-
Ch 29: Stigma, Discrimination and Gender sensitivity
FullscreenStigma and Discrimination towards TB Patient
ContentStigma is when someone sees you in a negative way.
Discrimination is when someone treats you in a negative way.
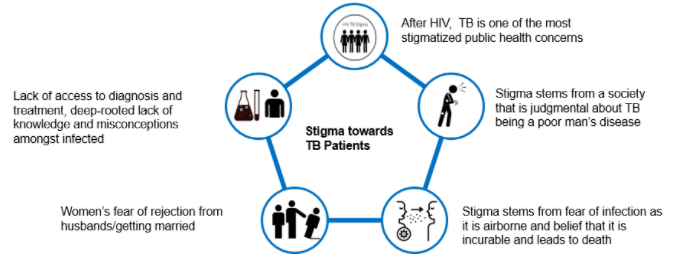
TB patients face various forms of stigma and discrimination in the community
Figure: Stigma towards TB Patients in the community
Effects of Stigma on TB Patients
ContentAt Individual Level
- Lack of self-esteem and confidence
- Increased sense of emotional isolation, feeling of guilt and anxiety
- Physical as well as financial debilitation
- People, more often women, are forced to leave their homes
- Concealing symptoms and hesitancy in seeking medical care making disease management more difficult
- Delayed diagnosis, interrupted treatment that can lead to further transmission and DRTB
- Vulnerability increases, can lead to suicidal thoughts due to isolation and shame
At Family and Community Levels
- Loss of household earnings
- Exposure of caregivers to the risk of infection that lowers productivity and cycle of poverty further gets perpetuated
- Isolation and stigmatization of infected persons often by people of their community
- Deep-rooted lack of knowledge and misconceptions among the affected and infected within their cultural and religious environment
- Loss of status and negative impact on those with the disease, their caregivers, family, friends and communities
- Perceived and internalized stigma of the community due to socio-cultural values that TB is punishment for sins or transgression
Gender Aspects of TB
ContentAlthough more men are affected by TB, women and transgender persons experience the disease differently. Gender differences and inequalities play a significant role in how people of all gender access and receive healthcare services.
Gender difference in Men Women Incidence of TB - Higher proportion of men(approximately- 2:1) are diagnosed with TB than women
- More likely to have microbiologically confirmed Pulmonary TB
- More likely to have Clinically diagnosed pulmonary TB and extra – pulmonary forms of TB
- Prevalence of HIV-TB co-infection is higher among women who live in overcrowded houses and consume alcohol
- High Risk for developing TB – Pregnant women and women in the postpartum period
Exposure, Risk & Vulnerability - Smoking and alcohol consumption among men
- High risk for developing TB - employment in mining, quarrying, metals and construction industries
Undernutrition, their role as caretakers and the use of solid fuel for cooking puts women at risk for TB Health Seeking & Health system factors - Fear of loss of income and the consequences of absence from work hinder care seeking.
- Women face difficulties due to perceived stigma, prioritization of household chores, lack of money or financial dependence
Treatment Outcomes - Pressure to get back to work and lifestyle habits such as smoking or consumption of alcohol influence discontinuation of treatment in men
- Migrant workers, mostly men, often face difficulties in adherence to treatment in the face of extreme poverty and issues of daily survival
- Women tend to have better adherence and treatment outcome as compared to men
- Stigma and discrimination are major impediments to treatment adherence, mainly among unmarried women, newly married women and the elderly
Transgender population often has low literacy, low education levels and are poor. A high proportion of transgender persons are known to smoke, consume alcohol and use drugs. All these factors make them vulnerable to TB.
Addressing Gender Inequalities
ContentBroad principles to address gender inequalities in TB care
- Confidentiality of patient needs to be maintained
- Non-discrimination and non-stigmatising behaviour to be promoted
- Respect for all to be ensured
- Informed consent and informed treatment
- Accountability to be fixed for actions and inactions
- Access for all health services
- Rights-based approach
- Empowered communities - Ensure representation of women, men and transgender persons in all forums
- Work in partnership - Strengthen linkages between program, private sector and communities
-
Ch 30: Counselling for Collecting Sputum Specimen
FullscreenObtaining Induced Sputum
ContentInduced sputum is considered in a situation where a person is unable to provide sputum sample in sufficient quantity for Tuberculosis (TB) diagnostic test. This situation is more evident in children.
