Drug-sensitive Tuberculosis
ContentWhat is Drug-Sensitive Tuberculosis (DS-TB)?
-
DSTB is a case where a person is infected with TB bacteria that are susceptible to all first line anti-TB drugs. It means that all of the first line TB drugs will be effective as long as they are taken properly and regularly.
-
This type of TB has the best prognosis and the shortest treatment duration.
-
Patients diagnosed with TB are considered to be DS-TB case, till such time s/he detected with resistance to any anti-TB drugs.
Kindly provide your valuable feedback on the page to the link provided HERE
-
Categorization of TB Treatment Regimen
ContentDaily Regimen is prescribed for TB patients, where patients need to consume the medicine daily.
Daily Regimen comprises of the first line Anti TB drugs, based on
- Age: Adult/Paediatric
- Weight of the patient: Weight Bands
Age: Based on the age, patients are categorized into
- Adults: Patient's age should be 19 years or more.
- Paediatrics: Patient's age up to 18 years and weight less than 39 Kgs
Weight Bands:
- Treatment dosage is based on the TB patient’s weight.
- A weight band category is defined for Adult and Paediatric patients separately and medicines are issued based on that weight category.
Treatment Regimen for DSTB – Adult
ContentIntensive Phase(IP): Consists of eight weeks (56 doses) of HRZE in daily dosages as per weight of patient.
Continuation Phase(CP): Consists of 16 weeks (112 doses) of HRE in daily dosages as per weight of patient.
For adults, there are five weight bands, as shown in the table below. The table also indicates the number of FDC tablets that have to be consumed in each weight band
Weight band category
Intensive phase(IP)
(HRZE - 75/150/400/275)
Continuation phase(CP)
(HRE - 75/150/275)
25–34 kgs
2
2
35–49 kgs
3
3
50–64 kgs
4
4
65–75 kgs
5
5
>=75 kgs
6
6
Regular monthly follow up of the patient needs to be done and if patient loses or gains approx. 5 kg weight and if weight band changes during the treatment, then the dose of the patient needs to be recalculated.
Treatment Regimen for DSTB - Pediatrics
ContentIntensive Phase (IP)
Consists of eight weeks (56 doses) of HRZ in daily dosages as per weight of patient.
Ethambutol (E) is given separately for children to monitor ophthalmic side effects.
Continuous Phase (CP)
Consists of 16 weeks (112 doses) of HRE in daily dosages as per the weight of the patient.
In Pediatric, there are six weight bands’s as shown in the table below. The table also indicates the number of FDC tablets that has to be consumed in each weight band
Weight Band category
Fixed-Dose Combinations (FDCs)
Intensive phase (IP)
(HRZE - 75/150/400/275)
Continuation phase (CP)
(HRE - 75/150/275)
4-7 kgs
1 1 8-11 kgs
2 2 12-15 kgs
3 3 16-24 Kgs
4 4 25-29 Kgs
3 + 1A 3 + 1A 30-39 Kgs
2 + 2A 2 + 2A Regular monthly follow-up of the paediatric patient needs to be done and if the patient weight crosses the range of the weight band during the treatment, then the weight band of the patient should be changed immediately.
Children above 39 kg shall usually be adolescents, the drug dosage requirement for them would be similar to adults
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
Adverse Drug Reactions(ADRs) to First Line Treatment
ContentSymptoms
Drug Responsible
Action to be taken by Community Health Volunteers
Gastrointestinal Symptoms
Any Oral Medications
-
Reassure patient.
-
Give TB Drugs with less water at a longer interval.
-
If symptom persists, refer to the nearest health facility
Itching/Rashes
Isoniazid
-
Reassure patient.
-
In case of severe itching, refer the patient to the nearest health facility
Tingling/ burning/ numbness in the hands & feet
Isoniazid
-
Refer the patient to the nearest health facility
Joint Pains
Pyrazinamide
-
Reassure patient.
-
Increase intake of liquids.
-
If severe, refer the patient to the nearest health facility
Impaired Vision
Ethambutol
-
Refer the patient to the nearest health facility
Ringing in the ears, Loss of hearing, Dizziness and loss of balance
Isoniazid, Rifampicin or Pyrazinamide
-
Refer the patient to the nearest health facility
Hepatitis: Anorexia/ nausea/ vomiting/ jaundice
Isoniazid, Ethambutol, Rifampicin or Pyrazinamide
-
If patient detected with signs of jaundice, refer the patient to the nearest health facility
-
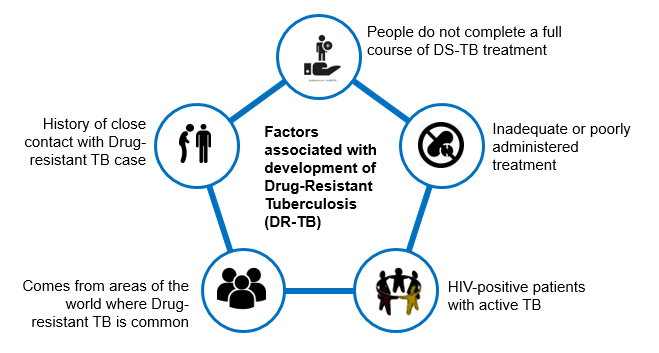
Drug-Resistant Tuberculosis(DR-TB)
ContentWhat is Drug-Resistant Tuberculosis?
