Evolution of TB Elimination Programme in India
ContentThe National Tuberculosis Control Program (NTP) of India was launched in 1962. It relied on BCG, X-ray based diagnosis and Streptomycin and INH based treatment centralized at district level.
Based on a review of the NTP, and WHO recommendations of the DOTS Strategy, Government of India then revised the NTP and launched new program with the title Revised National Tuberculosis Control Program (RNTCP) in 1997. It used Sputum microscopy at DMC(Designated Microscopy Centres) for diagnosis, and multi-drug Short Course Anti-TB Therapy, decentralized to the TU (TB Unit) level.
In recognition of the rising drug resistance problem the DOTS Plus/ PMDT (Programmatic Management of Drug Resistant TB) was launched in 2006 and scaled up to the entire country by 2012.
Further to strengthen the monitoring and supervision system - a case based notification system - Nikshay was introduced in 2012. The same year Tuberculosis was added as a notifiable disease at the point of diagnosis by all health care providers.
Other key milestones from 2012 to 2020 were the availability of the Standards of TB Care in India (STCI) in 2014, introduction of the Daily weight band wise Fixed Dose combination (FDC) in 2016 and new drugs like Bedaquilline and Delaminid were started in 2017 and 2018 respectively.
To emphasise the commitment of the Government of India and to accelerate the efforts towards TB elimination, RNTCP was renamed as "National Tuberculosis Elimination Programme (NTEP)" in 2020.

Figure: Key milestones under NTEP
Resources:
India's commitment to End TB
ContentThe Government of India has committed to achieving the Sustainable Development Goals(SDG) targets related to ending TB by 2025 (5 years ahead of the global target). This would mean that in 2025, the 2030 target of achieving 80% reduction in incidence, 90% reduction in deaths due to TB compared to that of 2015, is to be achieved.
Parameter 2015 Value SDG 2030 Target Commitment for 2025 Estimated annual Incidence 217 cases/Lakh 80% reduction 44 cases/lakh Estimated annual Mortality 4.5 lakh 90% reduction 45,000 Table: India's commitment to End TB by 2025.
Resources:
National Strategic Plan [NSP] for TB Elimination 2017-25
ContentThe National Strategic Plan (NSP) for TB elimination 2017–25 is a bold strategic framework to drive the acceleration of progress toward TB Elimination, and achieving the Sustainable Development Goal (SDG) and End TB targets for India. It expects to guide the activities of all stakeholders including the national and state governments, development partners, civil society organizations, international agencies, research institutions, private sector, and many others whose work is relevant to TB elimination in India. It is adopts strategies under four groups DETECT, TREAT, PREVENT, BUILD.
VISION: TB-Free India with zero deaths, disease and poverty due to tuberculosis
GOAL: To achieve a rapid decline in burden of TB, morbidity and mortality while working towards elimination of TB in India by 2025.The results framework of the NSP outlines the various targets (impact and outcomes) to be achieved.
IMPACT INDICATORS 2015
(Baseline)2020 2023 2025 1. To reduce estimated TB Incidence rate (per 100,000) 217
(112-355)142
(76-255)77
(49-185)44
(36-158)2. To reduce estimated TB prevalence rate (per 100,000)
320
(280-380)170
(159-217)90
(81-125)65
(56-93)3. To reduce estimated mortality due to TB (per 100,000)
32 (29-35) 15 (13-16) 6 (5-7) 3 (3-4) 4. To achieve zero catastrophic cost for affected families due to TB 35% 0% 0% 0% Resources
Assessment Questions
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct Answer Explanation Part of pre-test Part of post-test Which are the groups under which strategies for National Strategic Plan (NSP) for TB elimination 2017–25 were developed? DETECT, TREAT, PREVENT DETECT, TREAT, PREVENT, BUILD DETECT, TREAT, PREVENT, REHABILITATE DETECT, TREAT, REHABILITATE DETECT, TREAT, PREVENT, BUILD The National Strategic Plan (NSP) for TB elimination 2017–25 adopts strategies under four groups: DETECT, TREAT, PREVENT, BUILD. Yes Yes Which of the following does the National Strategic Plan (NSP) for TB elimination 2017–25 aim to bring down to 0% by 2025? Incidence rate Prevalence rate Mortality rate Catastrophic cost for affected families Catastrophic cost for affected families The target of the National Strategic Plan (NSP) for TB elimination 2017–25 is to achieve zero catastrophic cost for affected families due to TB Yes Yes NTEP Objectives- in relation to NSP 2017-2025
ContentNSP 2012 - 2017 had the aim of achieving universal access to quality diagnosis and treatment. The NSP 2017-2025 which builds on the success and learnings of the last NSP, and articulates the bold and innovative steps required to move towards TB elimination. In 2020, RNTCP was renamed to "National Tuberculosis Elimination Programme" with the following objectives:

Figure: Objectives of NTEP
Resources:
Organizational Structure of NTEP
ContentNational Tuberculosis Elimination Programme (NTEP) is a centrally sponsored programme being implemented under the aegis of National Health Mission.