- Sputum induction is usually done using 3% nebulized hypertonic saline.
- The patient is pretreated with nebulized bronchodilators like salbutamol prior to induction.
- Following saline nebulization, chest physiotherapy is done to loosen up the secretion and the samples are collected from the throat or nasopharynx using a collector attached to a suction at one end and a catheter/ tube to the other.
- The suction catheter provokes cough and the secretions brought up are collected via suction.
Sputum Induction has to be carried out only in a clinical setting under the close supervision of a trained medical practitioner.
Resources
Kindly provide your valuable feedback on the page to the link provided HERE
-
Ch 31: Communicating Results to the patient
FullscreenNeed to communicate results to patient
ContentIt is important that patients receive their positive/negative test results and an adequate explanation of the results in a timely manner.
Time required for different Laboratory test results include:
1. Smear microscopy/follow up:1 day
2. Nucleic Acid Amplification Test (NAAT) (CBNAAT/Truenat):1-2 days
3. Line Probe Assay (LPA): 2-3 days
4. Liquid Culture DST (Drug Susceptibility testing): 22-48 days
Results of all laboratory tests such as smear, culture and DST / LPA / NAAT should be entered in Nikshay by the testing facility
Communicating test results
Communicating test results to the patient provides an opportunity to discuss about TB disease, its prognosis and treatment options.
It also includes counselling and educating patient and family members on need for regular treatment, cough etiquette and proper disposal of sputum to prevent transmission of disease.
It is important that:
- All results should be communicated to the concerned health facility through Nikshay as soon as results are available
- Alternative means (email, SMS etc) are also used to communicate the test results
- Test results once available, should be promptly communicated to the patients by NTEP supervisors/general health system staff/community volunteers within 1-2 days
- It is essential that laboratory technicians record the complete addresses of patients examined for diagnosis. This facilitates tracing and initiation of treatment for all diagnosed TB cases
- All patients whose test report is positive should be provided information on TB disease, TB treatment and counselled for early treatment initiation. Emphasis should be made on starting the treatment at the earliest in order to prevent further transmission of disease .
- The primary caregivers and other household members of the patient should be counselled for matters related to patient’s TB treatment, cough hygiene, risk of spreading infection, nutrition and also address issues related to gender, stigma, discrimination or any other psycho-social issues (if any, related to TB diagnosis) that could impact treatment initiation.
- For those patients whose test report is negative (active TB ruled out), they should be further tested for TB infection (TBI) and on confirmation of TBI, their eligibility for TB preventive treatment (TPT) should be assessed and necessary action should be taken, if eligible.
- For those patients who do not have TB disease nor TB infection, negative test result also needs to be communicated. Broad spectrum antibiotics are prescribed to them for 10-14 days. Most patients are likely to improve with a course of antibiotics if they are not suffering from TB.
- If the symptoms persist after the course of antibiotics, the patient is re-evaluated by repeat sputum and X-ray examination and decision to treat accordingly is made by the treating physician.
Resources
- Training Modules for Programme Managers and Medical Officers
- Module for Senior Treatment Supervisor
- Guidelines for PMDT in India, 2021
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test Who conveys the results of TB tests to the patient? NTEP supervisors General health system staff
Community volunteers All 4 Results of TB tests are communicated to the patients by NTEP supervisors, general health system staff and community volunteers. Yes Yes Test results are communicated to patients by NTEP supervisors within how many days?
2 days 4 days 6 days 8 days 1 Test results once available, should be promptly communicated to the patients by NTEP supervisors/general health system staff/community volunteers within 1-2 days Yes Yes How to communicate results to TB patient
ContentWhen the referring health facility receives the test results from the DMC, the results are communicated to the patient through NTEP supervisors/health facility staff/Medical Officer.
Both Positive and negative results need to be communicated to the patient. For negative results, counselling for further evaluation and testing need to be done for the symptoms.
