-
CHO-CH25: Guidelines and Protocols for ACSM activities
FullscreenOrganising Community meetings
ContentCommunity meetings are organised by the Senior Treatment Supervisor (STS) or the partner Non-Government Organisation (NGO) under the supervision of the Medical Officer.
- These meetings are conducted to create awareness about TB among the general population, community leaders, people’s representatives, Self-help Groups (SHGs), community volunteers, traditional healers, etc.
- These meetings are organised in a community centre or any other suitable place at the village and slum level.
- To maximise the output, the community meetings should be planned appropriately.
Following are the steps involved in planning a community meeting:
Image
Resources
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Who supervises the conduct of community meetings? DTO STO MO STLS 3 Community meetings are organised by the STS or the partner NGO under the supervision of the Medical Officer. YES YES Community mobilization strategies-Tribal areas
ContentTribal people (10.4 Cr, 8.6% of total population) have higher prevalence (703 per 100,000) of TB compared to national average (256 per 100,000).10.4% of all TB notified patients are from tribal communities. The National TB program has prioritized this subgroup of population through Tribal Action Plans since 2005.
As a part of the Multisectoral collaboration with various Ministries, a guidance note on the joint action plan was developed by Ministry of Health and Family Welfare (MoHFW) and Ministry of Tribal Affairs in October 2020 and shared with the Secretaries of all States/ UTs for field level implementation. Tribal TB initiative, a unique partnership between the Ministry of Health and Family Welfare and Ministry of Tribal Affairs was initiated to improve the cascade of TB care and support services among Tribal Populations in India. The technical assistance for this initiate will be provided by USAID.
Challenges in communities in tribal areas:
Access, availability, and utilization of TB care services of these communities are hindered by:
- Geographical barriers
- Poor state of social determinants
- High impact of malnutrition, insufficient community involvement
- Health system constraints including lack of trained human resources
- Cultural and communication gaps between the care provider and the community, etc.
- The COVID-19 pandemic has probably further worsened the situation.
Community mobilization strategies in tribal areas:
Image
Various departments which play a role in community mobilization in Tribal areas:
- National Program Management Unit (NPMU) provides technical assistance in monitoring and implementation of the Tribal TB Initiative.
- Coordination among National Tuberculosis Elimination Programme (NTEP), National Health Mission (NHM), Ministry of Development of Northeastern Region, Ministry of Tribal affairs at National, state and district levels through national level Technical Support Unit.
Image
- Coordination with ‘Centre of Excellence’ within the Ministry of Tribal Affairs, with a key focus on TB.
- Partnering with private sector players for leveraging resources for TB elimination in Tribal communities.
- Documenting best practices, and commission tribal health research studies in collaborations with identified government institutions.
- Various departments collaborate for improving the operational excellence of existing demand-side interventions such as Village Health Sanitation and Nutrition Days (and committees), Jan Arogya Samiti platforms, Jan Andolan initiatives, engaging TB-Champions, and training of faith healers and other community influencers.
Resource
Assessment
Question Answer
1
Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Community mobilization strategies in tribal areas include home visits. True False 1 Community mobilization is about seeking cooperation and support from different stakeholders in general and the community in specific.
Home visits will improve awareness on various government schemes, provisions, facilities available for TB patients and to improve treatment literacy and adherence among TB patients in tribal areas.
Community mobilization strategies-Rural areas
ContentRural populations have more limited access to primary care physicians than residents of urban areas, and are older, sicker, and poorer than urban counterparts. Travel to reach a primary care provider may be costly and burdensome for patients living in remote rural areas, with subspecialty care often being even farther away. These patients may substitute local primary care providers for sub specialists, or they may decide to postpone or forego care. Many social determinants act as barriers for rural communities to access health services.
Challenges faced by communities in rural areas are:
- Higher poverty rates, which can make it difficult for participants to pay for services or programs
- Cultural and social norms surrounding health behaviors
- Low health literacy levels and incomplete perceptions of health
- Linguistic and educational disparities
- Limited affordable, reliable, or public transportation options
- Unpredictable work hours or unemployment
- Poor primary healthcare and infrastructure in rural areas
- Lack of access to tuberculosis testing and treatment centers in remote unreached areas
- Unregulated indigenous system of medicine
- Poor airborne infection control
- Poor nutrition and Malnourishment
Community mobilization strategies in rural areas include:
Image
Various committees which play a role in community mobilization in rural areas:
Image
- Village Health Sanitation and Nutrition Committees (VHSNCs) - In each Gram Panchayat, Village Health Sanitation and Nutrition Committees (VHSNCs) have been formed at the village level under National Health Mission (NHM). These committees are entrusted with community-level planning and implementation of health and sanitation, and have representation from the local government, local health centre, and the local community.