National Level: Managed by Central TB Division (CTD), the technical arm of the Ministry of Health and Family Welfare (MOHFW)
State Level: State TB Cell coordinates the overall TB elimination programme in state under the guidance of State Health Society. The training ,supervision, monitoring and evaluation NTEP at state level are looked after by STDC (State TB Training and Demonstration Centre).
District TB Centre (DTC) is the nodal point for all TB elimination activities in the district under the guidance of the District Health Society.
Tuberculosis Unit (TU) Level: NTEP activities at block/sub-district level are implemented through TU which comprises Designated Medical Officer (MO) supported by two full-time NTEP staff - STS (Senior Treatment Supervisor) & STLS (Senior TB Lab Supervisor).
PHI (Peripheral Health Institute): PHI is a health facility manned by a Medical Officer (MO). Some of the PHIs are also the Tuberculosis Diagnostic Centres, which are the most peripheral level laboratories in the NTEP structure. All the Private Health Facilities like Private Practitioners / Private Hospitals / Clinics / Nursing Homes are also PHI.

Figure: Organisational structure of NTEP
Resources:
The State TB Cell
ContentThe State TB Cell or STC is the state-level implementing structure of the National TB Elimination Program (NTEP). It is the leading institution for management of NTEP activities at the state level.
The STC is a State Government entity that acts as the bridge between the Central and State Governments for implementing the NTEP. It works under the guidance of the Central TB Division (CTD), and it oversees the program implementation at the districts.
- The State TB Cell is supported by the State TB Training and Demonstration Centre (STDC) for its technical functionalities. STDC mainly supports training, supervision and monitoring.
- The nodal laboratory for the State is the Intermediate Reference Laboratory (IRL). This supports quality assurance of the smear microscopy network and laboratory services in the state.
- The STC has a fully operational State Drug Store (SDS) which is responsible for the effective management and uninterrupted supply of good-quality of medicines and other logistics.
Human Resources at the State TB Cell are:
- State Tuberculosis Officer (STO). A dedicated official from the state health system, at the rank of a Joint Director is designated as the STO and heads the implementation of the NTEP at state level.
- Medical Officer STC (MO-STC): A medical officer from the state health system assists the STO in overseeing various activities.
- State DRTB Coordinator: Assist the STO in DRTB activities monitoring across the districts
- TB - HIV Coordinator: Assist the STO in overseeing TB comorbidities across the district.
- State PPM Coordinator: Looks at the private sector engagement
- State IEC Officer/ACSM Officer: Oversees the implementation of advocacy, communication and social mobilisation activities across different districts.
- STC - Epidemiologist: Assist the STO and STDC Directors by analyzing state-level data and preparing review materials
- Other support staff at the STC include
- Accounts Officer
- Technical Officer-PSM
- Secretarial Assistant
- Data entry operators/Nikshay operator
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Training Modules (5-9) for Programme Managers and Medical Officers, 2020.
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Which of the following statements are true about the State TB Cell (STC)? STC is a state government entity. It is the leading institution for the management of NTEP activities at the state level. It is supported by the STDC. All of the above 4 The STC is a state government entity that is the leading institution for the management of NTEP activities at the state level and is supported by the STDC. Yes Yes State TB Training and Demonstration Centre [STDC]
ContentThe State Tuberculosis (TB) Cell (STC) is supported by the State TB Training and Demonstration Centre (STDC) in many states through its three units – Training Unit, Supervision and Monitoring Unit and an Intermediate Reference Laboratory (IRL). This relationship is shown in the figure below.
- Training Unit: It is involved in estimating the training load, organizing state level training (Induction and Refresher) and evaluating the performance of those who undergo training.
- Supervision and Monitoring Unit: It consists of a team which is dedicated to the supervision of TB elimination activities through supervisory visits, periodic desk review of Nikshay and Nikshay Aushadhi data, and plans state internal evaluations apart from assisting in other supervision and monitoring activities of National Reference Laboratories, Central TB Division and other national/international monitoring missions.
- Intermediate Reference Laboratory: This supports an effective quality assurance system of the sputum smear microscopy network and laboratory services for the programmatic management of drug-resistant TB (molecular drug resistance and culture and drug susceptibility testing) in the state.
The STDC is also involved in operational research.
Human Resources in the STDC
- The STDC functions under the leadership of STDC Director.
