government), medical and paramedical associations, industry, medical insurance companies, private healthcare providers and diagnostic centres.
- Create and manage resources to sustain and accelerate TB prevention, control, care and treatment services through community engagement and a network of people affected by TB.
- Facilitate nutritional support, linkages with social welfare schemes, and rehabilitation of TB patients.
- Perform grievance redressal.
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Concerning the state TB forum, which of the following is false? It is involved in engaging communities affected by TB at the state level. It is chaired by the person affected by TB. It has 33 stakeholders. It convenes meetings biannually. 2 State TB forums are chaired by the Principal Secretary/ Secretary HFW, State Govt. Yes Yes Local Self Government [LSG]
ContentLocal Self Government is the management of local affairs by local bodies who have been elected by the local people.
-
The local self-Government includes both rural and urban government.
Image
Figure 1: Types of local self government
Rural Local Governments:
-
Panchayati Raj Institution (PRI) is a system of rural local self-government in India. PRI was constitutionalized through the 73rd Constitutional Amendment Act, 1992. The panchayat raj system in the entire country is not the same but, by and large, structure of LSG in most of the States have the three-tier structure:
Image
Figure 2: Structure of Panchayati Raj
Urban Local Governments:
-
An urban area is usually a compact and densely populated area. All types of urban local governments are democratically elected by the people based on electoral wards.
-
Municipal administration is necessary to provide basic civic facilities like water supply, drainage, garbage disposal, public health, primary education, construction, and maintenance.
Image
Figure 3: Types of Urban local bodies
- Other types of urban local governments in India - Notified Area Committee, Town Area Committee, Cantonment Board, township, Port trust, Special purpose agency.
Role of Local Self Government in Health.
-
The common departments in the LSGs are General Administration, Finance, Public Works, Agriculture, Health, Education, Social Welfare, Information Technology, and others. Thus, LSG could play an important role in addressing the determinants of health.
-
LSGs play an active role in preventive healthcare services like vaccination, controlling drinking water and foods, mother-child health, disease screening programs, sanitation precautions, controlling of wastes and animal diseases, controlling of environmental factors that have disease risks such as air and water pollution. They are seen as critical to the planning, implementation, and monitoring of the NHM. Implementation of the NHM in achieving its outcomes is significantly dependent on well-functioning gram, block and district level panchayats.
-
LSGs also deliver services toward health promotion.
-
The other services provided by the LSGs are: Emergency and ambulance services, rehabilitation centers, elderly care centers and home care services
-
ASHA/USHA is one of the important functionary in health care service delivery and selected by the Gram Panchayat.
Resources
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
The fundamental objective of Panchayati Raj system is to ensure which among the following?
1. People’s participation in development
2. Political accountability
3. Democratic decentralisation
4. Financial mobilisation
1,2,3
2,3
1,4
1,3
4
Panchayat Raj Institution (PRI) was constitutionalised to build democracy at the grassroots level and was entrusted with the task of rural development in the country. Active participation and vigilance on the part of the rural public is a must for the sustenance of democratic de-centralisation.
-
Role of LSG in TB Elimination
ContentLocal Self Governance is the management of local affairs by local bodies who have been elected by the local people. There are 2 types of Local Self Government (LSG): panchayats in rural areas and municipalities in urban areas. Local self-government (LSG) has deep connections and linkages with local people. Role of LSG in Tuberculosis (TB) elimination includes:
Image
Fig 1: Role of Local Self Government in TB Elimination
-
Awareness generation activities
With the participation of Panchayati Raj Institution (PRI) members in rural areas and municipalities in urban areas following awareness generation activities can be carried out:
- Health education on symptoms of TB, good cough etiquettes, available services for screening, diagnosis and treatment of TB, patient support/benefit schemes, TB in vulnerable groups (children, pregnant women, diabetic patients, patients on immunosuppressants, alcoholics and smokers) with emphasis on periodic screening for TB.
- Observance of World Tuberculosis Day on March 24
- Organize health-checkup camps and talks with the TB survivors
- Sensitize Panchayat Raj Institutions (PRI) members, faith leaders etc.
- Organize anti-stigma and non-discrimination campaigns
- Advocacy interventions
Local administration or Panchayat Raj Institutions (PRI) can be engaged in advocacy interventions to promote healthy behaviours and leverage support of TB patients:
- To install spitting bins.