-
Drug-Resistant TB occurs when bacteria become resistant to the drugs used to treat TB. This means that the drug can no longer kill the TB bacteria.
-
Multidrug-resistant TB (MDR TB) is a type of DR-TB where TB bacteria is resistant to both Isoniazid and Rifampicin, the two most potent anti-TB drugs.
Figure: High Risk for Drug-Resistant Tuberculosis (DRTB)
Resources:
-
Types of Drug Resistance Tuberculosis -DRTB
ContentResistant Sensitive
Unknown / Sensitive Types of Drug Resistance TB (DR TB) Resistance to Isoniazid (H) Resistance to Rifampicin (R) Resistance to Fluroquinolone (FQ)
- Ofloxacin,
- Levofloxacin,
- Moxifloxacin
Resistance to Group A Drugs
- Bedaquiline or
- Linezolid
H Mono / Poly Drug Resistance
- Resistant to Isoniazid (H)
- Sensitive to Rifampicin (R)
- Unknown / Sensitive to Fluoroquinolone (FQ) or Group A Drugs - Bedaquiline or Linezolid
Rifampicin Resistance (RR)
- Resistant to Rifampicin (R)
- Unknown / Sensitive to other drugs
Multi Drug Resistance TB (MDR TB)
- Resistant to Isoniazid (H) and Rifampicin (R)
- Unknown / Sensitive to Fluoroquinolone (FQ) or Group A Drugs - Bedaquiline or Linezolid
Pre-Extensive Drug Resistance (Pre -XDR)
-
Resistant to Isoniazid (H), Rifampicin (R) and any Fluroquinolone (FQ)
- Sensitive/ Unknown to Group A Drugs - Bedaquiline or Linezolid
Extensive Drug Resistance (XDR)
- Resistant to Isoniazid (H) , Rifampicin (R) and any Fluoroquinolone (FQ) and at least one additional Group A Drugs - (presently to either Bedaquiline or linezolid [or both])
Resources:
DR-TB Treatment Regimens
ContentDepending upon type of drug resistance, there are four broad DRTB Treatment regimen.
- H Mono/Poly Treatment Regimen(6-9 months)
- Shorter oral Bedaquiline containing MDR/RR-TB regimen(9-11 months)
- Shorter injectable containing regimen(9-11 months)
- Longer oral M/XDR-TB regimen(18-20 months)
Drugs administered for DRTB Regimen:
- Drugs are decided based on the drug resistance detected for a patient and will be informed by the medical officer.
- Injections might also be administered to the admitted patient.
- H Mono/Poly Regimen can be initiated at any health facility, while the other two regimen need to be initiated at N/DDR-TB Centre
Figure: Patient wise boxes(PWB) for DRTB Treatment
Pre treatment evaluation of a DRTB cases
ContentLet us understand the objective and importance of Pre-treatment Evaluation (PTE) of Drug-resistant TB (DR-TB) patients.PTE ObjectiveDrugs used for the treatment of drug-resistant TB have significant adverse effects. Hence, there is a need for PTE to rule out any underlying condition at the baseline, like co-morbid conditions, radiological abnormalities, Electrocardiogram (ECG) changes, or biochemical derangements.PTE is essential to identify:- The patient's eligibility for initiation of a particular regimen
- Patients who require special attention during treatment
- Regimen modifications from the beginning of treatment
Important Points
- In the majority of Multidrug-resistant (MDR)/ Rifampicin-resistant Tuberculosis (RR-TB) patients, PTE can be done on an outpatient basis.
- The District TB Officer (DTO) and Medical Officer of the TB Unit (MO-TU) can arrange for PTE at the Nodal and District DR-TB Centre (N/DDR-TBC) or at the sub-district level health facility, wherever feasible.
- No additional investigations are required for H Mono/ Poly DR-TB patients unless clinically indicated.
- The PTE carried out at the time of treatment initiation can be considered valid for 1 month from the date of the test result and the patient can be re-initiated on a subsequent regimen considering the previously conducted PTEs.
- Active Drug Safety Management and Monitoring (aDSM) treatment initiation forms are required to be completed for all DR-TB patients at the time of initiation of each new episode of treatment.
- PTE should include a thorough clinical evaluation by a physician and expert consultation as per the need.
