Drug-Resistant Tuberculosis(DR-TB)
ContentWhat is Drug-Resistant Tuberculosis?
-
Drug-Resistant TB occurs when bacteria become resistant to the drugs used to treat TB. This means that the drug can no longer kill the TB bacteria.
-
Multidrug-resistant TB (MDR TB) is a type of DR-TB where TB bacteria is resistant to both Isoniazid and Rifampicin, the two most potent anti-TB drugs.
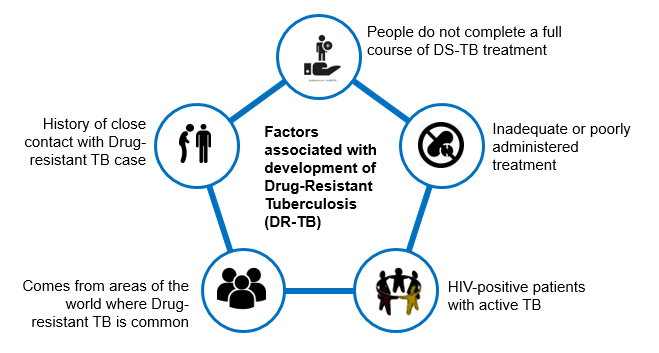
Figure: High Risk for Drug-Resistant Tuberculosis (DRTB)
Resources:
-
Goals of DR-TB Treatment
ContentGoals of Drug-resistant Tuberculosis (DR-TB) treatment under the National Tuberculosis Elimination Program (NTEP) are as follows:
Image

Figure: Goals of DR-TB Treatment; Source: Guidelines for PMDT in India, March 2021, p41.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- Technical and Operational Guidelines for TB in India, 2016.
Kindly provide your valuable feedback on the page to the link provided HERE
Screening for DR-TB
ContentAll patients diagnosed with TB should have universal access to rapid DST for at least Rifampicin and further DST for at least Fluoroquinolones among all TB patients with rifampicin resistance, i.e. UDST.
UDST tests are offered preferably before treatment initiation to a maximum within 15 days from diagnosis. Based on the UDST test result, if Rifampicin resistance is detected, the patient is shifted to DR-TB Treatment Regimen. If Rifampicin resistance is not detected, then first-line anti TB treatment is continued, and the patient is screened further on their follow-ups. If tested positive in sputum examination during any patient follow up, then sputum is sent for further drug resistance testing, and the patient is referred to PHI for follow-up.
Figure: Screening of patient for initiating DRTB Treatment from DSTB Treatment
Types of Drug Resistance Tuberculosis -DRTB
ContentResistant Sensitive
Unknown / Sensitive Types of Drug Resistance TB (DR TB) Resistance to Isoniazid (H) Resistance to Rifampicin (R) Resistance to Fluroquinolone (FQ)
- Ofloxacin,
- Levofloxacin,
- Moxifloxacin
Resistance to Group A Drugs
- Bedaquiline or
- Linezolid
H Mono / Poly Drug Resistance
- Resistant to Isoniazid (H)
- Sensitive to Rifampicin (R)
- Unknown / Sensitive to Fluoroquinolone (FQ) or Group A Drugs - Bedaquiline or Linezolid
Rifampicin Resistance (RR)
- Resistant to Rifampicin (R)
- Unknown / Sensitive to other drugs
Multi Drug Resistance TB (MDR TB)
- Resistant to Isoniazid (H) and Rifampicin (R)
- Unknown / Sensitive to Fluoroquinolone (FQ) or Group A Drugs - Bedaquiline or Linezolid
Pre-Extensive Drug Resistance (Pre -XDR)
-
Resistant to Isoniazid (H), Rifampicin (R) and any Fluroquinolone (FQ)
- Sensitive/ Unknown to Group A Drugs - Bedaquiline or Linezolid
Extensive Drug Resistance (XDR)
- Resistant to Isoniazid (H) , Rifampicin (R) and any Fluoroquinolone (FQ) and at least one additional Group A Drugs - (presently to either Bedaquiline or linezolid [or both])
Resources:
DR-TB Treatment Regimens
ContentDepending upon type of drug resistance, there are four broad DRTB Treatment regimen.
- H Mono/Poly Treatment Regimen(6-9 months)
- Shorter oral Bedaquiline containing MDR/RR-TB regimen(9-11 months)
- Shorter injectable containing regimen(9-11 months)
- Longer oral M/XDR-TB regimen(18-20 months)
Drugs administered for DRTB Regimen:
- Drugs are decided based on the drug resistance detected for a patient and will be informed by the medical officer.
- Injections might also be administered to the admitted patient.