- To install signages on good cough etiquettes.
- Free distribution of masks/handkerchief/tissues to TB patients in the community.
- Services for case finding (Active and latent TB Infection)
With the help of LSGs outreach activity can be planned and undertaken by community/non-governmental organizations (NGO) volunteers, Accredited Social Health Activist (ASHA) and Multi-Purpose Worker (MPW-Male)/ Auxiliary Nurse Midwife (ANM) under the supervision of the Community Health Officer (CHO)/Medical Officer- Urban Primary Health Centre (MO-UPHC), for case finding. These activities include:
- Vulnerability assessment
- Screening for symptoms of TB using Community Based Assessment Checklist (CBAC)
- Periodic active case finding among identified vulnerable populations
- Prompt referral of persons with TB symptoms to health center
- Treatment support and monitoring
- Local self governments can engage in formation and conducting meetings of treatment support groups.
- Health education for TB patients and their household contacts can be conducted on TB symptoms, treatment, managing adverse drug reactions, nutrition during house visits and treatment support group meetings.
- Counselling for TB patients and caregivers can be organised by PRI members and local administration.
- LSGs can mobilise funds from philanthropists to support the TB Patients, to supplement and augment healthcare facilities, screening and testing requirements, buying diagnostics and any other resources that might be required.
- TB preventive measures
- Under supervision of LSGs screening can be conducted of household/workplace contacts and other contacts of TB patients as eligible in the local context and identified vulnerable population for TB/latent TB infection.
- LSG can promote airborne infection control at workplaces and community settings.
- Interventions to ensure community participation
- LSGs can participate in identifying and training TB Champions and facilitate their participation in Village Health Sanitation Nutrition Committees (VHSNCs), Mahila Arogya Samitis (MASs), Jan Arogya Samitis and TB forum meetings.
- VHSNCs and MASs can discuss TB related issues in their meetings, conduct awareness programmes and extend support to case finding and treatment.
Resources
- Operational Guidelines for TB Services at Ayushman Bharat Health and Wellness Centres Central TB Division, Ministry of Health and Family Welfare (MoHFW), Government of India 2020
- Pradhan Mantri Khanij Kshetra Kalyan Yojana (PMKKKY), Ministry of Mines, Government of India, 2015.
- Training Modules (5-9) for Programme Managers and Medical Officers, Central TB Division, Ministry of Health and Family Welfare (MoHFW), Government of India, 2020.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Local self-government can help in identifying and mapping socially and clinically vulnerable groups using available data from Municipal/ Block/ Taluka/ Zila Panchayats' records. Periodic drives can be conducted by them to identify and trace cases and link them to services provided under National Tuberculosis Elimination Programme (NTEP) and other social schemes.
True
False
1
Media advocacy by local self-government can engage the local media to disseminate information. With strategic communication and social mobilisation through Local self-government, the community members will help in gaining awareness about the services available in NTEP as well as other social schemes.
-
District TB Forum
ContentThe district TB forum is a community-engagement modality that aims to empower and engage the TB-affected community. Constituted by TB patients (cured or on treatment), community leaders, government officials, experts and NGOs; it gives a voice to the affected community and advocates with the programme managers for the resolution of challenges faced by TB patients in accessing TB services.
District TB forum is composed of various stakeholders as shown in the table below and its meeting is to be convened at least every 6 months at the district level.
Table: Composition of the District TB Forum
Chairperson District Magistrate Co-Chairperson Chief Executive Officer, Zilla Parishad Members - District Development Officer
- Chief Medical/ Health Officer
- WHO Representative – TB Consultant
- Representative of Tuberculosis Association of India
- Pulmonologist and Professor of Community Medicine of Medical Colleges
- District President, Indian Medical Association
- Two representatives of reputed local NGOs/CSOs on a rotation basis
- Representative from NTEP partners on a rotation basis (REACH/ UNION/ CHAI/ PATH/ FIND/ WHP/ KHPT)
- Five TB patient representatives (past TB patients/ family members)
- Representative of district-level PLHIV Network
- Representative Officer from RCH who manages NGOs
- District TB Officer
- PRI member (Zilla Parishad/ BDC/ Panchayat)
- Journalist
- Advocate
- Representative of the corporate sector
Abbr: WHO: World Health Organisation; NGOs/CSOs: Non-governmental and Civil Society Organisations; NTEP: National TB Elimination Programme; WHP: World Health Partners, PLHIV: People Living with HIV; RCH: Reproductive Child Health; PRI: Panchayati Raj Institutions; BDC: Block Development Council Functions of the District TB Forum
- To advise on strategies for engaging communities affected by TB and increasing community participation in TB programs by forming a network of people affected by TB.