Training and Supervision & Monitoring Units:
- 1 Epidemiologist
- 1/more Medical Officer
- 1 Nikshay Operator
- 1 Secretarial Assistant
Intermediate Reference Laboratory (IRL):
- 1 Microbiologist
- 1 Microbiologist- External Quality Assistance (EQA)
- 1 Senior Laboratory Technician- EQA
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, 2020.
- Training Modules (5-9) for Programme Managers and Medical Officers, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
District TB Centre [DTC]
ContentThe key level for the management of public health services is the district level. The District Tuberculosis Centre (DTC) is the nodal point for tuberculosis (TB) control activities in the district.
Functions of the DTC
The primary role of the DTC is a managerial one. The DTC is the central program management unit of the district responsible for all activities related to National TB Elimination Programme (NTEP) implementation such as:
- Advocacy
- Active case finding
- Diagnosis, treatment (both for drug-susceptible and drug-resistant TB cases) and follow up
- Managing comorbidities
- Service delivery
- Maintaining diagnostic and treatment infrastructure
- Setting up Drug-resistant TB (DR-TB) centres
- Ensuring community engagement and TB forums
- Multi-sectorial involvement for drug management, and supervision and monitoring
- Financial management
- Drugs, logistics and supply chain management.
Components of the DTC
- District Drug Store (DDS)
- Nucleic Acid Amplification Test machine (Cartridge Based NAAT or TrueNAT)
- Designated Microscopic Center (DMC)
- Treatment Support Center
- Drug Resistant TB (DR-TB) Center
- X-Ray Unit
With expansion of TB services and ongoing collaboration with various national programs, the structure of DTC is highly integrated as part of general health system and some components may cater to non-TB patients as well e.g., the DMC may be a part of general laboratory, and X-ray unit can be functional for all departments and not just chest/TB section.
Human Resources Deployed at the DTC
The Chief District Health Officer (CDHO) / Chief District Medical Officer (CDMO) / Civil Surgeon or an equivalent functionary in the district is responsible for all medical and public health activities including control of TB.
A full-time District TB Officer (DTO), trained at the national level and based at the DTC, is responsible for planning, training, supervising and monitoring the programme in the district. The DTO is assisted by other technical and secretarial staff:
- Medical Officer- District TB Center
- District DR-TB-HIV Coordinator
- District Public Private Mix Coordinator
- District Program Coordinator
- District Drug Store Pharmacist
- District Data Entry Operator-Nikshay
- District Accountant
- Senior TB laboratory Supervisor
- Senior Treatment Supervisor
- Laboratory Technicians for DMC and NAAT site
- Counsellor for District DR-TB center
- TB Health Visitors
While the National TB Elimination Program (NTEP) approves the above positions through National Health Mission NTEP Project Implementation Plan, the district always has the flexibility for additional resource deployment based on the need and existing epidemic. The DTO and his/her team are supported by various other program officers/staff and non-governmental organizations working in the field for Tuberculosis and Health.
Resources
- NTEP Training Modules 1-4 for Programme Managers & Medical Officers, 2020.
- NTEP Training Modules 5-9 for Programme Managers & Medical Officers, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Tuberculosis Unit [TU]
ContentTuberculosis (TB) unit (TU) is the sub-district level supervisory unit of National TB Elimination Program with the following organogram:
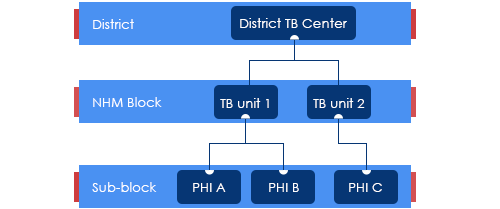
Figure: Organogram of a TB Unit
(PHI: Peripheral Health Institution)
TUs are based mainly on National Health Mission (NHM) health blocks with the aim of aligning with the NHM Block Programme Management Unit (BPMU) for optimum resource utilization and appropriate monitoring.
The TUs have been created based on a population of 1 per 2,00,000 (range 1.5 – 2.5 lakh) for rural and urban populations and 1 per 1,00,000 (0.75 – 1.25 lakh) population in hilly/tribal/difficult areas.
The TU consists of a designated Medical Officer-Tuberculosis Control (MO-TC), as well as one full-time supervisory staff - Senior Treatment Supervisor (STS). However, one Senior TB Laboratory Supervisor (STLS) will be there in every 5 lakh population (one per 2.5 lakh population for tribal/hilly/difficult areas), mostly covering 2-3 TUs.
TB Unit manages the provision of TB services (Diagnosis, Treatment, Prevention, etc.) and programme management in the assigned geographical area.