- H Mono/Poly Regimen can be initiated at any health facility, while the other two regimen need to be initiated at N/DDR-TB Centre
Figure: Patient wise boxes(PWB) for DRTB Treatment
Pre-treatment Evaluation [PTE] of DR-TB Patients
ContentPTE Objective
Drugs used for the treatment of drug-resistant TB have significant adverse effects. Hence, there is a need for PTE to rule out any underlying condition at the baseline, like co-morbid conditions, radiological abnormalities, Electrocardiogram (ECG) changes, or biochemical derangements.
PTE is essential to identify:
- The patient's eligibility for initiation of a particular regimen
- Patients who require special attention during treatment
- Regimen modifications from the beginning of treatment
Table: Pre-treatment (PTE) for MDR/RR-TB patients Clinical Evaluation Lab based evaluation History and Physical Examination Random blood sugar (RBS) Height HIV testing following counselling Weight Complete blood count (Hb, TLC, DLC, platelet count) Psychiatric evaluation if required Liver function tests (including serum proteins) TSH levels Urine examination – routine and microscopic Serum electrolytes (Na, K, Mg, Ca) Urine pregnancy test (in women of reproductive age group) Chest X-ray ECG Important Points
- In the majority of Multidrug-resistant (MDR)/ Rifampicin-resistant Tuberculosis (RR-TB) patients, PTE can be done on an outpatient basis.
- The District TB Officer (DTO) and Medical Officer of the TB Unit (MO-TU) can arrange for PTE at the Nodal and District DR-TB Centre (N/DDR-TBC) or at the sub-district level health facility, wherever feasible.
- No additional investigations are required for H Mono/ Poly DR-TB patients unless clinically indicated.
- The PTE carried out at the time of treatment initiation can be considered valid for 1 month from the date of the test result and the patient can be re-initiated on a subsequent regimen considering the previously conducted PTEs.
- Active Drug Safety Management and Monitoring (aDSM) treatment initiation forms are required to be completed for all DR-TB patients at the time of initiation of each new episode of treatment.
- PTE should include a thorough clinical evaluation by a physician and expert consultation as per the need.
- Laboratory-based tests should be performed based on the drugs used in the treatment regimen.
- Pre-treatment evaluation should be made available free of charge to the patient.
Resources
Second Line anti TB drugs
ContentThe anti-TB drugs recommended for treatment of Multi- and Extensively Drug-resistant (M/XDR) TB patients are grouped into three groups – A, B and C (Figure below).
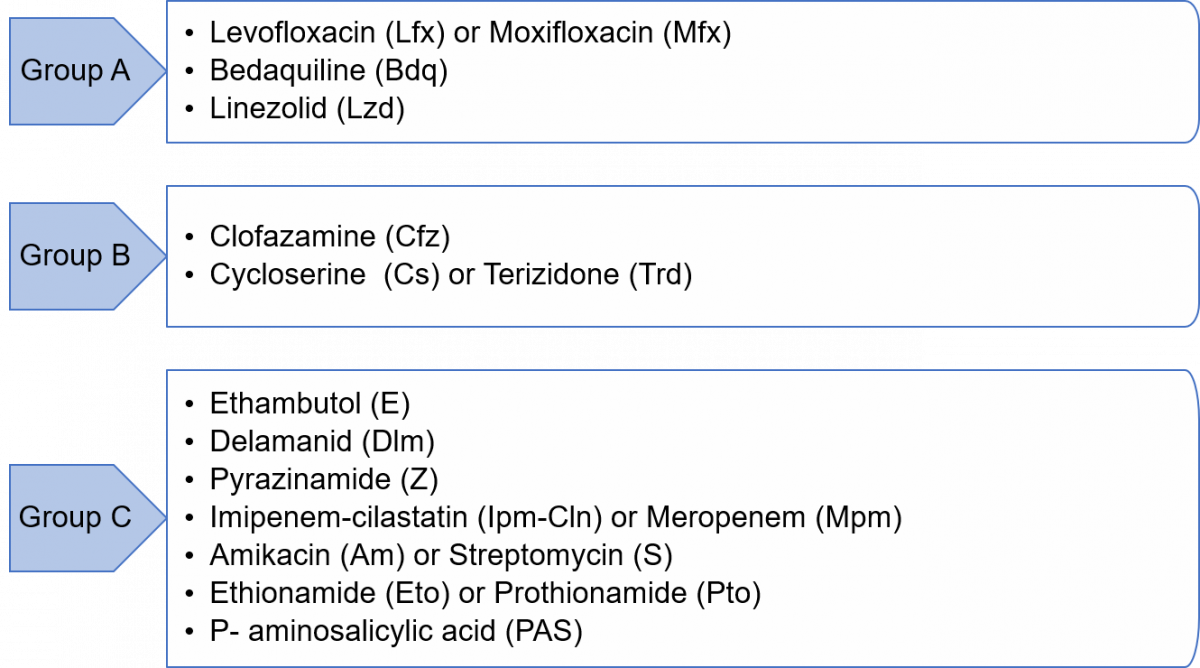
Figure: Groups A, B and C of Anti-TB Drugs used in Treatment of M/XDR-TB Patients
Grouping of drugs is done based on their efficacy, experience of use and drug class. This grouping is intended to guide the design of individualized, longer M/XDR-TB regimens (the composition of the recommended shorter MDR/RR-TB regimen is largely standardized).