- To periodically review the progress of community involvement and network of people affected by TB.
- Highlight the concerns and needs of TB patients, and work with the government and a broad range of individuals/ organisations to develop better and more responsive health services.
- Advocate for greater and more equitable access to quality, accurate and independent information for patients. To focus on reducing health inequalities by campaigning for patients to have the right to be involved in decision-making.
- Enable dialogue between all stakeholders involved in a TB patient’s care such as government (including local self-government), medical and paramedical associations, industry, medical insurance companies, private healthcare providers and diagnostic centres.
- Create and manage resources to sustain and accelerate TB prevention, control, care and treatment services through community engagement and a network of people affected by TB.
- Facilitate nutritional support, linkages with social welfare schemes, and rehabilitation of TB patients.
- Perform grievance redressal.
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Concerning the district TB forum, which of the following is true? It is involved in engaging communities affected by TB at the state level. It is chaired by the person affected by TB. It has only 3 stakeholders. It convenes meetings biannually. 4 The district TB forum engages communities affected by TB at the district level is chaired by district magistrates, convenes meetings biannually, and comprises of various stakeholders. Yes Yes TB Champion
ContentA TB Champion is a person who has been affected by TB and successfully completed the treatment.
TB Champions, in their capacity as survivors, are role models and can provide valuable support to those with TB and their families.
Figure: Roles of TB Champion
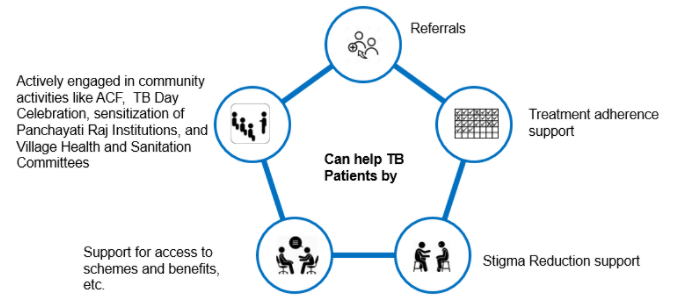
Community Health Volunteers should identify TB Champions and engage them to provide their support to the patient in activities like:
Figure: Help to TB Patients by Community Health Volunteers
Joint Effort for Elimination of Tuberculosis [JEET] Model of the Patient Provider Support Agency [PPSA]
ContentStudies have shown that nearly half of all patients with TB in India first seek care in the private sector, where there are significant gaps across the patient-care cascade, notably diagnostic delays, irrational and non-standardized regimens, and under-reporting to authorities. As a result, over a million cases of TB are missed in India every year. In order to address these challenges, project “Joint Effort for Elimination of Tuberculosis” (JEET) was envisaged. The key objective of this project is to set up effective and sustainable structures to strengthen existing systems and seamlessly extend quality TB care to patients in the private sector.
Patient Provider Support Agency (PPSA)
PPSA is one of the implementation Models under JEET Project and is responsible for continuous, end-to-end engagement of private sector to provide quality TB services to patients seeking care in private sector. The PPSA Model has the following key components:
1. Engagement of private providers
-
Network with private sector providers and promotes quality and early diagnosis,
-
Use of rapid diagnostics and Drug Susceptibility Testing (DST), TB notifications, and treatment as per Standards for TB Care in India (STCI)
-
Utilisation of available public sector services under the National TB Elimination Programme (NTEP) for the patients seeking care in the private sector.
2. Support engaged private sector providers for TB notifications in Ni-kshay
-
Through sensitisation
-
By establishing mechanisms/ modalities to support private sector notifications.
3. Linkage to free diagnostics services by the programme
-
All the presumptive TB cases are linked to free TB diagnostics services extended through a sample transport mechanism established under PPSA.