Communication as a tool embodies attitudes, behavior, body language, style, method of presentation, quality of listening and perceptions and interpretations.
It is important that the health staff communicating TB test results to patient is trained in interpersonal communication (one-to-one) and soft skills (listening, motivating, problem solving etc).
The results are communicated in a polite and non-authoritarian manner that encourages open communication and builds rapport with the patient
Resources
- Training Modules (5-9) for Programme Managers and Medical Officers, NTEP, 2020
- Module for Senior Treatment Supervisors (STS): Ensuring Proper Treatment, Registration and Reporting, CTD, 2005.
- Guidelines for PMDT in India, NTEP, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
The Peripheral Health Worker (PHW) should visit the house of the patient (within a week) to communicate results to the patient.
True
False
1
The Peripheral Health Worker (PHW) should visit the house of the patient (within a week) to communicate results to the patient.
Yes
Yes
-
Ch 32: Counselling the TB patients
FullscreenTB Awareness Generation in Community
ContentAwareness should be generated in the community for promoting various health programmes, health seeking behaviours, screening of TB cases etc. by involving and sensitizing community influencers including PRI members and treatment support groups.
Figure: Activities for awareness generation in community
Counselling for TB treatment initiation
ContentCounselling before initiating treatment for a patient. is an important component of the National TB Elimination Programme (NTEP). The patient is counselled along with his family by the health staff.
Counselling is done on the following points:
- Health education on TB and its symptoms
- Mechanism of TB transmission
- Infection control measures, like cough etiquette and sputum disposal
- Nature and duration of treatment
- Importance of adherence to treatment and the need for complete and regular treatment
- Possible side effects of drugs
- Consequences of irregular treatment or premature cessation of treatment
- Nutritious diet
- Nikshay Poshan Yojna
Communication tools
1. Communication is provided through interpersonal communication in one-to-one sessions and by use of Information, Education and Communication (IEC) materials like posters, pamphlets, flip charts, etc.
2. Arogya Sathi App: The app empowers TB patients to proactively increase their awareness of TB by addressing Frequently Asked Questions (FAQs) regarding TB and information on the symptoms of TB and side-effects of anti-TB drugs. It also helps them in accessing their treatment details, DBT details and adherence calendar.
3. Nikshay Sampark: National TB call centre "Nikshay Sampark" toll-free helpline number 1800-11-6666 can be contacted anytime by patients and their families to resolve concerns and issues faced by TB patients.
Resources
- Training Modules (1-4) for Programme Managers and Medical Officers, NTEP, 2020.
- Guidelines for PMDT in India, NTEP, 2021.
Assessment
Question
Answer 1
Answer 2
Answer 3
Answer 4
Correct answer
Correct explanation
Page id
Part of Pre-test
Part of Post-test
Nikshay Sampark can be used as a communication tool to resolve concerns and issues faced by TB patients.
True
False
1
Nikshay Sampark can be used as a communication tool to resolve concerns and issues faced by TB patients.
Yes
Yes
Counselling for regular follow-up during the treatment
ContentThe continuum of counselling and care is essential to constantly motivate TB patients to take their full drug regimen and complete it in due course.
Counselling is regularly given by counsellors, treatment supporters and all those involved with patient care and treatment.
Counselling should start at the initial point of contact as soon as the diagnosis is established and continued during all visits:
- By the patient to a health facility
- By healthcare workers’ visit to the patients’ home
- Through the national TB call centre (Nikshay Sampark)
Key Points for Counsellors:
- Counsellors must inform patients that regular monthly follow-up during their treatment is important to understand their TB treatment response and to determine if they have been cured.
- During these monthly follow-up visits, TB patients should be screened for any clinical symptoms and/or cough. If found positive on screening, then sputum microscopy and/or culture should be considered. This is important to detect recurrence of TB as early as possible.