- Panchayat Raj Institution (PRI) - Members of PRI refers to local self-government at the village level. The village pradhan (head) and members of the Panchayat are elected members of the Gram Panchayat. They are the key people who can, after sensitization, mobilize the community for TB care and control and make allocations for TB patients’ nutrition and travel requirements.
- Yuva mandal/Mahila mandals (Youth/women’s clubs) - Community-level federations of young boys/girls/women, sometimes even comprising several women SHGs.
- Self-help groups (SHG) - An SHG is a group of individuals with a homogenous social and economic background, who voluntarily come together to regularly save small amounts of money and contribute to a local fund to meet the members’ emergency needs on a mutual help basis. These groups collectively manage their payments and ensure proper use of credits. Many NGOs currently engaged in the project are involved in formation/registration of these SHGs. It would be advisable to involve these NGOs for ease of implementation.
- Community-based organizations (CBO) - A CBO is a small group of people from a community, who come together for a particular purpose. It may be a local association of people mobilized around water conservation, mother and childcare, sustainable agriculture, education, or adolescent health; a group of social service persons; or any other such active group in a village.
Resource:
Assessment:
Question
Answer
1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Community mobilization strategies in rural areas includes empowering key decision-makers, people affected by TB, and marginalized and vulnerable populations.
True
False
1
This leads to raising awareness of services available and general health literacy surrounding TB.
More people accessing public health services will lead to better utilization of services.
- Higher poverty rates, which can make it difficult for participants to pay for services or programs
-
CHO-CH26: Community Engagement
FullscreenCommunity Engagement
ContentCommunity engagement is a process of developing relationships that enable stakeholders to work together to address health-related issues and promote well-being to achieve positive health impact and outcomes.
Mobilize communities to engage them in TB care and to increase ownership of the Programme by communities.
Why Community Engagement?
Figure: Importance of Community Engagement
Importance of Community Engagement in TB
ContentCommunity-based TB activities are conducted outside the premises of formal health facilities (e.g. hospitals and clinics) in community-based structures (e.g. schools and places of worship) and homesteads. Community health workers and community volunteers carry out community-based TB activities. Both can be supported by nongovernmental organizations and/or the government.
Community Engagement is a cost effective intervention to improve health service coverage and deliver accessible and people-centered integrated care.
Figure: Importance of Community Engagement
TB Champion
ContentA TB Champion is a person who has been affected by TB and successfully completed the treatment.
TB Champions, in their capacity as survivors, are role models and can provide valuable support to those with TB and their families.
Figure: Roles of TB Champion
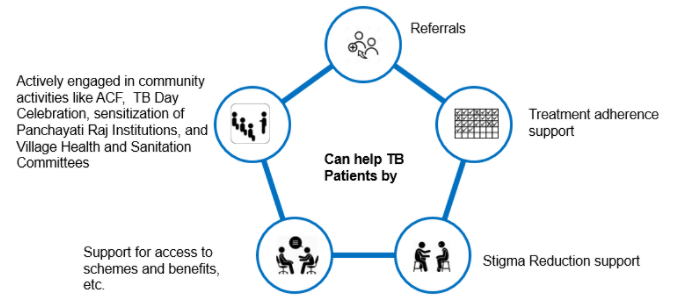
Community Health Volunteers should identify TB Champions and engage them to provide their support to the patient in activities like:
Figure: Help to TB Patients by Community Health Volunteers
-
CHO-CH27: Social Inclusion and wellness activities
FullscreenSocio economic factors affecting TB patients
ContentSocio-economic factors affecting TB patients are:
1. General socioeconomic conditions of the society, culture and environment. This includes:
-
Gross Domestic Product (GDP)
-
Immigration
-
Urbanisation
-
Incidence of TB in the country
-
Labour policy
-
Access to healthcare
2. Socioeconomic position of the individual. This includes:
-
Income
-
Education
-
Occupation
-
Social class/ caste
-
Indigenous/ tribal population
-
Gender
3. Living and working conditions. This includes:
-
Housing conditions (overcrowding and poor ventilation especially in night shelters, de-addiction centres, old age homes, prisons)
-
Employment conditions - Occupation with risk of developing TB (mines, coal industry, sand blasting industries, weaving & glass industries, stone-crushers, cotton mill workers, tea garden workers, rice mill workers, etc.,)
-
Homelessness
-
Hard to reach areas
-
Urban slums
3. Psychosocial risk factors, such as:
-
Social exclusion
-
Depression
4. Individual lifestyle risk factors, such as:
-
Smoking
-
Alcohol abuse
-
Tobbaco use
-
Drug abuse
-
Nutrition (malnutrition)
-
Co-morbidities like diabetes mellitus, malignancies, patients on dialysis and on long term immunosuppressant therapy HIV, past history of TB
Resources
- NTEP Training Modules (1 to 4) for Programme Managers & Medical Officers, CTD, 2020.