Resources
- Guidelines for Programmatic Management of Tuberculosis in India, 2021.
- WHO Consolidated Guidelines on Tuberculosis, Module 4 - Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Newer Anti-TB Drugs
Content
Figure: Sirturo 100 mg Bedaquiline Tablets
- Newer anti-TB drugs are needed to improve the treatment outcomes of DR-TB, shorten the duration of treatment, address the problem of drug resistance, and have less toxic drugs.
- Five decades after the discovery of Rifampicin, two newer drugs with anti-TB effects were approved for the treatment of multidrug-resistant tuberculosis (MDR-TB) by the Central Drugs Standard Control Organization (CDSCO). These are:
- Bedaquiline (Bdq)
- Delamanid (Dlm)
- In July 2020, the Drug Controller General of India (DCGI) also approved a third newer drug - Pretomanid (Pa) to use under the Conditional Access Programme (CAP) under the National Tuberculosis Elimination Program (NTEP).
Resources
- The Use of Bedaquiline in the Treatment of Multidrug-resistant Tuberculosis, Interim Policy Guidance, WHO, 2013.
- The Use of Delamanid in the Treatment of Multidrug-resistant Tuberculosis in Children and Adolescents, Interim Policy Guidance, WHO, 2016.
- WHO Consolidated Guidelines on Tuberculosis, Module 4: Treatment- Drug-resistant TB Treatment.
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
Kindly provide your valuable feedback on the page to the link provided HERE
Weight Band-wise Dosages of DR-TB Drugs for Adults
ContentThe dosage for Drug-resistant TB (DR-TB) drugs used in the regimen by weight bands for adults are enumerated in the table below.
Table: Weight Band-wise Drug Dosage of DR-TB Drugs for Adults; Source: Guidelines for PMDT, India 2021, pp.51,64. SR NO
DRUGS 16-29 KG 30-45 KG 46-70 KG >70 KG 1 Levofloxacin (Lfx) 250 mg 750 mg 1000 mg 1000 mg 2 Moxifloxacin (Mfx) 200 mg 400 mg 400 mg 400 mg 3 High dose Mfx (Mfxh) 400 mg 600 mg 600 mg 600 mg 4 Bedaquiline (Bdq) Week 0–2: Bdq 400 mg daily
Week 3–24: Bdq 200 mg 3 times per week
5 Clofazimine (Cfz) 50 mg 100 mg 100 mg 200 mg 6 Cycloserine (Cs)3 250 mg 500 mg 750 mg 1000 mg 7 Linezolid (Lzd) 300 mg 600 mg 600 mg 600 mg 8 Delamanid (Dlm) 50 mg twice daily (100 mg) for 24 weeks in 6-11 years of age
100 mg twice daily (200 mg) for 24 weeks for ≥12 years of age
9 Amikacin (Am)1 500 m 750 mg 750 mg 1000 mg 10 Pyrazinamide (Z) 750 mg 1250 mg 1750 mg 2000 mg 11 Ethionamide (Eto)3 375 mg 500 mg 750 mg 1000 mg 12 Na - PAS (60% weight/ vol)2,3 10 gm 14 gm 16 gm 22 gm 13 Ethambutol (E) 400 mg 800 mg 1200 mg 1600 mg 14 Imipenem - Cilastatin (Imp-Cln)3 2 vials (1 g + 1 g) bd (to be used with Clavulanic acid) 15 Meropenems (Mpm)3 1000 mg three times daily (alternative dosing is 2000 mg twice daily 16 Amoxicillin-Clavulanate (Amx-Clv) (to be given with Carbapenems only) 875/125 mg bd 875/125 mg bd 875/125 mg bd 875/125 mg bd 17 High-dose H (Hh) 300 mg 600 mg 900 mg 900 mg 18 Rifampicin (R) 300 mg 450 mg 600 mg 750 mg 19 Pyridoxine (Pdx) 50 mg 100 mg 100 mg 100 mg 1For adults more than 60 yrs of age, dose of Second Line Injectable (SLI) should be reduced to 10 mg/kg (max up to 750 mg)
2In patients on Para-aminosalicylic Acid (PAS) with 80% weight/volume the dose will be changed to 7.5 gm (16-29 kg); 10 gm (30- 45 kg); 12 gm (46-70 kg) and 16 gm (>70 kg)
3Drugs can be given in divided doses in a day in the event of intolerance
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-resistant Tuberculosis, 2014.