- Counsellors should inform patients of the follow-up schedule, and follow up, via physical visits or telephone calls, with patients to verify that they have gone for their follow-up visits at these times:
a. Clinical evaluation at the end of every 4 weeks of treatment
b. Sputum examination at the end of each treatment phase i.e., intensive and continuation phase
c. Long-term post-treatment follow up: Sputum examination, at an interval of 6 months, 12 months, 18 months and 24 months, and if suspected, referred for testing again.
A counselling register is maintained for all patients for recording information about the patients’ situation and counselling services provided from the time of diagnosis till post-treatment follow-up period.
Information to be Provided to Patients During Regular Monthly Follow-up
- Nature and duration of treatment
- Need for regular treatment/adherence
- Information on the lab results, and the reliability of lab results
- Consequences of irregular treatment or pre-mature cessation of treatment
- Possible side effects of anti-TB drugs and management of side effects
- Nutritional counselling (Nikshay Poshan Yojna)
- Services under National TB Elimination Program (NTEP) and linkage to social protection schemes
- Infection control precautions that are necessary, and re-assurance to the family against panic or unnecessary stigmatization of the patient
Resources
Guidelines for PMDT in India, 2021
Assessment
Question Answer 1 Answer 2 Answer 3 Answer 4 Correct answer Correct explanation Page id Part of Pre-test Part of Post-test During the monthly follow-up visits during TB treatment, patients should be screened for any clinical symptoms and/or cough. True False 1 During the monthly follow-up visits during TB treatment, patients should be screened for any clinical symptoms and/or cough. Yes Yes Counselling of TB Patients
ContentConfidential dialogue between a health care provider and a patient that helps a patient to define his/her feelings, cope with stress, and to make informed decisions regarding treatment.
The patient should be counselled at all the three phases i.e.,
Pre-treatment counselling`
- About TB disease and treatment
- Air borne infection control
- Need for adherence
- Public Health Actions
- Identification of adverse events
- Tobacco /Alcohol cessations
- Identification of comorbidities
During Treatment Counselling
- Importance of Adherence
- Identification of adverse events
- Importance of timely follow ups
- Public Health Actions
- Tobacco /Alcohol cessations
- Management of comorbidities
Post treatment Counselling
- Testing at the end of treatment.
- Long term follow up
- Tobacco /Alcohol cessations
Objectives of TB Counselling:
- Prevention of TB transmission.
- Provision of emotional support to TB patients.
- Motivation of TB clients to complete treatment.
- Helping patients make their own informed decisions about their behaviour and supporting them in carrying out their decisions.
Figure: Characteristics of effective counselling
Do's & Don'ts for Patient Communication
ContentDo’s
- Active listening, emphatic gestures and expressions
- Ensure the confidentiality of the conversation done with the patient
- Ensure Minimum interruption during the conversation with patient
- Ensuring availability of IEC materials such as posters, videos, pamphlets etc. to dispel myths and misconceptions.
Don'ts
- Do not use any negative stereotypes
- Do not have any physical wall or glass between patient and yourself
- Do not breach the trust and confidentiality of the TB patient
- Do not make threats or use coercive language
- Do not exaggerate dangers or risk of TB
- Do not blame or shame TB patients
Nutritional Counselling
ContentNutritional Counselling begins with the nutritional assessment of TB patients by
-
Nutritional Status: Assessing the height, weight and BMI of the TB patient
-
Diet and Preference food for TB patients
-
Current appetite and food intake of TB patients
Based on the nutritional assessment, following information can be conveyed to TB Patients
-
Patients with TB should be encouraged to have frequent food intake in the form of three meals and three snacks.
-
Attempts should be made to increase the energy and protein content in the meals and snacks without increasing its volume.
-
The addition of oil, butter or ghee to the chapati or rice can increase the energy content of the diet.
-
Pulses in other forms, e.g. sprouts, roasted Chana, groundnuts, can be taken as snacks in either fried or in roasted form. Milk and eggs to be included in the diet.
-
The use of easily available nutritious foods based on vegetarian/non-vegetarian preferences of the patients must be emphasized.
-
Information about NFSA (National Food Security Act) and Poshan abhiyan should be given.
Figure: Healthy diet for TB Patients
Resources:
Kindly provide your valuable feedback on the page to the link provided HERE
-
Fullscreen