- Social Determinants of Tuberculosis Context Framework and the Way Forward to Ending TB in India, IPH, India, 2020.
Assessment
Question
Answer
1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Socio-economic factors affecting TB patients are:
-
Housing
-
Income
-
Access to healthcare
-
Alcohol abuse
1,2
2,3,4
1,2,3,4
1,2,4
3
TB is one of the few diseases which reflects and expresses social inequalities. Living conditions, economic conditions, lifestyle, and access, affordability, and availability of healthcare are factors which affect TB patients.
-
Stigma and Discrimination towards TB Patient
ContentStigma is when someone sees you in a negative way.
Discrimination is when someone treats you in a negative way.
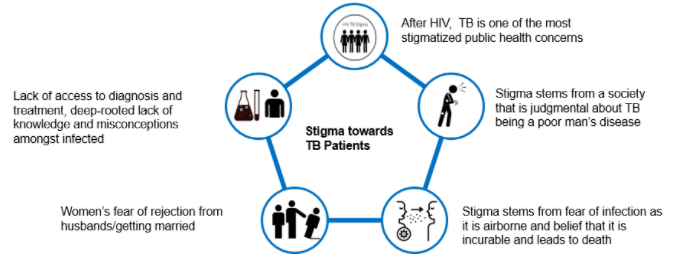
TB patients face various forms of stigma and discrimination in the community
Figure: Stigma towards TB Patients in the community
Socio-Economic Determinants for Tuberculosis
ContentSocioeconomic determinants of health include the conditions in which people are born, grow, live, work, and age. These determinants play an important role in increasing the risk of acquiring TB infection, its progression into active TB disease and further transmission to contacts.
Socio-economic factors affect health-seeking behaviour and access to TB services
Figure: Socioeconomic factors that are affecting the health of TB patients
There may be difficulties in transportation to health facilities and lack of social support to seek care when they fall sick. This delays the contact with health systems for appropriate diagnosis and initiation of treatment.
Effects of Stigma on TB Patients
ContentAt Individual Level
- Lack of self-esteem and confidence
- Increased sense of emotional isolation, feeling of guilt and anxiety
- Physical as well as financial debilitation
- People, more often women, are forced to leave their homes
- Concealing symptoms and hesitancy in seeking medical care making disease management more difficult
- Delayed diagnosis, interrupted treatment that can lead to further transmission and DRTB
- Vulnerability increases, can lead to suicidal thoughts due to isolation and shame
At Family and Community Levels
- Loss of household earnings
- Exposure of caregivers to the risk of infection that lowers productivity and cycle of poverty further gets perpetuated
- Isolation and stigmatization of infected persons often by people of their community
- Deep-rooted lack of knowledge and misconceptions among the affected and infected within their cultural and religious environment
- Loss of status and negative impact on those with the disease, their caregivers, family, friends and communities
- Perceived and internalized stigma of the community due to socio-cultural values that TB is punishment for sins or transgression
Gender Aspects of TB
ContentAlthough more men are affected by TB, women and transgender persons experience the disease differently. Gender differences and inequalities play a significant role in how people of all gender access and receive healthcare services.