Kindly provide your valuable feedback on the page to the link provided HERE
Treatment of DR-TB in Children
ContentThe principles of designing Drug-resistant TB (DR-TB) treatment regimens (Shorter or longer oral Multi (M)/ Extensively Drug-resistant TB (XDR-TB), and H mono/ poly DR-TB regimens in children are similar to adults:
- Children, aged 5 years to less than 18 years of age and weighing at least 15 kg, are eligible for both longer oral and shorter oral Bedaquiline-containing Multidrug-resistant (MDR)/ Rifampicin-resistant TB (RR-TB) regimens.
- Management of H mono/ poly DR-TB in children will be the same as in adults and child-friendly formulations can be used.
- The drug doses should be used as per paediatric weight bands.
- Bedaquiline (Bdq) tablets suspended in water have been shown to have the same bioavailability as tablets swallowed whole and therefore, should be used to treat DR-TB in children until a child-friendly formulation becomes available.
- Delamanid (Dlm) is already approved for treating M/XDR-TB under the National TB Elimination Programme (NTEP) for children from 6 years onwards.
- As in adults, the extension of Bdq beyond 6 months and concomitant use of Bdq and Dlm in special situations will apply to children as well.
- Treatment can be directly extended to 9 months in certain conditions like extensive disease, extrapulmonary TB, uncontrolled comorbidity, smear-positive cases at the end of the 4th month and when the regimen is modified.
- Shortening the total treatment duration to less than 18 months may be considered in children without the extensive disease.
- For children under 5 years of age, where neither Bdq nor Dlm is approved yet, the longer oral M/XDR-TB regimen should be suitably modified as per the replacement drug. A suitable regimen can be designed considering child-friendly formulations where Bdq can be replaced with Amikacin (Am), Pyrazinamide (Z) or Ethionamide (Eto) in the initial phase.
- Children below 5 years are not excluded from short-course regimens, instead receive short course injectables till further evidence on the use of Bdq is available.
- The use of injectable agents in children should be exceptional and limited to salvage treatment and be monitored for early detection of ototoxicity.
- Meropenem is the preferred drug over imipenem in TB meningitis considering the risk of seizures in children due to Imipenem.
Additional Information
- Achieving an appropriate dose in children aged 3-5 years will be easier when the special formulation dispersible 25 mg tablet used in trials in these age groups becomes available.
- The recent data review for the World Health Organization (WHO) guidelines suggested that there are no additional safety concerns for concurrent use of Dlm with Bdq.
- For treatment and management of adverse drug reactions in children, there should be provision for treatment in consultation with a specialist.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- Consolidated Guidelines on Tuberculosis: Module 4 - Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Adverse Drug Reactions(ADRs) to Second Line Treatment
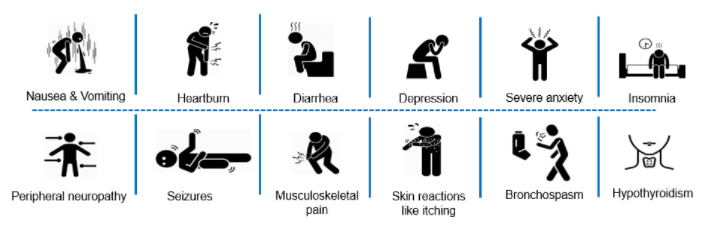
ContentCommon Adverse events to second line treatment are as below
Figure: Adverse Drug Reaction to Second line drugs
Adverse events should be identified, monitored and be referred to
- Nearest treating doctor for minor symptoms or
- District DR-TB Centres for major symptoms
If required, hospitalization can be done at the District DR-TB Centers where inpatient facility is available or referred to a Nodal DRTB Centre for admission
Reporting of Adverse Events and Serious Adverse Events
ContentAll serious and non-serious adverse events which are possibly, probably or very likely related to any anti-TB drug need to be reported by the physician to the National TB Elimination Programme (NTEP).Serious Adverse Events (SAE) needs to be reported to the nearest ADR monitoring centre (AMC) and Central TB Division (CTD) within 24 hours. Any death of a patient occurring during treatment, regardless of causality, must be reported as an SAE.
aDSM-treatment review form to be filled whenever the DR-TB patient develops any SAE
- The primary responsibility of filling up the aDSM forms will be with the nodal officer of the DR-TB centre with the help of a senior medical officer (SMO) or medical officer (MO) designated.
- It is essential that Nikshay data entry are being done on regular basis by statistical assistant at the NDR-TBC and senior DR-TB TB-HIV supervisor at the DDR-TBC centre.
- Forms should be maintained in hard copies until the ADR module is active in Nikshay.
Once relevant forms of aDSM are filled in Nikshay, information is directly communicated to the pharmaco-vigilance programme of India (PvPI) through the Vigiflow=connecting bridge for signal generation.
Resources
Fullscreen