- Laboratory-based tests should be performed based on the drugs used in the treatment regimen.
- Pre-treatment evaluation should be made available free of charge to the patient.
Resources
- Guidelines for Programmatic Management of Drug-resistant Tuberculosis in India, March 2021.
- WHO Consolidated Guidelines on Tuberculosis: Module 4 -Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
Second Line anti TB drugs
ContentThe anti-TB drugs recommended for treatment of Multi- and Extensively Drug-resistant (M/XDR) TB patients are grouped into three groups – A, B and C (Figure below).
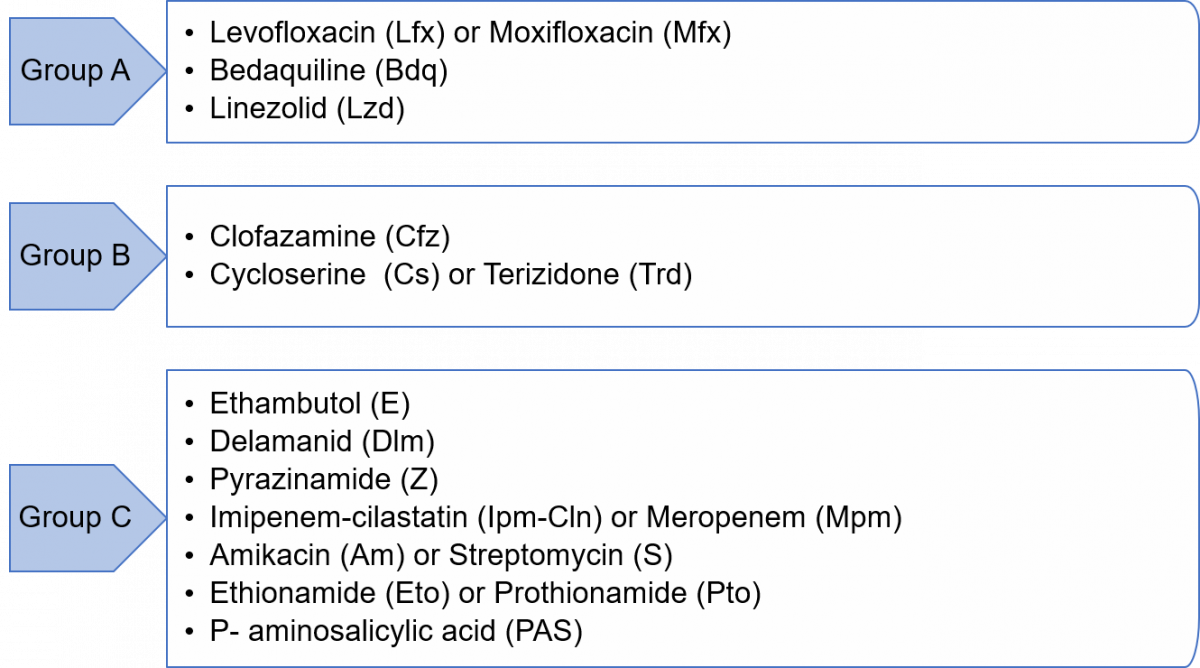
Figure: Groups A, B and C of Anti-TB Drugs used in Treatment of M/XDR-TB Patients
Grouping of drugs is done based on their efficacy, experience of use and drug class. This grouping is intended to guide the design of individualized, longer M/XDR-TB regimens (the composition of the recommended shorter MDR/RR-TB regimen is largely standardized).
Resources
- Guidelines for Programmatic Management of Tuberculosis in India, 2021.
- WHO Consolidated Guidelines on Tuberculosis, Module 4 - Treatment: Drug-resistant TB Treatment, 2020.
Kindly provide your valuable feedback on the page to the link provided HERE
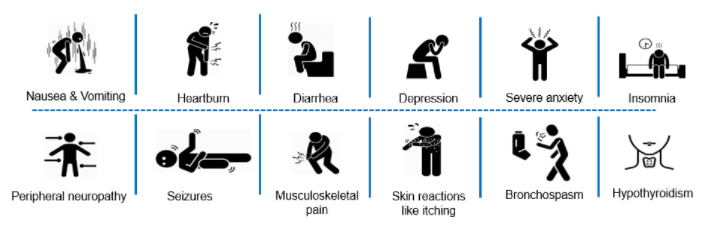
Adverse Drug Reactions(ADRs) to Second Line Treatment
ContentCommon Adverse events to second line treatment are as below
Figure: Adverse Drug Reaction to Second line drugs
Adverse events should be identified, monitored and be referred to
- Nearest treating doctor for minor symptoms or
- District DR-TB Centres for major symptoms
If required, hospitalization can be done at the District DR-TB Centers where inpatient facility is available or referred to a Nodal DRTB Centre for admission
Fullscreen