Gender difference in Men Women Incidence of TB - Higher proportion of men(approximately- 2:1) are diagnosed with TB than women
- More likely to have microbiologically confirmed Pulmonary TB
- More likely to have Clinically diagnosed pulmonary TB and extra – pulmonary forms of TB
- Prevalence of HIV-TB co-infection is higher among women who live in overcrowded houses and consume alcohol
- High Risk for developing TB – Pregnant women and women in the postpartum period
Exposure, Risk & Vulnerability - Smoking and alcohol consumption among men
- High risk for developing TB - employment in mining, quarrying, metals and construction industries
Undernutrition, their role as caretakers and the use of solid fuel for cooking puts women at risk for TB Health Seeking & Health system factors - Fear of loss of income and the consequences of absence from work hinder care seeking.
- Women face difficulties due to perceived stigma, prioritization of household chores, lack of money or financial dependence
Treatment Outcomes - Pressure to get back to work and lifestyle habits such as smoking or consumption of alcohol influence discontinuation of treatment in men
- Migrant workers, mostly men, often face difficulties in adherence to treatment in the face of extreme poverty and issues of daily survival
- Women tend to have better adherence and treatment outcome as compared to men
- Stigma and discrimination are major impediments to treatment adherence, mainly among unmarried women, newly married women and the elderly
Transgender population often has low literacy, low education levels and are poor. A high proportion of transgender persons are known to smoke, consume alcohol and use drugs. All these factors make them vulnerable to TB.
Addressing Gender Inequalities
ContentBroad principles to address gender inequalities in TB care
- Confidentiality of patient needs to be maintained
- Non-discrimination and non-stigmatising behaviour to be promoted
- Respect for all to be ensured
- Informed consent and informed treatment
- Accountability to be fixed for actions and inactions
- Access for all health services
- Rights-based approach
- Empowered communities - Ensure representation of women, men and transgender persons in all forums
- Work in partnership - Strengthen linkages between program, private sector and communities
Wellness Activity for TB Patients
ContentYoga
- Yoga aims at holistic functioning of the mind and body. It consists of various exercises and specific body positions and movements(yoga asana) which can be learnt and performed under the supervision of a yoga teacher.
- Yoga will help to clean the upper respiratory tract and the sinuses. The breathing exercise or pranayama induce relaxation and help to reduce the stress levels of the patients considerably.
Meditation
- Meditation is a practice where an individual uses a technique – such as mindfulness, or focusing the mind on a particular object, thought, or activity – to train attention and awareness, and achieve a mentally clear and emotionally calm and stable state.
Exercise
- Exercise is being recognized as an important modality for gaining good health and recovering from illness and disease.
- Exercise like cycling and walking are great ways to make sure that the TB infection that was once in your system has been completely eradicated. Once recovered, it is a good idea to keep up the exercise, as this is a factor in stopping the TB from returning at a later date.
-
Rehabilitation Service to TB Patients
- Emotional support must be provided to patients with TB and their families during illness. Receiving TB diagnosis is often regarded by patients as a real stigma that isolates them from their family and society. Psychologists can support patients to help reduce misconceptions and socially integrate former patients.
- TB is a contagious disease that induces fear and social isolation and needs a long period of drug administration, sometimes with adverse effects. Therefore, therapeutic education is very important, which serves the purpose of explaining to patients and their families about the condition of the disease, the risks of contagiousness, the stages of treatment and prognosis.
- Exercise may be light initially, followed by assisted and active exercise. Once the patient’s condition is stable, a 6-minute walk test may be done in the room or corridor. The intensity should be progressively increased, depending on the patient’s tolerance.
- Nutrition: Weight loss is associated with fatigue and decreased exercise capacity. There is a risk for the patient not recovering body weight at the end of drug therapy, despite receiving correct TB treatment. Nutritional supplementation may play a positive role in the recovery of these patients.
- Tuberculosis Drug side effects: A proactive clinical approach is required to replace/stop the use of the concerned drugs.
- Providing Assistive devices Hearing aids, cochlear implants, tinnitus-masking devices, mobility aids, and prosthetic/orthotic devices improve the quality of life of patients.
- Corrective Surgery: May be required in TB of the bones, spine etc.
- Community and home-based care: This becomes important in severe neuromuscular deficits and movement disabilities.
- Physiotherapy: A trained physiotherapist may help through:
- Sputum clearance technique for reduced sputum quantity, better ventilation and relief of symptoms
- Cough education involving body positioning during coughing, control of breathing in coughing to achieve mobilization and secretions
- Counselling: Psychological support is required for facing long-term/permanent disabilities like loss of vision and hearing loss as side effects of the drugs, paralysis in TB meningitis, infertility in genital TB etc.