Resources
Peripheral Health Institutions [PHI] and Health Facilities
ContentUnder the National Tuberculosis Elimination Programme (NTEP), a Peripheral Health Institute (PHI) is a health facility that is manned by at least a Medical Officer (MO), where diagnosis and management of Tuberculosis (TB) are done.
At this level, there are dispensaries, Primary Health Centres (PHCs), Community Health Centres (CHCs), referral hospitals, major hospitals, speciality clinics or hospitals (including other health facilities), TB hospitals, Anti-retroviral Treatment (ART) centres and medical colleges within the respective district.
All health facilities in the private and Non-government Organisation (NGO) sectors participating in NTEP are also considered PHIs. Some of these PHIs also function as Designated Microscopy Centres (DMCs).
Role of PHIs in Program Management for TB Elimination
- PHIs undertake tuberculosis case-finding and treatment activities as a part of the general health services.
- In situations where more than one MO is posted in any of the PHC, one of them may be identified and entrusted with the responsibilities of the NTEP.
- Additionally, NTEP provides 1 TB Health Visitor (TBHV) per one lakh urban population to support the urban TB control activities in urban settings/ medical colleges.
Resources
DR-TB Centres and Network
ContentDrug-resistant Tuberculosis Centres (DR-TBCs) are specialized centres for the clinical management of Drug-resistant TB (DR-TB).
Each DR-TBC needs to have established a DR-TB committee to carry out the clinical management of DR-TB patients.
DR-TBCs can be established in the public sector where appropriate facilities are available.
- The DR-TBC can also be established in the private sector on mutually agreeable terms and conditions based on the Guidance Document on Partnerships, 2019.
District level: There are District Drug-resistant TB Centres (DDR-TBCs) to manage DR-TB cases. These centres will function under the guidance of Nodal Drug-resistant TB Centres (NDR-TBCs). Almost every district has a mandate to establish a DDR-TBC in India. There are around 620 DDR-TBCs established in the country.
State/ Regional level: At the state/ regional/ division level, there are NDR-TBCs to manage seriously ill DR-TB cases. There are 173 NDR-TBCs established in India.
Decentralized DR-TB services through an expanded network of DR-TB centres has helped the National TB Elimination Program in improving access to DR-TB services and has also resulted in improved DR-TB treatment linkage and better management of DR-TB patients.
Resources
Drugs Stores in NTEP
ContentImage
DRUG STORE
Central TB Division, MoHFW, has
Under NTEP, there is a large network of drug stores across the country to ensure a regular and uninterrupted supply of drugs and consumables. The Drugs and consumables are procured at the Central level and supplied at Central warehouses (GMSDs & CMSS); further drugs and consumables are supplied to the State Drug Stores and further dissemination to district and sub-district levels following the stocking norms to ensure uninterrupted supply of drugs and consumables to the patient.
To provide overall policy guidance and coordination, the Procurement and Supply Chain Management (PSM) Unit has been established at Central TB Division (CTD), MoHFW, for procurement and Supply Chain Management of all types of anti-TB drugs, diagnostics and consumables.
Standards of TB Care in India
ContentThe Standards for TB Care in India (STCI), which is a locally customized version of the International Standards of Tuberculosis Care, mentions 26 standards that every citizen of India should receive irrespective of the sector of treatment.
STCI were developed based on a series of discussions involving various stakeholders including clinicians, public health specialists, community workers and patient advocates.
STCI represent what is expected for quality TB care from the Indian healthcare system including both public and private systems.
It was first published in 2014 and outlines standards across the four themes of TB diagnosis, TB treatment, public health action and social inclusion.
Following are the list of the 26 Standards:

Table 1: Categorisation of the Standards for TB Care in India, Source: Standards for TB Care in India, World Health Organisation, pp. 13-23
Resources
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test How many standards in TB care are described in the Standards of TB Care in India (STCI) 2014? 4 15 26 32 3 There are 26 standards for TB care under four major categories: diagnosis, treatment, public health actions and social inclusion. Yes Yes Stages in TB Patient's Lifecycle
ContentThose who are suspected of having TB disease are first screened for symptoms like cough and fever for more than 2 weeks, blood stained sputum and weight-loss. If found positive on screening, then TB patients are referred for testing to the nearest health facility. If diagnosed with TB, then they are subsequently initiated on treatment. The TB patients initiated on treatment are regularly monitored with the help of field staff or digital interventions like 99DOTS and MERM (Medication Event Reminder Monitor) technology. NTEP staff also ensures that the TB patients are regularly followed up on monthly basis till their treatment completion.

Figure: Patient Flow
Kindly provide your valuable feedback on the page to the link provided HERE
Fullscreen