4. Linkage to free treatment services by the NTEP
-
Facilitates issue of NTEP Fixed Dose Combinations (FDCs) through engaged private sector practitioners and chemists
-
Facilitates linking patients to the public sector for initiation of treatment of Drug-sensitive TB (DS-TB) and Drug-resistant TB (DR-TB)
5. Support for treatment adherence
Adherence support is provided to patients through:
-
A team of treatment coordinators
-
NTEP provided Information and Communication Technology (ICT) enabled mechanism/ Call Centre for reminder SMS and phone calls.
6. Incentives to patients and private providers
-
NTEP provisioned incentives as per the National Strategic Plan (NSP) are provided to the engaged private providers and patients seeking care through them.
Image
Figure: The Service Delivery Model for PPSA
Patient Provider Support Agency Lite (PPSA lite)
An alternative model of PPSA called PPSA lite is implemented in 141 cities across seven states. City officers in PPSA lite cities/ districts support:
-
Mapping of private practitioners and identification of TB champions
-
Private sector provider engagement through Continuing Medical Education (CMEs)
-
Capacity building of NTEP staff to undertake private sector engagement.
-
Providing program monitoring support and facilitating reviews.
Resources
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Under PPSA treatment adherence support is provided to patients in the private sector.
True
False
1
Adherence support is provided to patients through a team of treatment coordinators and through NTEP-provided Information and Communication Technology (ICT) enabled mechanism/ Call Centre for reminder SMS and phone calls.
YES
YES
-
Patient-provider meetings
ContentPatient-provider meetings are important to ensure patient support and improve case holding/ treatment adherence.
Objective: To orient the patients on the course of the treatment, the importance of adherence and the risk for close contact. It also provides a platform to discuss the difficulty in following treatment courses by the patients and the need for further counselling if required.
Purpose: The purpose of this meeting is to counsel patients in a group who are on treatment or who are about to begin treatment. This is an opportunity for free interaction between providers and patients and also an opportunity for patients to clarify their doubts, if any.
Facilitators: These meetings are organized by the treatment supporter/ Directly Observed Treatment (DOT) provider. The Senior Treatment Supervisor (STS)/ Medical Officer (MO) are to conduct these meetings.
Target Group: Patients on treatment or who are about to begin treatment. There could be 5-10 patients (minimum) in such meetings. (If there is a large number of patients at one centre, small groups of about 10 patients may be made so that better interaction takes place between patients and providers).
Participants: Block medical officer/ Medical Officer - TB Control (MO-TC), field staff (STS, TB Health Visitor (TBHV), Senior TB Lab Supervisor (STLS)), general health system staff, patients and their attendees.
Place: These meetings are to be organized at the health facility.
Duration and Frequency: These meetings can be organized once a month so that each patient who is on treatment has the opportunity to attend one such meeting during the intensive phase. The frequency of such meetings would be more than one in a month when there is a large number of patients at one health facility.
- Each meeting can be for half-hour to one hour.
- The patient may be provided refreshments (tea, snacks etc.)
Note: Patient-provider interaction meetings are additional to, and are different from, interpersonal communication that the provider has with the patient while administering treatment.
Messages to be Provided to Patients
- Basic information about tuberculosis, cough etiquette, etc.
- Importance of completing treatment
- Side-effects of drugs and how to manage these
- Importance of follow-up sputum examination
- Prophylaxis for children in the family
- Do’s and don’ts including protective measures, the role of a nutritious diet, etc.
Health Communication Materials: Flip book, banner, posters on TB, etc., are to be provided and used during these meetings.
Report Writing: At the end of each meeting, a report may be prepared to state the date and time of meetings, number of patients, name of facilitators, presence of MO in the meeting, topics covered/ main points discussed in the meeting, along with major concerns mentioned by the patients.
- The report is to be prepared by the STS.
- The list of patients who attended the meeting may be attached to the report.
- It may be more convenient to have a register at each centre for such meetings, and patients can write their names in the same register.
- These may be submitted by STS to the MO-TC on a monthly basis for onward submission to the District TB Officer (DTO) to be included in the quarterly Performance Monitoring Report (PMR).
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Technical and Operational Guidelines for Tuberculosis Control, RNTCP, 2019.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test How often should patient-provider meetings be conducted? Everyday Twice a year Once every month Once a year 3 Patient-provider meetings can be organised once a month so that each patient who is on treatment has the opportunity to attend one such meeting during the intensive phase. The frequency of such meetings would be more than one in a month when there is a large number of patients at one health facility. Yes Yes
Fullscreen