- Livelihood options: NGOs and support groups can create such options and/or facilitate treated patients to find various livelihood options
Psychosocial Support to TB Patients
ContentWho can provide Psychosocial support?
Family Members, Peer groups, treatment support groups, TB Champions, Community Health Volunteers(CHVs) and NGOs can provide psychosocial support to TB patients and their families by:
- Building a strong sense of community
- Helping the patients to contact a health worker or visit a health facility
- Providing treatment support to take their drugs and finish their treatment. Family members, community-based volunteers and workers can be trained as treatment supporters by NGOs
- Facilitating patients to access DBT for nutritional support under NPY
- Helping TB patients with comorbidities to visit the referral facility for treatment
- Treatment adherence support through peer support and education and individual follow up
- Home-based palliative care for TB
- Awareness generation, providing right information, behaviour change communication and community mobilisation for reducing stigma and discrimination
- Facilitating patients to join yoga/meditation/exercise groups once the active phase is over
- Facilitating and arranging rehabilitative services for problems/disabilities in TB patients
- Social and livelihood support
- Food supplementation
- Income-generation activities(NGO can start or facilitate patients to join activities like candle making, making festival-related goods)
- Sensitising PRIs to engage TB patients(who can work) through the Mahatma Gandhi National Rural Employment Guarantee Scheme(MGNREGS)
Rehabilitation service to TB patients
ContentThe holistic management of Tuberculosis (TB) patients can improve their life expectancy. The importance of addressing malnutrition, adverse drug reactions, psycho-social well-being, and catastrophic expenses correctly and in a timely fashion is essential in reducing morbidity and mortality.
Table: Rehabilitation services for TB patients Rehabilitation Services for TB Patients Care Providers Key Components Nutritional Rehabilitation 1. Senior Treatment Supervisor
2. TB Health Visitors
3. Accredited Social Health Activists (ASHAs)
4. Auxiliary Nurse Midwife (ANM)
5. TB treatment supporter
6. Medical officers at Peripheral Health Centre (PHC), Community Health Centre (CHC) level
-
Supporting nutritional needs of TB patients through Ni-kshay Poshan Yojana
-
Management of undernutrition in nutrition rehabilitation centres (NRCs)
-
Linkages for extra nutritional support for TB patients like the public distribution system (PDS) or food security act.
Pulmonary Rehabilitation
1.Physiotherapists (preferable one male and one female)
2. Nurses
3. Attendant
Management of physical and psychological impairment due to the disease to lower the handicap. Physical Rehabilitation -
therapists (preferable one male and one female)
-
Nurse Doctors
-
Surgeons
-
Physio
-
Attendant
-
Management of post-treatment sequelae by early identification and periodic assessment.
-
Comorbidity management
Social Rehabilitation 1. TB Health Visitors
2. Accredited Social
3. Health Activists (ASHAs)
4. Auxiliary Nurse Midwife (ANM)
5. TB treatment supporter
6. Medical officers at PHC, CHC level
7. Ni-kshay Mitra
-
Linkage for vocational rehabilitation e.g., Skill India
-
Synergy between social welfare support systems like:
-
Rashtriya Swasthya Bima Yojana (RSBY)
-
TB pension schemes
-
National rural employment guarantee scheme
-
National Health Protection Scheme (NHPS) for palliative care and rehabilitation
Mental Rehabilitation 1. Psychiatrist
2. Psychologists / Counsellors
3. TB Health Visitors
4. Accredited Social
5. Health Activists (ASHAs)
6. Auxiliary Nurse Midwife (ANM)
7. TB treatment supporter
8. Medical officers at PHC, CHC level
-
Psychological counselling to the patient and caregivers.
-
Assisting patients in the planning of decisions related to the end-of-life stage.
Patient rehabilitation is ensured by:
-
1. IT-based monitoring via Ni-kshay platform
-
2. Community-based monitoring
-
3. Surveillance: A comprehensive surveillance system for TB patients and their providers built into eNikshay. This is supported by a call centre for user-friendly private reporting and patient monitoring.
Resource
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Rehabilitation services to TB patients comprise Nutritional, Physical, Pulmonary, Social and Mental Rehabilitation.
False
True
2
The holistic management of tuberculosis (TB) patients can improve life expectancy. The importance of addressing malnutrition, adverse drug reactions, psycho-social well-being, and catastrophic expenses correctly and in a timely fashion is essential in reducing morbidity and mortality.
-
Fullscreen